
tags: bipolar disorder, manic depression, mental illness, psychiatry, psychology, children
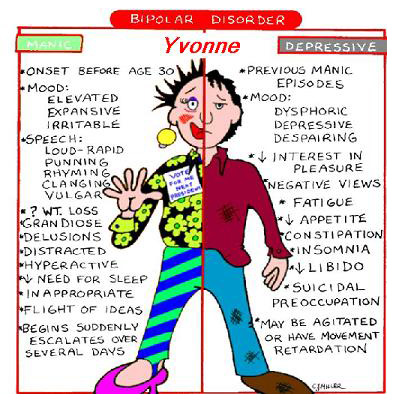
Image: Myself43.
If you are like me and suffered from unrecognized bipolar disorder as a child only to later have this mood disorder diagnosed upon reaching young adulthood, you might be pleased to learn that current research suggests bipolar disorder is increasingly being diagnosed as beginning in childhood. As a result, these bipolar kids are more likely to receive proper treatment and support such that they, their families and friends will suffer fewer of the deep emotional and social scars that can result from untreated bipolar disorder.
Bipolar disorder, historically known as manic depressive illness, is a serious psychiatric condition characterized by sudden and unpredictable mood swings between a state of euphoria, or mania, to paralyzing depression. This is the more serious "classical" form of the disorder, known as bipolar disorder, type 1. Type two differs from type one because a person's moods only shift between depression and a much milder form of mania known as hypomania. Between mood swings, most people with bipolar disorder are symptom-free. However, people with bipolar disorder have a strong risk for suicide, particularly when they are experiencing mood swings. This mood disorder has long been known to have a strong genetic component, because it typically runs in families.
Until recently, the psychiatric paradigm was that bipolar disorder did not manifest itself until a person reached young adulthood. However, current research has been increasingly calling this into question since children as young as six years old appear to show at least some symptoms of bipolar disorder.
On the other hand, skeptics claim that bipolar disorder is being increasingly diagnosed in children either because bipolar disorder is the mental illness du jour or because of diagnostician confusion. For example, aggression or irritability -- typical to bipolar disorder -- are also characteristic of several other conditions such as attention-deficit hyperactivity disorder.
Thus, the challenge is to recognize and corretly treat bipolar disorder in children so its social and psychological effects can be limited.
"Children don't get married four times, or max out their credit cards, or buy real estate they can't afford," said Dr. Barbara Geller of Washington University in St. Louis, who led the study. "We have to find the childhood equivalent of these behaviors."
To do this study, Geller and her colleagues included grandiosity in addition to irritability or aggression as their study selection criteria that marked mania in children. Grandiosity, a common adult symptom of bipolar mania, is observed in children who engage in dangerous high-risk behaviors such as such as running into traffic because of a sense of invincibility.
After defining their diagnostic criteria, Geller and her colleagues identified and studied 115 children between the ages of 7 and 16 whom they diagnosed with bipolar disorder type one because they had or were suffering either with mania or a mixed state. A mixed state is characterized by both depressive and manic symptoms.
The children visited Geller and her colleagues at the start of the study and then for 9 follow up visits over eight more years. The team separately interviewed the children and their parents about the child's symptoms, diagnoses, daily cycles of mania and depression, and interactions with others. One hundred and eight of the children completed the study.
During the ensuing eight years, Geller and her colleagues found that the children spent 60.2% of their weeks with some number of mood episodes, and 39.6% of the weeks with some episodes of mania. In total, 87.8% of Geller's patients recovered from mania (figure 1);

However, nearly all (73.3%) of these bipolar children later relapsed with another manic or mixed state episode. Second and third episodes of mania in the children included psychosis, cycling between mania and depression, and were of long duration. For example, on average, the length of a second manic episode was 55.2 weeks and the average length of a third episode was 40 weeks. Further, the team found that the relapse rate in bipolar children was strongly influenced by maternal warmth (figure 2);

Of the 54 children who reached 18 years of age or older at the end of the study period, 44.4% continued to experience manic episodes, which is a rate that is much higher than for the general population. In this group of young adults, 35.2% developed substance abuse, a rate that is similar to people who are diagnosed with bipolar disorder as adults. The team says these findings indicate that there may be significant continuity between childhood and adult bipolar disorder.
"Children with mania grow into adults who have mania," observed Dr. Geller.
The team concluded their paper by writing that this study emphasizes the need for further research into diagnosing and treating childhood bipolar disorder.
"In conclusion, mounting data support the existence of child bipolar disorder I, and the severity and chronicity of this disorder argue strongly for large efforts toward understanding the neurobiology and for developing prevention and intervention strategies."
As an adult who suffered from an unrecognized bipolar type I disorder from childhood, I strongly agree with Dr. Geller and her colleagues, particularly since my own mood disorder was instrumental in destroying both my childhood and my relationship with my family.
Source
Barbara Geller, MD; Rebecca Tillman, MS; Kristine Bolhofner, BS; Betsy Zimerman, MA (2008). Child Bipolar I Disorder: Prospective Continuity With Adult Bipolar I Disorder; Characteristics of Second and Third Episodes; Predictors of 8-Year Outcome Archives of General Psychiatry, 65 (10 ), 1125-1133 [free PDF].
