
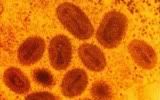
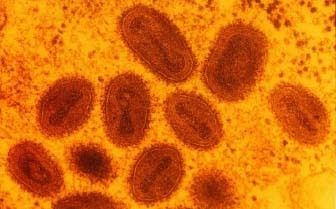
 Smallpox is, without a doubt, the biggest success story in all of vaccination. The practice of variolation, or the purposeful inoculation of naïve individuals with material from scabs of smallpox victims, was practiced for years prior to Edward Jenner's substitution of cowpox for the smallpox (Variola) virus. The vaccinia virus, thought to be a derivative of cowpox, has been used in the 20th century in smallpox vaccination campaigns. Vaccina elicits antibodies that protect from smallpox infection, yet typically causes an asymptomatic or only mildly symptomatic infection. This worldwide effort led to the last known naturally-occurring case of smallpox, which occurred in 1977 in Somalia. (The last known U.S. case dates back to 1949). However, in the aftermath of 9/11 and fears over the use of bioweapons, the U.S. military instituted the controversial smallpox vaccination program, as part of the Department of Defense's "national strategy to safeguard Americans against smallpox attack." To date, over a million service people have been vaccinated. This program has been in the news several times recently, as vaccinia infections have spread beyond the vaccinated individual and to family members and now, sexual partners. More after the jump.
Smallpox is, without a doubt, the biggest success story in all of vaccination. The practice of variolation, or the purposeful inoculation of naïve individuals with material from scabs of smallpox victims, was practiced for years prior to Edward Jenner's substitution of cowpox for the smallpox (Variola) virus. The vaccinia virus, thought to be a derivative of cowpox, has been used in the 20th century in smallpox vaccination campaigns. Vaccina elicits antibodies that protect from smallpox infection, yet typically causes an asymptomatic or only mildly symptomatic infection. This worldwide effort led to the last known naturally-occurring case of smallpox, which occurred in 1977 in Somalia. (The last known U.S. case dates back to 1949). However, in the aftermath of 9/11 and fears over the use of bioweapons, the U.S. military instituted the controversial smallpox vaccination program, as part of the Department of Defense's "national strategy to safeguard Americans against smallpox attack." To date, over a million service people have been vaccinated. This program has been in the news several times recently, as vaccinia infections have spread beyond the vaccinated individual and to family members and now, sexual partners. More after the jump.
This past March, reports surfaced regarding a 2-year-old Indiana boy. His father was in the Army, and had recently received his smallpox vaccination. The vaccinia virus contained in the vaccine is a live virus; therefore, it is capable of replication in the recipient, and potentially of spread to others. This is exactly what happened in this case. The father sread it to his son, who developed a rare side effect: eczema vaccinatum, essentially a crusty skin rash caused by the virus in those who already suffer from eczema. In the boy's case, the rash eventually spread over 80% of his body, and the condition can be life-threatening. (Indeed, the boy was on a ventilator for a time, and doctors predict he'll lose up to 20% of his outer skin layer). The boy's mother also contracted the virus, although a much milder case than her son.
Now, just this week comes a report of sexual transmission of vaccina virus. An Alaskan woman and another U.S. soldier engaged in "manual stimulation and vaginal intercourse" three days after the soldier had received his smallpox vaccination. A month later, the woman reported to her doctor with vaginal sores. As her symptoms worsened and were unresponsive to treatment, doctors took swabs from the lesions and submitted them to both the state health department and the CDC, who determined the virus present in the swabbed material was a match to vaccinia.
While these are only two cases out of over a million vaccinated, they are instructive in that both could probably have been prevented. Eczema is one risk factor for development of severe illness after vaccinia infection; therefore, vaccine recipients themselves are questioned about history of eczema, and are reportedly cautioned about avoiding others who are known to have a similar history post-vaccination. The newspaper article says that the child was known to have such a history; therefore, his father should have been cautioned to stay away from him in the days following vaccination. Whether he wasn't told, or simply didn't understand and/or pay attention isn't known, as far as I could tell.
With the second case report, contact vaccinia is much more common than the serious eczema vaccinatum that the boy developed. However, this also could have been prevented with more information. The Morbidity and Mortality Weekly Report (MMWR) write-up states:
Since March 8, 2007, CDC and the U.S. Department of Defense have received reports of four instances of nongenital contact vaccinia associated with recently vaccinated service members, including two cases from Indiana and one case each from Alabama and New Mexico.
and the CIDRAP article states:
According to the US Department of Defense (DoD) Web site, 61 cases (36 lab-confirmed) of contact vaccinia occurred, mainly to spouses and adult intimate contacts, between Dec 13, 2002, and Apr 12, 2007.
This suggests that more education, with a stress on avoidance of close contact in the post-vaccination period, could have prevented these cases.
In the broad scope of things, these really are only a handful of cases, particularly given the large number of servicemen and women who've been vaccinated to date. However, as vaccinia requires close contact to efficiently spread, an emphasis on these cases and the need to keep a bit to one's self in the post-vaccination period is something that simply doesn't hurt to emphasize. It also has served to cause those exposed to question the need for a vaccination program in our military, since smallpox is one of the few pathogens where post-exposure vaccination can still stop the onset of disease.
Image from http://www.humanillnesses.com/original/images/hdc_0001_0003_0_img0246.j…
{kind=link}
- Log in to post comments
I've read through this thread and come to an undisputable conclusion. I'm sure all will agree.
The folks here are rabid cunts. You'll forgive the epithet.
But it's true. I mean, the "How dare you sirs!" and "Do you bother to read?" and "Ho hum, sigh, the denialists are at it again!"
Well, they earn you the title, "Cunt". As in,
You're really such a bunch of vicious, dishonest, cunts.
And,
What a bunch of psychopathic cunts you are.
Good expression, cunt.
I think it describes a way of being that is in effect throughout this blog, in response to the overly-long, but quite brilliant posts of Dr. Maniotis.
I know none of you will answer any question honestly. You are maniacs, losers, vicious scumbag bastard nazi racist, eugenicist shitheads. And I know you'd prefer to round up and exterminate anyone who disagrees with you - you show your fangs in every trite, snarky, bullshit response.
I can't help but to feel that the men in this group are graduates of the little-lord-fauntleroy school for hemophiliac mother's-little-angels. And the women...I already said it. Vicious cunts. Really, and that goes double for Jeffries. (you dirty little thing, who knows what you're up to at home?)
Look, history will have it's say. And I think it will pin the title of 'great big fucking cunt' on the losers in this bin. I mean, it would, but I don't think anyone will remember a single one of you.
So, good luck, losers. Keep sucking each other's tiny wangs for luck. You haven't got a shred of decency, and I'm sure most of your friends fear and hate you.
But you wouldn't have it any other way.
This is a classic example of the paradox of vaccination: when do you stop vaccinating because the risks outweigh the benefits?
We had the honor of having Donald Henderson, who led the campaign to eradicate smallpox, give a talk here a few years ago. You would not want to go back to those days. After 9/11 and the 10/4 anthrax attacks there was a lot of real concern about smallpox, but does the military really need to keep up this vaccination program now? Would it not be more sensible to stockpile the vaccine, in case it ever is needed, preferable in multiple locations?
It's probably worth noting that, first, as vaccines go vaccinia has an extremely high rate of side-effects - much higher than almost any other vaccine in common use. If smallpox wasn't such a fearsome disease, vaccinia wouldn't have been used. And second, there's still considerable research on developing safer smallpox vaccines. A lot of it is working on making attenuated versions of vaccinia that are still immunogenic.
Unfortunately, the smallpox vaccination campaign was begun with political spin posing as a scientific decisionmaking process--not untypical of the kind of information our current administration often uses for its decisionmaking process.
Vaccinia was an excellent vaccine for eliminating smallpox. There was no good reason to start vaccinating all of us against it, or even our troops. But as he and his lot built the case for weapons of mass destruction in Iraq, Cheney either became convinced or pretended to become convinced that Iraq had smallpox stores. He pushed the CDC's advisory committee into recommending that 10 million Americans get the vaccine (only 40,000 civilians did).
There was some circular reasoning at work here. If Saddam was evil enough to be stockpiling smallpox, he was evil enough to invade. If he was evil enough to invade, he must be stockpiling smallpox. The evidence? We had decided to start vaccinating against it--which we wouldn't have done if it wasn't a real threat, right? This was a hall of mirrors. DA Henderson initially fed the flames though he has since said there was never any evidence that Iraq had the stuff.
It's worse, isn't it? With 40,000 civilians vaccinated, isn't there that much more chance someone we don't want to have real smallpox could get some? It's like telling a thousand people to keep a secret. [make up some embarassing secret and publish it here].
They say you're much more likely to be shot if you own a gun.
So which came first: the word vaccination, or vaccinia?
Stephen,
The vaccinia virus is not the disease virus. It will give you immunity against the disease, and it's a real virus, but it's not smallpox (variola). Vaccinia can spread, but only rarely and by direct contact like Tara says. Variola spreads by direct contact and can also be airborne.
Which word came first?
Well, they both come from 'cow' since cowpox was used for variolation. I would guess vaccination came first and then 'variola' and 'vaccinia' as the different pathogens were identified. Anyone else know?
It's worse, isn't it? With 40,000 civilians vaccinated, isn't there that much more chance someone we don't want to have real smallpox could get some? It's like telling a thousand people to keep a secret. [make up some embarassing secret and publish it here].
They say you're much more likely to be shot if you own a gun.
So which came first: the word vaccination, or vaccinia?
It's worse, isn't it? With 40,000 civilians vaccinated, isn't there that much more chance someone we don't want to have real smallpox could get some? It's like telling a thousand people to keep a secret. [make up some embarassing secret and publish it here].
They say you're much more likely to be shot if you own a gun.
So which came first: the word vaccination, or vaccinia?
Sorry - it kept saying "Server Error". I assumed it didn't post.
This seems really pointless. If someone had been working on small pox as a biological weapon, wouldn't they go to the trouble of tinkering with it so the existing vacciation did not work?
Corbs,
That's an interesting thought. I don't know though.
You'd have to have a lot of infrastructure maybe not for the genetic tinkering but then for the confirmation and testing and weaponization and production. I don't think there's any terrorist group that could do this. So we're talking about state actors only and other than Russia and maybe China, if they can get the virus, who else?
If you can get some smallpox and deliver it, well, that's one thing. But getting the smallpox and playing with it without destroying it or killing yourself that's another egg entirely.
AIDSBLOG of the month: available online at
http://securebar.secure-tunnel.com/cgi-bin/nph-freebar.cgi/110110A/http…
Dear Dale and Adele,
Dale. Suffice it to say, you are right, I am not "a medical doctor" (thank The Intelligent Designer): But I do have to teach pathology at the largest medical school in the United States to second year medical students (about 250/course/year), cell biology (only graduate students these days-thank whom ever), oncology and cancer biology (to young doctors here who work with me on such projects as trying to transform MCF 10A cells, and normal cervical cells with live "HPV" (acquired from patients condemned and whose lives have been ruined by Digene's kit or Merck's fraudulent vaccine). On a daily basis I teach my grad students and post docs about what I have learned about breast cancer and melanoma reversion using simple ECM molecules found in embryos, and oncolytic herpes viruses and CMV. With my bioengineering students (typically small groups of senior undergrad students) we design and build projects in a year-long course-they won both First and Second Place awards in the Chicago-Wide UIC bioengineering EXPO competition two years ago-and yes I was proud of them http://www.uic.edu/depts/enga/current_students/expo2005.htm), and believe it or not, I also teach piano (in 1975 I first went to The University of Iowa as a Freshman on a music scholarship, but got interested in the Iowa Writer's workshop, dropped out of college to live at a commune in Iowa City called Black's Gas Light Village, and then started reading F. Nietzsche, J. Joyce, Nikos Kazantzakis (who I named one of my son's after), and others, but I decided I could never write "as good as them guys" so I got a degree in physical anthropology and primate studies-which couldn't get me a job as Reagan had just been elected and the NIH budget cut so a guy I wanted to study lemers with in Madagascar couldn't take me, so I stayed an extra year at Washington University after I graduated and taught Human Osteology to premed students and archaeology students, and forensic scientists, etc, etc. Then to feed myself and my woman, I started tissue culturing as a lab tech in different labs in St. Louis and Berkeley CA for 5 years before deciding to get my PHD in cell biology. After I got my PhD at Berkeley, I was on Judah Folkman's vascular task force for several years at Harvard as a post-doc while working out the basis of endothelial receptor signaling in the context of normal tissues and cancer. While at The University of Iowa, and contrary to the anti-angiogenesis hypothesis I helped explore with Folkman while a postdoc, I did make a minor discovery that tumors make their own vascular system if they are malignant, and the vasculature is made from tumor cells, and not endothelial cells in a variety of malignant cancers. Some 50 independent groups have confirmed the findings since I first reported the phenomenon in 1999. Unfortuately, the finding predicted the failure of anti-angiogenesis for cancer-a 12 or more billion-dollar industry, which has occurred despite the hype regarding avastin or other so-called anti-angiogenesis inhibitors (Call up Sloan-Kettering, M.D. Anderson, University of Wisconsin Comprehensive Cancer Center, The NIH, Dana Farber, or other leading cancer institutions-and ask them about their trials with Avastin, Endostatin, Angiostatin, or VEGF-inhibitors if you don't believe me). So yes you are correct, I am no DOCTOR and I don't really have any basis for asking a question about medicine, or biology.
Adele, You can tell me to go to hell and that I am a self-deluded fool, and you can make fun of how I spent the money donated at my father's funeral on Alive and Well AIDS alternatives (its amazing how you found this out, but then I remembered it was on his obit-amazing what you can learn on line these days that is potentially damaging to a fellow like me), and how that makes me incapable of thinking rationally. But somehow, I am not at all surprised. You guys like to taunt and terrorize the survivors of dead loved ones, like Christine and Robin, while you advocate such things as The Nazi State taking their children away to test and drug them to death as they did at ICC and elsewhere, despite their good health and parents observations (ever have your own children-better get them "HIV" tested even if you yourself test inconsistently positive 6 different times, as did Christine Maggiore)? Regarding inconsistently testing 6 times in a row, as she did, and this of course is very important to consider regarding the case of Eliza Jane (whose funeral I attended), is that in science, I was taught that if something happens, say in a Petri dish, once, it is a fluke (like testing positive on an Eliza or WB or PCR): if it happens twice, it is a coincidence. If it happens 3 times in a row, then you got a line to draw on a graph-etc. For someone like Christine, who has tested inconclusive, positive, inconclusive, positive, negative, and positive, I don't think that qualifies as any kind of reality regarding her "HIV-status" in any epistemology (except perhaps religion), if you see what I mean.
However, I am disappointed by both of your learned criticisms of me. Once again, and despite all your learned and well-considered responses, you didn't answer my simple question about the T-cells. Just for the record, I forwarded the money to Christine's organization because at that difficult time during the demise and loss of my father from brain cancer at 73, and because of the insistence of his DOCTORS at his hospital who insisted on testing him for "HIV" dementia against my wishes, and my demands to not do so. I felt that Christine Maggiore was at that time the most articulate spokesperson on the subject of how "HIV-positive" folks are stigmatized and brutalized by the AIDS establishment and Public Health Service, and by people such as you and your ilk. As a consequence, I thought that Christine's organization may be able to reach more of the folks whose lives have been victimized and often destroyed- and who have been terrorized by people like you, and I felt that her organization was more worthy of support than all of the quack scientists and Church of Modern Medicine folks:
1. who continue to advocate such things as failed "HIV" vaccines and "HIV" vaccine trials (that contain dangerous adjuvants such as MF-59-or squalene, used to intentially evoke non-specific immune reacions, because, to date, and as Barre-Sinoussi concluded at Toronto last summer in her talk, 15 failed "HIV" vaccine trials (at taxpayers expense exceeding $120,000,000/ for some of them) have not evoked humoral, cellular, or mucosal immunity, or demonstrated T-cell activation to date (see the 1995 Congress of the United States: Office of Technology assessment. Adverse Reactions to HIV Vaccines: Medical, Ethical, and Legal Issues-Roger C. Herdman, Director-a document which claims there were at least 30 such trials conducted before 1995, and as many as 80 trials that were aborted or not fully disclosed-I guess Barre-Sinoussi didn't read the congressional reports detailing adverse reactions and legal issues involved with any "HIV" vaccine, and she only was aware of the recent 15 failed "HIV" trials),
2. who continue to advocate that although almost a million Americans supposedly have antibodies to "HIV" in their bodies and should test "HIV-positive," as demonstrated by the production of antibodies to "HIV," and that contrary to what is understood about how the immune response is supposed to work by first identifying antigens in the universe that are non-self, and which appear to the immune system as non-self (which "HIV" apparently does according to your logic since about 1,000,000 "HIV" positive Americans can't all be artifacts), that somehow, "HIV" vaccines are the way to go if you can only ignore the fact that thousands of people in "HIV" vaccine trials who have been injected with components supposedly derived from "HIV" have not, and will not develop those same "HIV-positive" antibodies to whatever the non-defined shit is that the "HIV" vaccinees are being jabbed and inoculated with, because whatever these molecules are, they are not viewed by the immune system as non-self, and cannot evoke a humoral, cellular, or mucosal responses, or even stimulate T-cells without adding squalene or other toxic adjuvants that cause autoimmune diseases in rats (and soldiers),
3. who continue to advance the idea that although "HIV" vaccine components could not have been derived from anything unique and exogenous because no humoral, mucosal, or cellular immunity is evoked, that adjuvants such as squalene are good for ya because there is evidence that they have evoked autoimmune diseases in every sick Gulf War I veteran tested that have antibodies to squalene found in their blood (P. B. Asa et al., Exp. Mol. Pathol 68, 196-197, 2000; Asa PB, Wilson RB, Garry RF. Antibodies to squalene in recipients of anthrax vaccine. Exp Mol Pathol. Aug;73(1):19-27, 2002; see Gary Matsumoto's book, Vaccine A, Basic Books Publisher), and, in addition, squalene is the molecule of choice if you are trying to get a grant that proposes the induction of arthritis, lupus-like syndromes, or neurodegenerative diseases, or other autoimmune diseases in rats, or other experimental animals,
4. who continue to advocate Nazi-like initiatives such as failed cancer drugs like AZT or other DNA chain terminators that wipe out the immune system at the dosages given to a generation of gay men during the 1980's and early 90's, or in many cases infants and pregnant women, before it was found (by the Veterans Affairs and Concorde study and many, many others) that "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians (1); and that "The results of Concorde do not encourage the early use of zidovudine in symptom-free HIV-infected adults, and call into question the uncritical use of CD4 cell counts as a surrogate endpoint for assessment of benefit from long-term antiretroviral therapy (2);" and that children born to ZDV-treated mothers "are more likely to have a rapid course of HIV-1 infection compared with children born to untreated mothers, as disease progression and immunological deterioration are significantly more rapid and the risk of death is actually increased during the first 3 years of life" (3),
5. who continue to advocate smearing microbicides on the genitals of every African is a good thing, despite at least 2 large studies that were stopped because it was found that these microbicides increased the formation of lesions and increased the incidence of "HIV-positivity" in these folks who were told to use them to help curb their wild sexual behavior since they are black,
6. who now advocate we chop off a part of every black-male's penis in Africa as they cheerfully "line up around the clinics" to be circumcised following the recommendations of studies performed on 100% of persons that visited STD clinics for STD treatments (chlamidia, syphilis, etc) according to Robert Bailey, who is at my institution, and who did the recent much touted, circumcision study that was published by newspapers world-wide before the peer review study emerged a month or two ago ( and which Charles Geshekter and I wrote a report that totally demolishes these claims because African statistics are not given by Africans themselves, because when they are, no such numbers come even close to those of the AIDS establishment, or Bailey's),
7. who ignore Max Essex's nevirapine-induced "virological failure" of 41.7% versus 0% in the 875, 000 African mother-child pairs in which nevaripine was "tested" (despite Tremont's admitted fudging of the nevaripine trial results and Fishbein's dismissal for blowing the whistle on him the year before -"AIDS Research Chief Rewrote Safety Report." By John Solomon, Dec 2004. Associated Press Writer. www.ahrp.org/infomail/04/12/15b.php):
"Well over 875,000 women and infants have received a single dose of nevirapine. A single dose of nevirapine is the cornerstone of the regimen recommended by the World Health Organization (WHO) to prevent mother-to-child transmission among women without access to antiretroviral treatment and among those not meeting treatment criteria. However, nevirapine resistance is detected (with the use of standard genotyping techniques) in 20 to 69% of women and 33 to 87% of infants after exposure to a single, peripartum dose of nevirapine. Among 60 women starting antiretroviral treatment within 6 months after receiving placebo or a single dose of nevirapine, no women in the placebo group and 41.7% in the nevirapine group had virologic failure (P<0.001). Women who had received a single dose of nevirapine had significantly higher rates of virologic failure on subsequent nevirapine-based antiretroviral treatment than did women who had received placebo. This apparently deleterious effect of a single dose of nevirapine was concentrated in women who initiated antiretroviral treatment within 6 months after receiving a single dose of nevirapine. We did not find that a previous single dose of nevirapine compromised the efficacy of subsequent nevirapine-based antiretroviral treatment in women who started antiretroviral treatment 6 months or more after delivery. Among the 30 HIV-infected infants, a single dose of nevirapine (one each to mother and infant) as compared with placebo was associated with significantly higher rates of virologic failure and smaller CD4+percentage increases in response to subsequent nevirapine-based antiretroviral treatment"[4],
8. who continue to advocate such Nazi-like initiatives as universal "HIV" testing, despite the fact that even "AIDS experts" like Klausner and others have stated that the hapatitis B vaccine [5], the flu vaccine [6,7,], and more than 70 known reasons or syndromes will evoke a positive "HIV" test at rates as high as 2%-5% ?% of "low risk" (read white) populations of soccer moms and golf-enthusiasts living in the suburbs.
Somehow, I ain't surprised by your statements or responses to my simple question. And you still haven't answered my question:
I will state it again: Is AIDS a disease of too few lymphocytes (less than 1000/ul as given by the WHO), or is it a disease of too many lymphocytes, like cancer, or as in the case of Eliza Jane who had 10,800/ul, and who died of a classic delayed hypersensitivity reaction to b-lactams, as described by a huge literature on Medline?
Gee wizz guys-I ain't asking for much here. Don't make fun of my father's death or the fact that I chose to make his funeral contributions go toward helping stigmatized "HIV-positive" folks. Please don't make excuses on how children can have 10,800 T-cells and be considered AIDS patients. Please don't insult our ability to know the difference between the numbers, 1000 and 10,800. For example, 1000 lymphocytes is 1 more that 999 lymphocytes, right? And 10,800 lymphocytes is 1 more than 10,799 lymphocytes, right?
"AIDS" in children is considered to occur according to the WHO publication I referenced above, when T-cells are at or around 1000/ul. You can't have 10,800 lymphocytes and have PCP or a nervous system infection. It don't work that way.
So, it is always good to talk "science" with you on such a "upcoming" "intellectual" website. And no, I ain't A DOCTOR!
Cheers,
andrew
Very sad, Andrew, such a promising career as yours has been sidetracked by delusions. It's happened to others, but it's just as sad in you. And I wouldn't make fun of anyone's death. I didn't make fun of your father. I resent your suggesting it. I just pointed out if you're so down with Alive and Well you give contributions in a loved one's honor! then youre not objective. It's like if I'm on the board at Merck, I can't go out and defend Vioxx publically and pretend I'm just some random gal. You'd point out my conflict, and you should. That's what I did, any disrespect was for you, not your father, who has nothing to do with this.