- Log in to post comments
Interesting paper. I have never really examined my childhood and looked for BP symptoms. I was never really manic until my mid-twenties. I had problems with depression, but that could have been due to my living conditions.
Earlier diagnosis is definitely good. It reduces suffering for one thing. There was a school of thought that earlier treatment can reduce odds of the BP progressing to a more severe form, but I don't know what current research says.
yes, there are some clinicians who do think that treating bipolar disorder early in childhood might prevent it from progressing into a more serious form. but the skeptics think that those kids whose symptoms were treated and never worsened never really had bipolar disorder at all. however, it is difficult to know the answer to this question until we have a good genetic test that will identify bipolar disorder and can help discover the genetics underlying the condition -- perhaps certain genetic aspects associated with bipolar disorder are more likely to be "curable" through early treatment than others?
Is it possible to live in a constant mixed state?
I've never learnt much about bipolar disorder, but skimming your article one thing that strikes me is the length of the "high" and "low" periods. You get this vague impression from the media that they are shortish, perhaps on the order of single-figure weeks. But your article puts them more on the order of months.
I might be reading this wrong, as I haven't the time to read the paper or even digest the even figure 2 legend. (I'm bit confused as to what a couple of the terms precisely refer to without reading the paper itself.)
bipolar disorder suggests that moods change over time, so it's very very unlikely that a person can stay in a mixed state permanently. further, people in mixed states have the highest suicide risk, so this is really a bad place to be for an extended period of time (i should know, since this state is fairly typical for me!)
a particular mood can last months or years for most people with bipolar disorder, but some people experience rapid mood cycles, as i do. which means that they can go from despair to elation over a period of hours and then, a week or a month later, they can once more be depressed. no fun!
It strikes me that if the range of length of states is that great, you'd have to think very carefully about how you work with the results. (I'm thinking about the stats.)
I presume that a "mixed" state is distinct from rapidly switching from mania to depressive, so that "mixed" would mean symptoms of both at the same point in time as opposed to separate "states" within a short period of time? Splitting hairs, maybe?! (Figuratively, not literally!)
DeafScientist: IIRC, a cycle length of less than 24 hours is generally considered as "mixed state". The cycle length varies widely between individuals, from years down to... well, down to mixed state. (I've forgotten at what point it's considered "rapid cycling". Less than a year?)
Also: one very experienced PsyPharm I knew described mixed state as "among the most unpleasant conditions possible to a human being". So, long-term and continuous... yeah, I'd agree with GS, it's not very survivable.
Another psypharm commented to me that a lot of Bipolar folks never really get to "enjoy" periods of normality, because they spend those times trying to rebuild their lives from the havoc created by their last manic episode....
a mixed state is accompanied by very rapid fluctuations between deep despair and intense anxiety, hyperactivity, and irritability. one feature that remains consistent throughout these mood changes is the inability to concentrate on anything at all. when i am in a mixed state, i cannot remember what day it is, where i am, whether i've eaten recently (and i often cannot keep food down anyway), and i certainly cannot concentrate long enough to watch TV or read a book -- not even one sentence -- and remember what i've read. to put it mildly, living like this for weeks or months at a time is enough to drive anyone to suicide, and worse, they are energetic enough to do it, too. this is the reason that a mixed mood state is the most dangerous of all.
Thanks for that. I was a bit confused what "mixed" might mean!
I tend to forget to eat, but I'm sure that's a more normal failing of most scientists, y'know... getting myopically distracted once they start working... :-/
(Actually, my budget is small enough I'm working of one "proper" meal a day and occasionally not quite that. No need to ask me what I think of academic funding systems... Anyway, reminds me to stop this and get something to eat!)
Do many/some people experience short "bursts" of this type of thing in an otherwise "normal" life--? Or are these considered completely unrelated?
Rats (or should that be "Parrots"?), 'off' for 'of' in line 4. Couldn't cancel the post in time...
i am not an expert about what normal people might (or do) experience, so i don't know what to tell you.
Thanks for that.
Wayyy off topic, have you see "Psycology's pet subject" in the latest edition of Nature? I'm not sure if you have access to this, but its a review of Pepperberg's book "Alex & Me". I can imagine it'd appeal to you, perhaps.
*Sigh* 'seen' for 'see', right?!
Um, maybe I'm in the minority here, but it struck me as quite humorous that it could appear to be an epiphany that bipolar children are likely to become bipolar adults. Isn't that like saying "male children are likely to become male adults"?????? Well DUH! Obese children are likely to become obese adults, red headed children are likely to become red headed adults, mean spirited children are likely to become mean spirited adults...am I missing the real point, or just the only one pointing out that the emperor really isn't wearing anything at all?
Thanks for writing about this. At first it seems like a "Duh!" because biochemistry is biochemistry, right? I didn't know it was an issue based on an assumption. And I didn't know that symptoms would be different. So thanks for educating me.
Thanks for submitting this post to our blog carnival. We just published the 41st edition of Brain Blogging and your article was featured!
Thank you.
Sincerely,
Shaheen
im writing cause i might have bipolar disorder. are there any sites for this