But you're really into misrepresenting! Your only science arguments are misunderstandings so you resort to the usual, accuse people of racism and Nazism and genocide and statism and making fun of people's deaths.
Your "points" don't make sense. Same old denialist arguments. Same old anti-vaccination pie in the sky. Rebutted everywhere but of course you wouldn't accept it if God, Einstein, and the OED combined in one person hit you over the head with it. I'll not waste my little voice attacking your delusions. But since your so eagre about the TLC.
As I said, your questions about total counts were answered many times already on this blog, on other blogs and in the scientific literature. Since you are not a doctor and since you haven't read the discussion, I'll summarize again.
1. Newborns and toddlers tend to have higher lymphocyte counts than older children and adults. True too for HIV + babies vs HIV+ adults.
2. The literature describes cases where children have died of AIDS/PCP displaying total lymphocyte counts similar to Scovill's. The references was given on the other thread if youre interested.
3. The WHO recommendation is for places and times where you can't do a CD4 count. Sometimes the total count is a stand-in. If a child has a really low count, like 700 total, then you know the CD4 count can't be high no matter what the 4/8 ratio is. But if the total count is high, it doesn't mean the CD4 count HAS TO be high or the 4/8 ratio is normal. Like said, see cases where kids with high TLC died of PCP like EJ.
4. OK its not lymphocytes but if you're not a doctor how are you so sure about "delayed hypersensitivity reaction"? You act like you've read the lit on this. Can you give us some examples of children dying of it 48 hours after being exposed to something the very first time in their entire lives? And then the standard treatments by the EMTs having no effect? I just looked up some of these papers out of curiousity, I found one with 10 cases described but of course they'd all had the antibiotic long before the reaction and the reaction happened six or more days after they started taking it again. And they didn't die they had rashes and red skin and joint pain.
You accuse me of being religious. HAving faith. No. I like to read things in the lit before I believe them. I like confirmation. WHy do you talk about Type IV reactions when you don't know what they are? Why do you insist Maggiore tested this way and that way a certain number of times on an HIV test? Did you perform the test? Did you go through her medical records? Or do you believe her because well you believe her, shes a friend, this woman who brazenly calls herself "The Mom, The Legend"?
Andrew, let me suggest you leave the Maggiore issue alone. This is the third or fourth time I've said it on here, it's YOU and other denialists who ALWAYS bring up EJ. ANd then people respond with facts and you accuse them of victimizing someone.
Honestly.
The Eliza-Jane case is sad because a tragic loss of a child was turned into a political football. It is clear that a second autopsy was done on the child with manufactured results for political reasons to intentionally discredit the political activities of the mother.
I agree with Andy Maniotis who has an excellent grasp of this issue, and is an excellent academic molecular biologist. Andy is absolutely correct. PCP requires immunosuppresion to produce pneumonia. A normal lymphocyte count precludes immunosupression and precludes a diagnosis of AIDS.
Andy is not alone in his questions regarding many of the common practices of medicine which are based more on financial gain than on good science.
Indeed, all of science has been up for sale to commercial and political interests for decades. HIV/Aids is merely one example of a pervasive problem. The proposition of treating a retroviral nucleotide base sequence after it has been incorporated into the host genome with cytotoxic drugs is not only wrong, it is ineffective and immoral.
If and when respectability returns to science will remain an open question.
Why on earth is anyone paying attention to Adele? She's a clueless 20-something year-old, obnoxious twit.
Here's a google search of Dr. Maniotis' papers.
Adele, please direct us to anything you have ever published on any of these related topics. Thanks.
"The Eliza-Jane case" there's no hyphen idiot, is tragic because if this child had gotten basic standard medical care she'd be alive today.
PLEASE.
If anyone says one more time a child can't die from PCP if they have high total lymphocytes I'm gonna scream so loud they'll hear me in the next province.
Here's something I copied from an article "Science Outsold" on AIDStruth, aidstruth dot org.:
Nevertheless, diagnostic differences do separate adult and pediatric criteria, and for good reason. Quantitatively and qualitatively--and including the response to HIV [74, 75]--the immune systems of infants and toddlers are different from those of older children and adults. It is thus not a particular surprise that an immunodeficient child might fall prey to diseases seen relatively rarely in the immunocompromised adult (and vice versa; see earlier discussion of KS). A pediatrician must be on the lookout for symptoms that might not appear in adults, hence several unique conditions are CDC criteria for a pediatric AIDS diagnosis [76]. Treatment recommendations are also different for young (i.e. <6 year old) children. For example, whereas prophylactic treatment for fungal pneumonia is recommended for adults with CD4+ counts under 200/ul, it is encouraged even at higher CD4+ counts for children up to six years of age and for all HIV+ infants in the first year, regardless of CD4+ count. This is because the average young child has a much higher total number of CD4+ lymphocytes than the average adult. In contrast to adult disease, the "risk of developing PCP in this age group is only weakly dependent on the T-helper cell count" [77]. In other words, even children with "high" CD4+ T-cell counts can develop AIDS-defining conditions. One study of perinatally-infected infants found Pneumocystis carinii pneumonia (PCP) in a child with a total lymphocyte count of about 10,000 [78]; several other children with PCP also displayed higher-than-average counts.
Here are the references.
74.Palumbo, P.E., et al., Predictive value of quantitative plasma HIV RNA and CD4+ lymphocyte count in HIV-infected infants and children. Jama, 1998. 279(10): p. 756-61.
75.Church, J.A., HIV disease in children. The many ways it differs from the disease in adults. Postgrad Med, 2000. 107(4): p. 163-6, 169-71, 175-6 passim.
76.CDC, 1994 Revised Classification System for Human Immunodeficiency Virus Infection in Children Less Than 13 Years of Age, 1994, CDC.
77.Urschel, S., et al., Withdrawal of Pneumocystis jirovecii prophylaxis in HIV-infected children under highly active antiretroviral therapy. Aids, 2005. 19(18): p. 2103-8.
78.Thea, D.M., et al., Benefit of primary prophylaxis before 18 months of age in reducing the incidence of Pneumocystis carinii pneumonia and early death in a cohort of 112 human immunodeficiency virus-infected infants. New York City Perinatal HIV Transmission Collaborative Study Group. Pediatrics, 1996. 97(1): p. 59-64.
There you have it. Kids can die of PCP even with total cell counts like EJ. Now can any of you three denialist out there give me a single report where a child died of Type IV reaction 48 hours after FIRST EXPOSURE EVER to ANYTHING?
PS, hey thanks for the comment on my age I wish I was still 20-something!
OK, that quote was messed up. THis follows what I have in italics above.
"<6 year old) children. For example, whereas prophylactic treatment for fungal pneumonia is recommended for adults with CD4+ counts under 200/ul, it is encouraged even at higher CD4+ counts for children up to six years of age and for all HIV+ infants in the first year, regardless of CD4+ count. This is because the average young child has a much higher total number of CD4+ lymphocytes than the average adult. In contrast to adult disease, the "risk of developing PCP in this age group is only weakly dependent on the T-helper cell count" [77]. In other words, even children with "high" CD4+ T-cell counts can develop AIDS-defining conditions."
And then some more.
"One study of perinatally-infected infants found Pneumocystis carinii pneumonia (PCP) in a child with a total lymphocyte count of about 10,000 [78]; several other children with PCP also displayed higher-than-average counts."
Wow. Sorry. I missed the little arrow. Let me try again.
Heres the whole thing.
"Nevertheless, diagnostic differences do separate adult and pediatric criteria, and for good reason. Quantitatively and qualitatively--and including the response to HIV [74, 75]--the immune systems of infants and toddlers are different from those of older children and adults. It is thus not a particular surprise that an immunodeficient child might fall prey to diseases seen relatively rarely in the immunocompromised adult (and vice versa; see earlier discussion of KS). A pediatrician must be on the lookout for symptoms that might not appear in adults, hence several unique conditions are CDC criteria for a pediatric AIDS diagnosis [76]. Treatment recommendations are also different for young (i.e. LESS THAN 6 year old) children. For example, whereas prophylactic treatment for fungal pneumonia is recommended for adults with CD4+ counts under 200/ul, it is encouraged even at higher CD4+ counts for children up to six years of age and for all HIV+ infants in the first year, regardless of CD4+ count. This is because the average young child has a much higher total number of CD4+ lymphocytes than the average adult. In contrast to adult disease, the "risk of developing PCP in this age group is only weakly dependent on the T-helper cell count" [77]. In other words, even children with "high" CD4+ T-cell counts can develop AIDS-defining conditions. One study of perinatally-infected infants found Pneumocystis carinii pneumonia (PCP) in a child with a total lymphocyte count of about 10,000 [78]; several other children with PCP also displayed higher-than-average counts."
My God, Adele, are you an embarrassment. You can't even cut and paste right!
Dear Adele,
I felt I needed to respond to your criticisms, and tried several times to post on the http://securebar.secure-tunnel.com/cgi-bin/nph-freebar.cgi/110110A/http…
site, but it kept saying "page not found." I saw that you also post on the Aeteology site, so I took a chance that you might see my response. You might want to inform Tara about the other site "isn't it interesting..." being unpostable. She won't respond to any info I send her.
First the info I relayed to you about Christine's inconsistent testing came from reference 3, her book. I have never seen her records, as she is quite private about that sort of thing, probably because she is perfectly healthy. But I have no reason to believe she would lie about her stigmatization and how it occurred over and over again during the 6 inconsistent tests.
Regarding your response to my post this morning: (and I have included refs that are from a much longer analysis I wrote when Eliza Jane died, so they don't begin at 1,2, and there is a gap-you can figure it out:
Nobody can claim to be an expert on adverse reactions to drugs: the science that studies them is at its infancy. However, it is widely appreciated that adverse reactions for all kinds of pharmaceutical interventions are under-reported, or aren't reported at all. No physician or hospital wants to be responsible for the tragic event that a prescription, meant to alleviate suffering, caused an adverse reaction or death of a patient. Yet the history of drug and vaccine trials show that responses to these and other medical interventions are always associated with unpredictable adverse responses, as the physiology of every human is different. When adverse reactions do occur, they may be difficult or impossible to pigeonhole as a stereotypical series of complications. Nevertheless, and despite under reporting, beta-lactam adverse reactions are frequently reported. Most doctors indeed ask, "are you or is your child allergic to penicillins or other antibiotics," before they are prescribed.
The World Health Organization puts the figure of adverse reactions to this class of drugs at around 0.7%-10%, depending on the nation studied (14).
In a 2000 case report, da Fonseca reported that (15):
"Penicillin is the drug that most often leads to allergic reactions and anaphylaxis. The incidence of adverse events triggered by penicillins is believed to be between 1% and 10%. Up to one-tenth of these episodes are life-threatening, with the most serious reactions occurring in patients with no history of allergy."
Investigators who study allergic reactions, such as Gomes et al., reported that: (16):
"The prevalence of self-reported drug allergy was 7.8% (181/2309): 4.5% to penicillins or other betalactams, 1.9% to aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs) and 1.5% to other drugs. In the group 'allergic to beta-lactams', the most frequently implicated drug was penicillin G or V (76.2%) followed by the association of amoxicillin and clavulanic acids (14.3%)."
"Women were significantly more likely to claim a drug allergy than men (10.2% vs. 5.3%). The most common manifestations were cutaneous (63.5%), followed by cardiovascular symptoms (35.9%). Most of the reactions were immediate, occurring on the first day of treatment (78.5%).
Out of 2409 spontaneous adverse event reporting from 1991-1996 in Bulgaria:
" 29% of the adverse drug reaction reports concerned the patients in the age groups of 0-5 year old, and amoxicillin is a drug with a majority of reports for the period" (17).
A group in Spain reported similar findings where amoxicillin caused the most adverse reactions (18).
So-called delayed reactions with amoxicillin are also frequent, and are a subject of intense investigation. For example, there is a developed literature on the subject with titles such as: "Diagnosing nonimmediate reactions to penicillins by in vivo tests" (19), "A diagnostic protocol for evaluating nonimmediate reactions to aminopenicillins" (20), "Diagnosis of nonimmediate reactions to betalactam antibiotics" (21), "Role of delayed cellular hypersensitivity and adhesion molecules in amoxicillin-induced morbilliform rashes" (22), "Nonimmediate reactions to betalactams: prevalence and role of the different penicillins" (23), "In vitro T-cell responses to beta-lactam drugs in immediate and nonimmediate allergic reactions" (24), "Skin test evaluation in nonimmediate allergic reactions to penicillins" (25), "Two cases of toxic epidermal necrolysis caused by delayed hypersensitivity to beta-lactam antibiotics" (26), "Immediate and delayed hypersensitivity from penicillin (27), "Incidence of beta-lactam-induced delayed hypersensitivity and neutropenia during treatment of infective endocarditis" (28).
Nevertheless, in their allopathic training, most medical students are only taught that "a true amoxicillin allergic reaction" is rapid and stereotypic, would present as tachycardia and produce its symptoms within seconds or minutes instead of hours or days, and would be rapidly reversible by administration of epinephrine. This misinformation ignores the developed literature on delayed hypersensitivity reactions indicated above. The weight of Eliza Jane's heart as reported by the ME at autopsy was 131% of normal. This evidence of ventricular hypertrophy (or edema) is best attributed to loss of pressure due to loss of fluid over a period of hours from the capillaries in the heart, and subsequent widely observed compensation by the heart muscle to pump more fluid. It also ignores the likelihood that electromechanical dissociation (EMD), may have been responsible for the slowed rhythms of her heart and the pulseless state that were noted by the ER staff (rather than tachycardia), in association with hypotensive multiple organ failure accompanying massive edema (loss of fluid from the vasculature). If there is significant loss of blood volume from the vasculature, because 40% of it has leaked out into the tissues due to the toxic effects of amoxicillin, and if the vasculature continues to be permeable, as indicated by the measurements of Eliza Jane's abnormal organ weights, then as long as the antibiotic was present and inducing a series of reactions leading to vascular permeability, it wouldn't matter if the heart was restarted or even working normally, or how much IV solution she was infused with. This hypothesis is supported by the fact that although the ER treatments of epinephrine transiently stimulated the heart to beat on several occasions, before she was given more antibiotics of an undisclosed type at the hospital, and presumably more IV's, the multiple boluses of epinephrine couldn't stabilize her heart for very long, or restore normal blood pressure or normal pulse. The IV fluids repeatedly administered could have killed her by continuing to swell her heart as they leaked out, causing EMD, and drowning her lungs (and kidneys) with extravasated proteins and fluids leaked from the vasculature. However, the fact that her abdomen and liver were protruding by the time she arrived at the ER may have meant that she had already leaked too much fluid from her own vasculature to ever recover normal vascular blood volume, even before the multiple IV's were administered, principally from the delayed adverse reaction to the amoxicillin itself (2):
"On May 14th, in a follow-up visit, one of the physicians found that her lungs were clear, but noted redness in addition to fluid in her right eardrum. He prescribed 400mg of amoxicillin twice a day to the beta-lactam-naïve child" (1).
"After the third dose of amoxicillin, she vomited several times, and she became agitated. Her mother noticed that her face became pale, her arms changed color and were cold to the touch. She became lethargic and ran a low fever. Then she fell unconscious and stopped breathing, and no pulse could be felt by the emergency team or by the admitting physicians" (2). (Do you think this is consistent with the kind of morbidity typically observed by children who are running around happy and healthy hours before and die of "AIDS?")
"The Los Angeles City Fire Department RA 239 was dispatched on May 16th at 0003 and arrived at Eliza Jane's home at 0006 (1,2). Upon the paramedic's arrival, Eliza Jane was found pulseless and apneic on the floor. She was cyanotic with cold extremities and asystolic on the cardiac monitor."
"Eliza Jane was presented at the emergency room of Valley Presbyterian Hospital at 0026 on May 16th. On arrival, she was pulseless, had no spontaneous respiration, and appeared very pale. Her pupils were mid position and fixed."
"The treating physician examined Eliza Jane and found that her abdomen and her liver were distended. Her extremities were cold and poorly perfused with non-palpable pulses. Her oral mucous membranes were pink and there was a lesion on her lower lip."
"At 0105 her heart rate began to slow down into the 40-60 b/min range and she did not have a papable pusle. CPR was restarted. She was bagged with 100% O2 and given high dose epinephrine 1.3mg, atropine 0.26 mg, and sodium bicarbonate 13 mEq. Her heart rate began to increase, it came up to 113 b/minute, and she had a palpable pulse."
"At 0137, no blood pressure could be obtained and Eliza Jane was started on dopamine drip at 5 microgram/kg per hour. Her blood pressure reached to 41/28 and was taken to CT scan. While in CT scan, she had another episode of asystole and she was given atropine, and sodium bicarbonate. She developed a pulse again and was transferred to the Pediatric ICU."
"At the PICU, her heart rate reached approximately 120b/min but she did not have a pulse. She was given fluid boluses, as well as being placed on dopamine 10 microgram/kg/hour and dobutamine 10 microgram/kg per hour. She did not have a pulse and her blood pressure was not obtainable in spite of these treatments. She was also started on antibiotics."
(Jesus H. Christ-I guess people have a lot of faith in antibiotics-that they can reverse cardiac arrest! I wonder what antibiotic they gave her in the ICU????)
The type of antibiotic given in the PICU is not disclosed, but is of concern, given that Eliza Jane presented with classic signs, and a package-insert-perfect description of an adverse reaction to amoxicillin, rather than end-stage AIDS, as stated by the Medical Examiner's office.
Amoxicillin package inserts (29) describe most if not all the reactions manifested by Eliza Jane in their warnings (I have underlined the adverse events manifested by Eliza Jane as described by her parents, the hospital, and the coroner's report)."
Beta lactam antibiotics-
Anaphylactic reactions manifested by urticaria, flushing, pruritus, laryngeal edema, and cardiovascular collapse may occur within minutes or, less frequently, hours after administration of beta lactam antibiotics (ie, drugs that have a common beta lactam ring structure)."
SIDE EFFECTS AND SPECIAL PRECAUTIONS
Gastro-intestinal side effects including diahrroea, nausea and vomiting may occur quite frequently. Pseudomembranous colitis has also been reported.Super-infection is relatively common. Doses should be reduced in severe renal failure.
Nausea and vomiting occurred after Eliza Jane's second dose of amoxicillin. Eliza Jane's kidneys were measured at 146% of normal, without significant damage exhibited microscopically, consistent with massive edema and recent injury.
"The most feared adverse events attributed to beta-lactam antibiotics are IgE type I immediate or accelerated reactions. These develop within minutes to hours of drug administration and cause hypotension, laryngeal edema or bronchospasm. Such reactions occur when patients with preformed beta-lactam-specific IgE antibodies, which are bound to tissue mast cells and circulating basophils, are exposed to the drug or tissue protein complex, resulting in the release of inflammatory mediators."
"Unpredictable reactions occur independent of the dose and route of administration and reflect such factors as drug intolerance, allergy, and other idiosyncratic responses. These reactions seem to preferentially affect certain body systems, most commonly blood, skin, and liver."
Eliza Jane's bood work was abnormal to the extent that she was profoundly anemic and exhibited a low hematocrit (Her hemoglobin and hematocrit counts were low (6.3 g/dl instead of 12-16g/dl, and 21% instead of 37-48%, respectively). (2). Her neutrophils were measured at 12% (normal=45-74%) (2). Her monocyte percentage was in the normal range at 8% (normal is 4-10%) and her platelet count (214 k/µl) was in the normal range (130 k/µl -400 k/µl) (2).
And as indicated on the amoxicillin package insert:
"Additional unique life-threatening reactions caused by beta-lactam antibiotics are referred to as "late" reactions. They include such events as hemolytic anemia, Stevens-Johnson syndrome, and exfoliative dermatitis."
Her liver findings were abnormal as well: Eliza Jane autopsy showed liver changes consistent with an immune reaction to amoxicillin, which in some cases of acute toxicity has been noted to resemble pregnancy-fat-like-accumulation and steatosis (30-33).
It is also now emphasized during the early training of many clinicians, as well as in the literature (16), that the effects of amoxicillin on the liver are usually only found when used with another drug, clavulanate, but this misinformation is not supported by the primary literature in Medline: there are many reports that indicate the rate of acute reactions occur in multiple cohorts of patients who were studied for amoxicillin versus amoxicillin-clavulanate reactions, and both appear quite frequently, judging by the number of reports. Perhaps the most comprehensive report that surveys the growing literature on the subject of amoxicillin versus amoxicillin/ clavulanate is presented by Berg et al, and in connection to both fatal and non-fatal adverse reactions to amoxicillin/amoxicillin clavulanate, which they claim typically occur after antibiotic therapy was discontinued, and serves to reinforce the idea that none of these drugs can be considered as safe, even after they are withdrawn (34).
Eliza Jane was never administered any skin allergy tests for amoxicillin, which may have been a wise thing to do, for a bata-lactam-naïve child. Even so, there have even been references to amoxicillin-induced death when cutaneous sensitivity tests to the beta-lactam drugs are given at allergy testing doses (which are extremely small doses) to determine if someone is allergic to these drugs, before giving them a full dose (35).
One group of allergists have even postulated the technical term "flare-up" to describe these kind of delayed reactions as a Type IV mechanism, and described the difficulty in typifying these kinds of reactions. As stated by Reig Rincon de Arellano I et al., (36).
" We suggest that this phenomenon of Flare up occurs by a Type IV mechanism mediated by T-cells without participation of IgE antibodies. The betalactam hypersensitivity mechanism which has usually been described is an IgE mediated reaction, but there are other not very well known mechanisms that are responsible for the delayed reactions."
And yes, I would doubt Einstein, God, and James Watson if they didn't provide evidence for their claims. Why should I be any less critical about the junk science you call "HIV/AIDS?" You might want to check out a paper I wrote in 1998 regarding the non-activity of "HIV" integrase in a toposomerase study (Because of the extreme censorship of us by the AIDS establishment, I had to bury the "HIV" non-result to get the damn thing published as a negative control for DNA minor groove binding). Also, you might want to read Gallo's book, Virus Hunting, where it describes my former boss, Judah Folkman's dismissal of the fact that Kaposi's sarcoma couldn't have anything to do with "HIV."
Ah, those were the days when it all was still innocent. Well, it ain't innocent anymore. You all have had ample warnings and questions from "deluded" folks like me, Robert Root-Bernstein, Karry Mullis, Walter Gilbert, Lynn Margulis, Michael Lange, Stephan Lanka, Val Turner, about 3000 scientists, physicians, and others (on Crowe's website that signed a rather long document), and oh, how could I forget, Peter Duesberg and his correct mistake regarding the existence of "HIV," and the predictions he made that have all come true (I heard him lecture on it for the first time in 1985 in our departmental weekly seminar, and I was horrified as were many of us at Berkeley, at his suggestion that AIDS is not caused by a human retrovirus.
Regards,
andy
1. Autopsy report (Case No 2005-0367), Department of Coroner, Los Angeles California. September 15, 2005.
2. Medical record # 856441, Valley Presbyterian Hospital, 15107 Vanowen Street, Van Nuys, Ca, 91404.
3. Christine Maggiore. What if everything you thought you knew about AIDS was wrong? American Foundation for AIDS Alterntives. 4th Printing, 2000.
14. Bull World Health Organ. 38(2):159-88, 1968.
15. da Fonseca Pediatr Dent. Adverse reaction to amoxicillin: a case report. Sep-Oct;22(5):401-4, 209, 2000.
16. Gomes et al. Self-reported drug allergy in a general adult Portuguese population. Clin Exp Allergy. Oct;34(10):1597-601, 2004.
17. Getov I, Dimitrova Z. Antibacterials: spontaneous report analysis for a six years period in Bulgaria. Boll Chim Farm. Apr;138(4):186-90, 1999.
18. Minguez MA, Zapatero L, Caloto M, Martinez-Molero MI. A study of allergy to penicillin antibiotics in 1995 in the Child Allergy Department of the Gregorio Maranon University hospital. Allergol Immunopathol (Madr). Mar-Apr;26(2):43-6, 1998.
19. Romano A, Viola M, Mondino C, Pettinato R, Di Fonso M, Papa G, Venuti A, Montuschi P.Int Arch Allergy Immunol. Diagnosing nonimmediate reactions to penicillins by in vivo tests. 1: Int Arch Allergy Immunol. Oct;129(2):169-74, 2002.
20. Romano A, Quaratino D, Di Fonso M, Papa G, Venuti A, Gasbarrini G.A diagnostic protocol for evaluating nonimmediate reactions to aminopenicillins. J Allergy Clin Immunol. Jun;103(6):1186-90, 1999.
21. Romano A, Blanca M, Torres MJ, Bircher A, Aberer W, Brockow K, Pichler WJ, Demoly P; ENDA; EAACI. Diagnosis of nonimmediate reactions to beta-lactam antibiotics. Allergy. Nov; 59(11):1153-60, 2004.
22. Barbaud AM, Bene MC, Schmutz JL, Ehlinger A, Weber M, Faure GC. Role of delayed cellular hypersensitivity and adhesion molecules in amoxicillin-induced morbilliform rashes. Arch Dermatol. Apr;133(4):481-6, 1997.
23.Terrados S, Blanca M, Garcia J, Vega J, Torres MJ, Carmona MJ, Miranda A, Moya M, Juarez C, Fernandez J. Nonimmediate reactions to betalactams: prevalence and role of the different penicillins. Allergy. Jul;50(7):563-7, 1995.
24.Luque I, Leyva L, Jose Torres M, Rosal M, Mayorga C, Segura JM, Blanca M, Juarez C. In vitro T-cell responses to beta-lactam drugs in immediate and nonimmediate allergic reactions. Allergy. Jul;56(7):611-8, 2001.
25.Torres MJ, Sanchez-Sabate E, Alvarez J, Mayorga C, Fernandez J, Padial A, Cornejo-Garcia JA, Bellon T, Blanca M. Skin test evaluation in nonimmediate allergic reactions to penicillins. Allergy. Feb;59(2):219-24, 2004.
26. Romano A, Di Fonso M, Pocobelli D, Giannarini L, Venuti A, Garcovich A; Two cases of toxic epidermal necrolysis caused by delayed hypersensitivity to beta-lactam antibiotics. J Investig Allergol Clin Immunol. Jan-Feb;3(1):53-5, 1993.
27. Fernandez de Corres L, Lobera I, Munoz D. Immediate and delayed hypersensitivity from penicillin. Contact Dermatitis. Mar;14(3):194-5, 1986.
28. Olaison L, Belin L, Hogevik H, Alestig K. Incidence of beta-lactam-induced delayed hypersensitivity and neutropenia during treatment of infective endocarditis. Arch Intern Med. Mar 22;159(6):607-15, 1999.
29. Amoxicillin Package inserts:
-Part 2: Summary Statements Evidence-Based Commentary - VII. Prototypes Of Immunologically Mediated Drug Hypersensitivity Ann Allergy 1999; 83:S665-S700
www.jcaai.org/pp/dh_7_prototypes.asp
30. Hautekeete ML Hepatotoxicity of antibiotics. Acta Gastroenterol Belg. May-Aug;58(3-4):290-6, 1995.
31. George DK, Crawford DH. Antibacterial-induced hepatotoxicity. Incidence, prevention and management.Drug Saf. Jul;15(1):79-85, 1996.
32. Brown SJ, Desmond PV. Hepatotoxicity of antimicrobial agents.
Semin Liver Dis. 22(2):157-67, 2002.
33. Liu ZX, Kaplowitz N. Immune-mediated drug-induced liver disease. Clin Liver Dis. Aug;6(3):755-74, 2002.
34.Berg P, Hahn EG. Hepatotoxic reactions induced by beta-lactamase inhibitors. Eur J Med Res. Dec 17;6(12):535-42, 2001.
35. Valyasevi MA, Van Dellen RG. Frequency of systematic reactions to penicillin skin tests. Ann Allergy Asthma Immunol. Nov;85(5):363-5), 2000.
36. Reig Rincon de Arellano I, Villalon Garcia A, Cimarra Alvarez-Lovell M, Robledo Echarren T, Martinez-Cocera M. Allergol Immunopathol. Flare up to betalactams. Sep-Oct;33(5):282-4, 2005.
Andrew, this is a decent analysis of delayed-reaction hypersensitivity to beta-lactams. I've even read some of these papers before. But what you pasted here has no relation to the Scovill death. All of this literature is about people who were exposed to beta lactams maybe once maybe twice maybe a hundred times and developed an allergy. Then later in life when they took the drug they had a reaction maybe like type I or maybe type IV. EJ never had this drug.
If you believe Maggiore about her tests, why don't you believe her when she says EJ never had an antibiotic before or any other drug except maybe tylenol? IF she wasn't exposed, how did she get sensitized?
You can look at this and think, hmmm, encephalitis, hmmm, HIV proteins, hmmm, history of underweight and under size, persistent illness, PCP in the lungs, herpesvirus lesion, history of candida. All of these associated with AIDS.
Or you can take your tack and look at EJ as a medical first. Someone who never had an antibiotic but then developed Type IV in 48 hours and also got steatosis, got giant cells in the brain, got PCP in her lungs and the rest. It's like an antimiracle. Scary.
Find me a description on Pub Med or from a doctor you know of a child whose perfectly healthy, never had a drug, takes it for the first time and in 48 hours is dead of a type IV reaction and I'll concede it's a possibility.
Dear Adele,
The article (78) you quote which you feel supports your argument that PCP can occurr in children with normal lymphocyte counts does not in fact support your case.
The study was done on children of DRUG ADDICTS.
The mother of Eliza Jane was NOT a DRUG ADDICT.
This is a very large discrepancy.
In fact, all the studies of pediatric HIV/AIDS are done on drug addict mothers. The children of drug addicted mothers have a high mortality during the first 6 months of life because they are born from DRUG ADDICTS.
So Adele, before you call anyone else an idiot, call yourself one. Look it up.
78. Pediatrics. 1996 Jan;97(1):59-64. Benefit of primary prophylaxis before 18 months of age in reducing the incidence of Pneumocystis carinii pneumonia and early death in a cohort of 112 human immunodeficiency virus-infected infants. New York City Perinatal HIV Transmission Collaborative Study Group. Thea DM, Lambert G, Weedon J, Matheson PB, Abrams EJ, Bamji M, Straus WL, Thomas PA, Krasinski K, Heagarty M.
Dear Adele,
Let me keep this brief for once and not in any particular order. I don't want the chicken to burn on the que!
I've met Christine once (at the funeral of her beloved daughter), and having been a Californian myself for many years, and after reading her monthly Alive and Well flyer for several years now, I can testify with some certainty that she is indeed a new age pseudo-hippie type that, principally because of her own health stigmatization issues, she is the type that goes for "natural healing" practices like the gold rush minors went for the gold. She goes in for massage therapy, natural healing, herbs, etc. She'd make a good president of a homeopathic or naturepathic school.
Your dogged insistence that one needs a prior reaction to a molecule (sensitization) to experience a full blown, life-threatening or even life ending reaction runs contrary to thousands of tragic events that happen every year where persons are exposed to some molecule for a first time and die, or nearly die. I am a member of the National Vaccine Information Center, and if you want, I could send you the Vaccine Adverse Events Reports for every and all vaccines, where people have never been exposed to the preparation before, and drop off as dead as a doornail within minutes, hours, or even is some cases, although rare, weeks after vaccination. Bee stings, certain food reactions, nuts, shell fish, etc. all are known to cause death in sensitive (not sensitized) persons.
I believe you are also incorrect about the delayed reaction literature I cited exclusively tabulating folks that have been pre-sensitized. The emergence, and existence of the allergin tests using homeopathic doses exists as a new science in recent decades precisely because it is so well known (and predictable) that many (sensitive-not pre-sensitized) folks experience a bad or fatal reaction to every and all pharmaceuticals. In cancer research, which is my area, the most "nervous" time during an animal trial of a new antibody against some component of the tumor microenvironment occurs in the first several minutes or hours after the antibody is injected.
EJ had gained weight the last 6 months of her life. Is this consistent with wasting? People gain weight with AIDS wasting syndrome? I guess its like the T-cells. You make it sound so common that children are dying every day with 10,000 lymphocytes/ul. However, you must concede, and forgive my sarcasm in my previous posts, immune difficiency illnesses in association with the AIDS-defining T-cell range
is rare as unicorns in the US. Do you think it likely that children are dropping like flies from AIDS-defining diseases frequently who have 10,000 cells/ul?
EJ is no medical first. She is a classic b-lactam package insert casualty of allopathic medicine.
If you want me to send you the vaccine literature tabulating deaths from all vaccine, I have much of it, have written extensively on it, etc. I don't need to find a DOCTOR who has experienced what you seek to find out. DEATHS FROM GARDASIL, FOR INSTANCE ARE BEGINNING TO TABULATE, BUT THEN I COULD SEND YOU THE LISTS WE HAVE FROM ANY VACCINE YOU ASK ME FOR. ITS ALL AVAILABLE ON THE VAERS GOVERNMENT DATABASES.
CHEERS,
ANDY
Dr. Maniotis,
You are far too gracious in your response to Adele. She's basically just an internet twit, who has done no serious scientific research on any topic, and wastes much of her time twiddling around on the internet.
Don't sweat it.
But, one question: Is there evidence of any girls dying from the HPV vaccination?
...and existence of the allergin tests using homeopathic doses exists as a new science in recent decades ...
She is a classic b-lactam package insert casualty of allopathic medicine.
Can anyone tell me what a homeopathic pathologist is?
Dear Keven,
Please see the following:
Cheers,
Andy, the Homeopathologist (thanks Chris Noble! What a great title! Beats my current one for sure).
For Immediate Release
May 23, 2007 Contact: Press Office
202-646-5188
Judicial Watch Uncovers Three Deaths Relating to HPV Vaccine
Event Reports Obtained from FDA Detail 1,637 Adverse Reactions to Gardasil
(Washington, DC) -- Judicial Watch, the public interest group that investigates and prosecutes government corruption, today released documents obtained from the U.S.
Food and Drug Administration (FDA) under the provisions of the Freedom of Information Act, detailing 1,637 reports of adverse reactions to the vaccination for
human papillomavirus (HPV), Gardasil. Three deaths were related to the vaccine.
One physician's assistant reported that a female patient "died of a blood clot three
hours after getting the Gardasil vaccine." Two other reports, on girls 12 and 19,
reported deaths relating to heart problems and/or blood clotting.
As of May 11, 2007, the 1,637 adverse vaccination reactions reported to the FDA via
the Vaccine Adverse Event Reporting System (VAERS) included 371 serious reactions.
Of the 42 women who received the vaccine while pregnant, 18 experienced side effects
ranging from spontaneous abortion to fetal abnormities.
Side effects published by Merck & Co. warn the public about potential pain, fever,
nausea, dizziness and itching after receiving the vaccine. Indeed, 77% of the
adverse reactions reported are typical side effects to vaccinations. But other more
serious side effects reported include paralysis, Bells Palsy, Guillain-Barre
Syndrome, and seizures.
"The FDA adverse event reports on the HPV vaccine read like a catalog of horrors,"
stated Judicial Watch President Tom Fitton. "Any state or local government now
beset by Merck's lobbying campaigns to mandate this HPV vaccine for young girls
ought to take a look at these adverse health reports. It looks as if an unproven
vaccine with dangerous side effects is being pushed as a miracle drug."
Judicial Watch filed its request on May 9, 2007, and received the adverse event
reports from the FDA on May 15, 2007. Judicial Watch has posted the adverse event
reports below.
(A recent study, published in the New England Journal of Medicine, also questioned
the general effectiveness of Gardasil.)
###
Click here to
view the Garadsil Related Deaths Reported to VAERS as of May 11, 2007
Click here to
view the Vaccine Adverse Event Reporting System (VAERS)
On July 14th the first report of a serious reaction to the vaccine was filed with the federal Vaccine Adverse Event Reporting System (VAERS). A 16-year-old Illinois girl was vaccinated July 7th and 13 days later developed symptoms eventually diagnosed as Guillian-Barre Syndrome. A 14-year-old girl in the District of Columbia was vaccinated on July 11th and complained of severe pain immediately following the injection, fell off the examining table and experienced a 10 to 15 second fainting spell ending up in the emergency room with a headache and speech problems. The report of this reaction, the first in the nation, was filed on July 14th, 15 days after the ACIP vote.
Six months later, 82 reports of GARDASIL reactions have been submitted to VAERS on behalf of at least 84 young girls and 2 boys.[1] Reaction reports have come in from 21 states and the District of Columbia.[2] Reactions were reported for children and young adults ranging in age from 11 to 27. Of the reports indicating what day the vaccine was given and the reaction occurred, 63 percent stated that the reaction occurred the same day the vaccine was given. All but three of the reports were for reactions that occurred within one week of vaccination.
This document is divided into three sections. The first section describes reaction reports for a number of reported adverse events: neurological symptoms including syncopal episodes and seizures, arthralgia and joint pain, Guillian-Barre Syndrome, and other immunological reactions. The second section addresses concerns related to vaccinating individuals already infected with HPV. The last section discusses issues that need to be
addressed by government regulators and the manufacturer and considerations for clinicians and consumers.
Reported Adverse Events
Presumably, the reactions described below occurred after the first dose of GARDASIL. GARDASIL is given in a three-dose series. None of the reports stated that the children and adults experiencing problems had previously been vaccinated with GARDASIL.
Syncopal Episodes and Seizures. One-quarter of all reports filed after GARDASIL vaccination were for neurologic adverse events including loss of consciousness, syncope, syncopal events and seizures. An additional five reports included symptoms of dizziness and feeling faint.
Syncope is defined as a temporary suspension of consciousness due to generalized cerebral ischemia (inadequate blood flow and lack of oxygen). The reports of syncopal episodes and their descriptions are remarkable. A physician from Washington State reported that in one morning, three patients experienced syncopal episodes. On August 8th another physician's office reported that two patients experienced syncopal episodes on the same day.
Although these reports did not detail what happened to the individuals experiencing these syncopal episodes, other reports did. The 14-year-old DC girl mentioned earlier experienced a syncopal episode combined with amblyopia (poor vision in one eye), abnormal speech, vomiting, and headache. Also experiencing vision problems, a 17-year-old New York girl reported feeling dizzy and her vision went "black for a few seconds" and she turned pale and lips turned purple and she also had fever and chills. Similar to
the DC girl, on July 18th immediately after being vaccinated, a 22-year-old Kentucky woman experienced slurred speech accompanied by pallor and shock. On August 29th, two hours after being vaccinated, a 15-year-old New York girl who had a history of asthma and was on four asthma medications experienced difficulty swallowing prompting a visit to the emergency room. On August 17th, 15 minutes after being vaccinated, a 14-year-old Pennsylvania girl passed out in the car on the way home.
Most of the reports do not describe what happened as a result of the syncopal episode but a few do. One 11-year-old Florida girl fell from the examining table and two Washington girls fell - a 16-year-old girl fell and hit her head on a carpeted concrete surface and a 14-year-old girl fell down and broke her nose.
Whether the 22 girls who experienced syncopal episodes actually experienced atonic seizures cannot be determined from these reports. Four girls, however, displayed observable seizure activity. The 11-year-old Florida girl who fell from the table also displayed "tonic posturing." Tonic posturing is a type of seizure where sustained contraction of muscles in the legs and arms occurs and consciousness is impaired. The 16-year-old Washington girl who fell and hit her head on the floor lost consciousness for one minute and displayed tonic posturing of her right hand. Additionally, a 15-year-old
girl from Virginia was described as having "a mild seizure." In California, a 13-year-old girl was walking down the hall after her vaccination, fell and had a 15-second tonic/clonic seizure. Tonic/clonic seizures are also known as "grand mal" seizures.
Additionally, there were reports of dyskinesia (difficulty or distortion in performing voluntary movements) and hypokinesia (slow or diminished movement of the body musculature) both of which have neurological implications.
Arthralgia, Joint Pain and Fever. Arthralgia is defined as pain in the joints. Concerns about arthritis were raised during the GARDASIL clinical trials. Reports of arthralgia in one or more joints accompanied by fever were noted in five instances from four young girls and women in Wisconsin, Texas and New York, and one 18-year-old New York male.
Guillain-Barre Syndrome. Reports state that two recently vaccinated 16-year-old girls - one from Illinois and the other from Mississippi - were diagnosed with Guillian-Barre Syndrome (GBS) following vaccination with GARDASIL. In both cases, the onset of symptoms occurred 13 days after vaccination. According to the National Institute for Neurological Disorders and Stroke:
GBS is a serious disorder in which the body's immune system attacks part of the peripheral nervous system. The first symptoms of this disorder include varying degrees of weakness or tingling sensations in the legs. In many instances, the weakness and abnormal sensations spread to the arms and upper body. These symptoms can increase in intensity until certain muscles cannot be used at all and, when severe, the patient is almost totally paralyzed. ... Vaccinations can trigger onset of GBS.
The Illinois girl described earlier was vaccinated on July 7th and symptoms were evident by July 20th. The girl also experienced gait abnormalities (trouble walking properly), asthenia (weakness without loss of strength), paresthesia (burning, prickling, tingling or numbness sensation usually felt in the hands, arms, feet and legs), and hyperkinesia (abnormal increase in muscle movement). The Mississippi girl was vaccinated on July 31st and by August 13th she had increasing numbness and tingling in her feet and hands
and was subsequently evaluated by a neurologist and diagnosed with GBS. The current health status of these girls is not known.
In both of these cases, the girls were also vaccinated with Aventis Pasteur's Menactra, a vaccine for meningococcal infections. Menactra has previously been associated with Guillain-Barre Syndrome, and the FDA and others have issued alerts.
Other Adverse Reactions.
Additionally, a number of other reactions to GARDASIL are noted in VAERS reports and they include: urticaria (hives); pruritus (itching); macular and papular rashes; blisters and vesicles near the injection site; swollen arms; lymphadenopathy (swollen lymph nodes); red, hot swollen knots at injection site; burning, stabbing, severe and
radiating pain at the injection site and in the affected limb during and after injection; nausea and vomiting; infections and skin ulcers, and other allergic reactions.
Other Considerations
GARDASIL is marketed as a "cervical cancer vaccine" and intended to prevent infection with specific HPVs - common viruses among sexually active women. It isn't clear what benefits or potential harms could arise from vaccinating sexually active women who have already contracted HPV. Of the 86 reaction reports filed with VAERS so far, 12 reports were generated by young women 18 and older who were taking hormonal contraceptives and presumably sexually active.
With respect to concerns related to vaccinating women with known HPV infections, adverse reaction reports were filed on behalf of a 17-year-old Texas girl who was already diagnosed with HPV and genital warts. Similarly, the 22 year-old Kentucky woman who experienced slurred speech following vaccination already had an abnormal pap smear with evidence of cervical dysplasia.
Implications
The early reports of potential safety problems with GARDASIL raise concerns and questions that need to be addressed by government regulators, manufacturers and prescribing physicians. Specifically, the following concerns need to be addressed:
1. Syncope, seizures and Guillian-Barre Syndrome have now beenreported with hours to a week after GARDASIL vaccination. GARDASIL manufacturer, Merck, should add these serious adverse events to the product manufacturer insert.
2. Considering that over 20 girls have experienced syncopal episodes sometimes combined with seizures and serious injuries, physicians should consider only giving GARDASIL when the patient is safely laying down on the examining table. Because there seems to be syncopal reactions up until 15 minutes after vaccination, patients should be asked to lie down for 15 minutes after receipt of GARDASIL.
3. The information provided by Merck indicates that it is safe to administer GARDASIL with Hepatitis B vaccine. The prescribing information states, "Results for clinical studies indicate that GARDASIL may be administered concomitantly (at a separate injection site) with hepatitis B vaccine (recombinant). Co-administration of GARDASIL with other vaccines has not been studied." Due to the small number of girls aged 9 to 15 who appear to have been evaluated for GARDASIL safety in Merck clinical trials
(fewer than 2,000) and lack of publicly available information about how many of these girls were given GARDASIL and hepatitis B vaccine simultaneously, the safety of administering GARDASIL and hepatitis B vaccine to all pre-adolescent girls is uncertain.
4. Aside from Hepatitis B, Merck does not state that it is safe to simultaneously administer GARDASIL with any other vaccine. Considering that there are ongoing evaluations of a reported association between Menactra (meningococcal vaccine) and Guillain-Barre Syndrome, and Merck does not explicitly indicate that it is safe to administer to administer GARDASIL and Menactra simultaneously, consumers and clinicians should question whether administering both GARDASIL and Menactra at the same time is safe.
5. Similarly, adverse reactions were reported when GARDASIL was administered with eight other vaccines: Hepatitis A, MNQ (?), MEN (Menactra), TD (Tetanus and Diptheria Toxoids), DPP (Diptheria/Pertussis/Polio), PNC Prevnar (Heptavalent pneumococca conjugate), DTaP (Diphtheria And Tetanus Toxoids and Acellular Pertussis Vaccine), and TDAP (Tetanus, Diptheria and Pertussis). Because Merck does not state that it is safe to administer simultaneously GARDASIL with any vaccine other than Hepatitis B, consumers and clinicians should question whether co-administration of GARDASIL and other vaccines is safe.
6. Most, if not all, of the reactions reported to VAERS were in response to the first of the three doses of GARDASIL. The Centers for Disease Control (CDC) Vaccine Information Sheet (VIS) developed for HPV vaccine states that severe reactions include "any unusual condition, such as a high fever or behavior changes. Signs of a serious allergic reaction can include difficulty breathing, hoarseness or wheezing, hives, paleness, weakness, a fast heart beat or dizziness." The CDC also states that "anyone who has ever had a life-threatening allergic reaction to yeast, to any other component of HPV vaccine, or to a previous dose of HPV vaccine should not get the vaccine." Which of the reactions reported to VAERS constitute a "life-threatening allergic reaction" and which, if any, of the children and young adults who experienced reactions should receive additional doses of vaccine? At the October 2006 ACIP meeting, CDC staff stated that only "three serious reports were reported to VAERS after HPV vaccination in females 14 and 16 years of age. One of these patients had vasovagal syncope and was hospitalized overnight for observation." [7]CDC's summary of the first 76 VAERS reports suggests that CDC doesn't regard the remaining reports as "serious." CDC needs to clarify which of the reactions reported to VAERS constitute contraindications to further vaccination with GARDASIL and make this information available to the public and to prescribing physicians.
7. What were the short and longer-term outcomes for the individuals who experienced the reactions reported to VAERS? Is there information available that would help to predict the characteristics that predispose one to be at greatest risk of experiencing a serious reaction?
8. The CDC's Vaccine Information Sheet indicates that allergy to yeast is a reason to avoid taking GARDASIL. Merck notes that contraindications to the vaccine include "hypersensitivity to the active substances or to any of the recipients of the vaccine. Individuals who develop symptoms indicative of hypersensitivity after receiving a dose of GARDASIL should not receive further doses of GARDASIL." The prescribing information provided by Merck does not specifically note that yeast allergy is a contraindication to taking GARDASIL. Government regulators and the manufacturer need to address the discrepancy between these documents and clarify the issues related to yeast allergy and make this information readily available to the public and prescribing physicians.
9. Additionally, Merck notes that vaccine ingredients include 225 mcg of aluminum (as amorphous aluminum hydroxyphosphate sulfate adjuvant), 0.78 mg of L-histidine, 50 mcg of polysorbate 80, and 35 mcg of sodium borate. These ingredients are not listed on the CDC's VIS sheet. The public needs this information so that they can identify whether they have "hypersensitivities" to any of the ingredients and whether they are at risk of experiencing a serious allergic reaction. Hypersensitivities and known allergic reactions are critical pieces of information that need to be communicated to prescribing physicians in order to make the safest possible vaccination decisions.
Government regulators including the CDC and FDA, in combination with Merck, should address the above safety concerns as soon as possible. Medical groups advocating use of GARDASIL should effectively communicate to physicians and patients the potential risks of using GARDASIL along with precautions to improve the safety of patient care.
Dear Keven,
I posted a bunch of info on Gardasil deaths/adverse reactions to date. The webmaster, however, is "holding" this info. I guess it probably won't be posted here. Its ashame. Email me directly at amanioti@uic.edu, and I will send you the info if these folks censor my post.
With sadness,
Andy
Dear Keven,
Second try to post:
For Immediate Release
May 23, 2007 Contact: Press Office
202-646-5188
Judicial Watch Uncovers Three Deaths Relating to HPV Vaccine
Event Reports Obtained from FDA Detail 1,637 Adverse Reactions to Gardasil
(Washington, DC) -- Judicial Watch, the public interest group that investigates and
prosecutes government corruption, today released documents obtained from the U.S.
Food and Drug Administration (FDA) under the provisions of the Freedom of
Information Act, detailing 1,637 reports of adverse reactions to the vaccination for
human papillomavirus (HPV), Gardasil. Three deaths were related to the vaccine.
One physician's assistant reported that a female patient "died of a blood clot three
hours after getting the Gardasil vaccine." Two other reports, on girls 12 and 19,
reported deaths relating to heart problems and/or blood clotting.
As of May 11, 2007, the 1,637 adverse vaccination reactions reported to the FDA via
the Vaccine Adverse Event Reporting System (VAERS) included 371 serious reactions.
Of the 42 women who received the vaccine while pregnant, 18 experienced side effects
ranging from spontaneous abortion to fetal abnormities.
Side effects published by Merck & Co. warn the public about potential pain, fever,
nausea, dizziness and itching after receiving the vaccine. Indeed, 77% of the
adverse reactions reported are typical side effects to vaccinations. But other more
serious side effects reported include paralysis, Bells Palsy, Guillain-Barre
Syndrome, and seizures.
"The FDA adverse event reports on the HPV vaccine read like a catalog of horrors,"
stated Judicial Watch President Tom Fitton. "Any state or local government now
beset by Merck's lobbying campaigns to mandate this HPV vaccine for young girls
ought to take a look at these adverse health reports. It looks as if an unproven
vaccine with dangerous side effects is being pushed as a miracle drug."
Judicial Watch filed its request on May 9, 2007, and received the adverse event
reports from the FDA on May 15, 2007. Judicial Watch has posted the adverse event
reports below.
(A recent study, published in the New England Journal of Medicine, also questioned
the general effectiveness of Gardasil.)
###
Click here to
view the Garadsil Related Deaths Reported to VAERS as of May 11, 2007
Click here to
view the Vaccine Adverse Event Reporting System (VAERS) Reports as of May 11, 2007
The early reports of potential safety problems with GARDASIL raise concerns and questions that need to be addressed by government regulators, manufacturers and prescribing physicians. Specifically, the following concerns need to be addressed:
1. Syncope, seizures and Guillian-Barre Syndrome have now been reported with hours to a week after GARDASIL vaccination. GARDASIL manufacturer, Merck, should add these serious adverse events to the product manufacturer insert.
2. Considering that over 20 girls have experienced syncopal episodes sometimes combined with seizures and serious injuries, physicians should consider only giving GARDASIL when the patient is safely laying down on the examining table. Because there seems to be syncopal reactions up until 15 minutes after vaccination, patients should be asked to lie down for 15 minutes after receipt of GARDASIL.
3. The information provided by Merck indicates that it is safe to administer GARDASIL with Hepatitis B vaccine. The prescribing information states, "Results for clinical studies indicate that GARDASIL may be administered concomitantly (at a separate injection site) with hepatitis B vaccine (recombinant). Co-administration of GARDASIL with other vaccines has not been studied." Due to the small number of girls aged 9 to 15 who appear to have been evaluated for GARDASIL safety in Merck clinical trials
(fewer than 2,000) and lack of publicly available information about how many of these girls were given GARDASIL and hepatitis B vaccine simultaneously, the safety of administering GARDASIL and hepatitis B vaccine to all pre-adolescent girls is uncertain.
4. Aside from Hepatitis B, Merck does not state that it is safe to simultaneously administer GARDASIL with any other vaccine. Considering that there are ongoing evaluations of a reported association between Menactra (meningococcal vaccine) and Guillain-Barre Syndrome, and Merck does not explicitly indicate that it is safe to administer to administer GARDASIL and Menactra simultaneously, consumers and clinicians should question whether administering both GARDASIL and Menactra at the same time is safe.
5. Similarly, adverse reactions were reported when GARDASIL was administered with eight other vaccines: Hepatitis A, MNQ (?), MEN (Menactra), TD (Tetanus and Diptheria Toxoids), DPP (Diptheria/Pertussis/Polio), PNC Prevnar (Heptavalent pneumococca conjugate), DTaP (Diphtheria And Tetanus Toxoids and Acellular Pertussis Vaccine), and TDAP (Tetanus, Diptheria and Pertussis). Because Merck does not state that it is safe to administer simultaneously GARDASIL with any vaccine other than Hepatitis B, consumers and clinicians should question whether co-administration of GARDASIL and other vaccines is safe.
6. Most, if not all, of the reactions reported to VAERS were in response to the first of the three doses of GARDASIL. The Centers for Disease Control (CDC) Vaccine Information Sheet (VIS) developed for HPV vaccine states that severe reactions include "any unusual condition, such as a high fever or behavior changes. Signs of a serious allergic reaction can include difficulty breathing, hoarseness or wheezing, hives, paleness, weakness, a fast heart beat or dizziness." The CDC also states that "anyone who has ever had a life-threatening allergic reaction to yeast, to any other component of HPV vaccine, or to a previous dose of HPV vaccine should not get the vaccine." Which of the reactions reported to VAERS constitute a "life-threatening allergic reaction" and which, if any, of the children and young adults who experienced reactions should receive additional doses of vaccine? At the October 2006 ACIP meeting, CDC staff stated that only "three serious reports were reported to VAERS after HPV vaccination in females 14 and 16 years of age. One of these patients had vasovagal syncope and was hospitalized overnight for observation." [7]CDC's summary of the first 76 VAERS reports suggests that CDC doesn't regard the remaining reports as "serious." CDC needs to clarify which of the reactions reported to VAERS constitute contraindications to further vaccination with GARDASIL and make this information available to the public and to prescribing physicians.
7. What were the short and longer-term outcomes for the individuals who experienced the reactions reported to VAERS? Is there information available that would help to predict the characteristics that predispose one to be at greatest risk of experiencing a serious reaction?
8. The CDC's Vaccine Information Sheet indicates that allergy to yeast is a reason to avoid taking GARDASIL. Merck notes that contraindications to the vaccine include "hypersensitivity to the active substances or to any of the recipients of the vaccine. Individuals who develop symptoms indicative of hypersensitivity after receiving a dose of GARDASIL should not receive further doses of GARDASIL." The prescribing information provided by Merck does not specifically note that yeast allergy is a contraindication to taking GARDASIL. Government regulators and the manufacturer need to address the discrepancy between these documents and clarify the issues related to yeast allergy and make this information readily available to the public and prescribing physicians.
9. Additionally, Merck notes that vaccine ingredients include 225 mcg of aluminum (as amorphous aluminum hydroxyphosphate sulfate adjuvant), 0.78 mg of L-histidine, 50 mcg of polysorbate 80, and 35 mcg of sodium borate. These ingredients are not listed on the CDC's VIS sheet. The public needs this information so that they can identify whether they have "hypersensitivities" to any of the ingredients and whether they are at risk of experiencing a serious allergic reaction. Hypersensitivities and known allergic reactions are critical pieces of information that need to be communicated to prescribing physicians in order to make the safest possible vaccination decisions.
Government regulators including the CDC and FDA, in combination with Merck, should address the above safety concerns as soon as possible. Medical groups advocating use of GARDASIL should effectively communicate to physicians and patients the potential risks of using GARDASIL along with precautions to improve the safety of patient care.
Wow Keven Tanna, thanks to your stunning brilliance, I can see that Adele is loosing, and Andy winning this battle of the brains. I never could have figured that out without your careful analysis of the facts on both sides of these complex issues. What can you tell us about the relationship of the current vaccinia virus strains used in smallpox vaccines, to the cowpox strains initially used by Jenner? If you do a little research, I bet the answer will surprise you.
Andy's Defender,
"The article (78) you quote which you feel supports your argument that PCP can occurr in children with normal lymphocyte counts does not in fact support your case.
The study was done on children of DRUG ADDICTS.
The mother of Eliza Jane was NOT a DRUG ADDICT.
This is a very large discrepancy.
In fact, all the studies of pediatric HIV/AIDS are done on drug addict mothers."
Wrong, wrong, and wrong again. 1. Andrew said you can't have PCP and high total cell counts. Categorical statement no exceptions for drug use. The article I gave contradicts him. There are several children reported in this SINGLE article who have above avg cell coutns but still have PCP and some die of it like EJ. 2. I called you an idiot becuase you actlike you know about EJ but you don't even spell her name right. Ok, so I'm not the spelling bee winner either but for gods sake its the little girl's name! 3. Not all HIV babies are born to drug addicts. That's a classic lie from Duesberg. He says the 20 percent or whatever of HIV kids of non drug addicts are normal background of disease! That would make a good epidemiologists choke. Yeah sure most mothers with HIV like 80% got it from drug injection because parenteral transmission is efficient. But not all. And those who did don't all keep taking drugs in pregnancy. ANd others get HIV from sex. Like Maggiore got it from her Italian boyfriend.
Andrew,
"EJ is no medical first. She is a classic b-lactam package insert casualty of allopathic medicine."
Sure, Andrew. That is, if you take symptoms from various types of reaction that don't happen in 48 hour window and put them all together. And then throw in some stuff not in the beta lactam insert like giant cells in the brain (AIDS) p24 in the brain (AIDS) a pneumonia x-ray in the hospital and PCP organisms not just DNA in the lungs (AIDS).
Change the topic, repeat and repeat, say what you want about VAERS and additives and spontaneous abortion blah blah blah. Saying it again don't make it so. Still waiting for that example. Just one other 3 year kid who was "perfectly healthy" who took antibiotic for first time in her life and was dead in 48 hours.
Aetiology readers who know about vaccine science know what the vaccine adverse events reporting system VAERS is. Anytime anyone has a health problem AND had a vaccine recently they can go on the internet and blame it on the vaccine. Most of it is junk. If you have a cold after you get a HPV you can blame it on the vaccine. Auto accident, neck pain, heck you can even report an unwanted pregnancy, maybe the vaccine messed up your pill. The spontaneous abortion thing is really tragic. Do you know how many pregnancies end this way? ACtually most pregnancies. But usually before the mom even knows she's pregnant. A miscarriage is a terrible thing for someone who wants a child and it's understandable to want to blame it on something. So you go online and find Andrew and all these antivaxxer sites and there's your culprit.
Since they don't have any science the antivaxxers use this system that serves a good purpose but I would also call it the Venting Animosyity to Excellent Research Science VAERS.
You can't blame deaths on HPV vaccine unless you've done real studies. You can't blame a PCP death with inflammation in the brain and HIV proteins on beta-lactams either unless you've got studies, mechanisms. You guys don't. You just have a dude with access to PubMed who gives a lot of irrelevant publications kind of like Duesberg used to do.
Andrew is right on this, some parts of reaction science are in their infancy. That puts the burden of proof on the anti-vaxxers and denialists to show what we know so far after years of research is mostly wrong. They haven't done it yet.
Now unlike Andrew who seems to have alot of time I actually do work. I'll be waiting for that paper about the kid who died of antibiotic in 48 hours without ever having one before and got encephalitis and PCP in 48 hours too.
Dr. Maniotis,
Thanks for the info re deaths from the HPV vaccine. Sounds like another, typical, junk science scam - to force vaccinations on people based on thin science and fear-mongering.
Andrew, despite what you might think, the scienceblog community is very anti-censorship, unlike the altie and woo communities. The only people to meet the banhammer that I know of are those that are especially abusive, or on Pharyngula, those who refuse to talk sensibly regarding evolution.
If the automatic filters are holding your comments, it is because it is programmed to catch certain keywords to prevent spam. Also, the entire system is being upgraded because of the traffic the community is receiving. Error messages are not uncommon, and if you get one, go back one page, refresh, and check to see that your post has gone up or not.
Cranks have a tendency to play the conspiracy and paranoia card as soon they see a chance to declare martyrdom. If your ego is so bruised by error messages or moderation, I would suggest that you set up your own blog.
To your comments, your attempts to establish your credibility via short listing your CV into a comment is an appeal to authority. It does nothing to argue your point. Science must stand on its own, without the appeal of names on the marquee. Andy's defender hurt you with a link to google scholar, where your contributing author position on a Medical Hypotheses article (pseudoscience journal with no credibility) and a link to barnesworld (a gathering place for AIDS denialists). From a quick skim of the links on google scholar, these were the only ones related to HIV or AIDS.
The allergic reaction hypothesis is an unlikely to the extreme, especially in light of the positive HIV protein staining in EJ's brain, and PCP in her lungs, and so many other important details. As someone who claims to study and teach on the subject of the progression of diseases, you should know that some disorders and diseases present and progress with variation between pediatric and adult patients. If she was an adult AIDS patient, weight gain and wasting would rule each other out, but she wasn't an adult. Some weight gain in a child is to be expected, but EJ's shallow growth curve and low weight for her age is consistent with pediatric AIDS.
Claims of a political autopsy are particularly unfounded but are expected hand-waving from conspiracy theorists. I can understand the psychological need of Christine Maggiore to deny that she played a role in the tragically short life of her daughter. The response to the autopsy report from Maggiore supporter and multi-conspiracy theory backer, Mohammed Al-Bayati, has been debunked in depth (Many links to other pieces found here also).
Al-Bayati's previous role in claiming vaccine injury in shaken baby cases should be illuminating as to his lack of qualifications, and how his statements should be valued, even after his response is discarded as lacking in evidence.
I wouldn't pay much attention to Andrew Maniotis' delusions. He demonstrated clearly on Hank Barnes' blog last year that he had no idea what the definition of AIDS was (in relation to a patient called Mrs Serrano)
http://barnesworld.blogs.com/barnes_world/2006/09/the_mathematics.html#…
So why should we bother to believe what he alleges to be the truth regarding antibiotic reactions? In fact he is pwned by his own attempts to prove EJ had a reaction:
Funny, I couldn't find any of the following problems listed, all of which EJ had:
Hepatic steatosis
Thymus atrophy
Thymus fibrosis
Encephalitis with giant cell formation
Pneumocystis pneumonia
Failure to thrive
Also there is no evidence to suggest EJ's anemia is more likely to be the result of an amoxicillin reaction (hemolytic anemia may occur in fewer than 1:10000 cases according to the SPC) than due to HIV itself, where anemia is actually very common (3-36% of cases) http://bloodjournal.hematologylibrary.org/cgi/content/full/91/1/301?ck=…
1. You admit EJ did not have a Type I anaphylactic reaction, so this is irrelevant.
2. Even if she did, why did she not have the urticaria, flushing, pruritis, or laryngeal edema?
3. Cardiovascular collapse is more likely to be consequent to hypoxia or sepsis.
Since EJ by definition would have had a "late" reaction, I guess you think she had all these problems too? Well EJ definitely had no signs of SJ syndrome or exfoliative dermatitis, so that leaves only one item, the anemia, which as I indicated above, is more likely to have been due to HIV infection and other intercurrent pathology.
So your own quoted "evidence" that EJ exhibited text book amoxicillin reaction is woefully lacking. Care to give it another go?
To Keven,
First of all, I'd like to be Adele's defender. You point out her lack of publications/young age/credentials as being unworth of my time or effort. She asks questions that require response: she may end up being Obama's or Ralph Nadir's Head of the NIH someday? Credentials don't matter. Well reasoned questions and evidence do. I intend to answer them. She wants me to find a dead 3 year old who died of amoxicillin (because she won't accept the WHO's studies and the others I sent, and I suppose no doctor ever asked her if she was allergic to penicillin before they jabbed her), then so be it! I don't think it will be difficult knowing as many parents who have come to us over the years with their dead children in their arms hours after vaccinations, adverse reactions to SSRI inhibitors because their children don't sit up in school and they are stigmatized as having "problems with their brain chemistry" etc. I need to work some today however, but will try to get to it this weekend.
To Robster:
Contrary to what you say about me:
"Cranks have a tendency to play the conspiracy and paranoia card as soon they see a chance to declare martyrdom. If your ego is so bruised by error messages or moderation, I would suggest that you set up your own blog,"
My statement about the webmaster "holding my info" as I expressed it, was indeed my mistake, that I saw corrected as soon as I tried to repost. It's just that
Tara's other site also rejected everything I tried to post numerous times initially in response to Adele's rebut to my T-cell argument about AIDS being a disease of too many T-cells with which she responded by reminding me (and the world) where my dead father's funeral proceeds were sent, so as a consequence, I don't have a leg to stand on scientifically, and I had felt the need to post on this one to answer Adele's question. Robster, my statement about the webmaster not so much the paranoia of a crank you detect here: its the 25 years of absolute censorship that we have experienced at the hands of Journal Editors like Maddox, the Good 'ol Boys at the helm in Science, the mainstream media, etc., the US government scientists like Fauci and Gallo who won't debate us or allow us to publish a word we have written, or even questions we need to ask, despite some of us being in the actual laboratories that were struggling with the AIDS issues early on, as I was with Kaposi's in Folkman's, as well as "HIV integrase," which I found didn't exist.
Furthermore, as a journal reviewer for a number of both first and second tier journals, I think you are in error when you state that:
"Andy's defender hurt you with a link to google scholar, where your contributing author position on a Medical Hypotheses article (pseudoscience journal with no credibility)"
Some of the most far reaching science that has ever been developed first appeared in Medical Hypotheses. It is a rare exception to the rank and file molecular reductionist crap that has ruined biology. Could I perhaps review some of your work sometime if you submit it to any of the journals I review for?
You shouldn't be so critical of Duesberg: he's not a liar. He's a member of the National Academy of Sciences, a Fogarty Scholar, a cancer researcher, a very compassionate individual (at least I have never known him to say a cruel word about anybody), a husband, and a rather insightful gentlemen. Everything he has said, accept two or three things about the AIDS era, have come true. Remember when Gallo said "HIV" is like getting hit by a truck-you need no co-factors. Why don't you read Montagnier. Or is there something unusual about his sexuality or his mother, or perhaps he likes to surf and watch girls like Karry Mullis was accused of doing? Why don't you read his Lancet article on how treatments in vitro for mycoplasm infections abbrogate "HIV" positivity in vitro for some strange reason.
Montagnier et al., in their AIDS denialism went even so far as to suggest that "HIV" is not only not necessary, but a different pathogenic cause, mycoplasms, may cause B (immune collapse):
In a 1991 paper that was published in the journal, Virology (Laurent-Crawford, A. G., Krust, B., Muller, S., Rivière, Y., Rey-Cuillé, M.-A., Béhet, J.-M., Montagnier, L. & Hovanessian, A. G. The Cytopathic Effect of HIV is Associated with Apoptosis. Virol. 185:829-839, 1991), Montagnier and his colleagues not only denied the A,B,C's of "HIV" pathogenesis by asserting that PHA was essential for T-cell activation, but they suggested in addition, that mycoplasma played some role in "HIV" pathogenesis. In postulating a role for mycoplasma, the normal sequence of cause and effect during viral replication is reversed, because maximal viral production succeeded instead of preceded, the maximum number of viable virus-producing cells, thus violating what is known about viral replication being dependent on the presence rather than an absence of cells:
" in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, whereas maximal virus production occurred at Days 10-17."
Cell culturists know that mycoplasma infections generate confusion, because they exert cytoplathic effects on cells similar to the way the "AIDS-virus" is believed to act in humans. Cells become "weakened" by this infectious pathogen over time, but cells are not killed outright, as in lytic viral infections.
But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7. For this to occur, Montagnier et al. would have us forget what is known about viruses. The production of viruses, and there are no exceptions, requires that viruses hijack cellular machinery and cellular materials such as cellular nucleic acids, cellular proteins, and cellular lipids to make more intact virions. Thus viral replication requires cells, not a lack of cells, to replicate, and maximal production of virus should precede and not succeed maximal cell death. Viruses (V) require cells (B) to make more V. There cannot be more V after V has killed most of B, because there would be no materials with which V can make more V, after most of B is killed off. So how are we supposed to accept the AIDS denialist hypothesis of Montagnier et al., that "HIV" actually produces more "HIV" (A) when there is less B (immune system cells)? This makes no sense.
Luc Montagnier et al., therefore advocated several forms of specific AIDS denialism:
Instead of:
"HIV" (A)-----------Immune collapse---(B)-------------------------AIDS-indicator----(C)
diseases
Montagnier et al. claimed:
(A plus but not minus PHA)------------ (B)------------------------------------------------(C)
And:
(A+Mycoplasma---------------------------(B)------------------------------------------------(C?)
removal agent)
RE: "As someone who claims to study and teach on the subject of the progression of diseases, you should know that some disorders and diseases present and progress with variation between pediatric and adult patients."
I do indeed. But this isn't even relevant to the case of Eliza Jane. People (children, adults, Ryan White, Rudoph Nuriev, Arthur Ash, Michael Glazer's wife and daughter, David Acer (the dentist who committed suicide when the CDC could't prove he'd infected anybody, which he hadn't, and they never even apologized to his relatives for ruining his life), don't die of AIDS in 36 hours, with 10,800 T-cells, while gaining weight, with their organs swollen 50-150% of normal in a few hours due to the extravassation of fluids (mostly from the IV's they gave her in the hospital, with only the distension of the liver was noted upon admission-I guess Christine and her 3 pediatricians are liars and EJ had these organ abnormalities for weeks before she died and they simply hid the distended organs in some baggy clothes-that's it), turning pale, etc. I will have to insist that we must agree to disaggree on the b-lactam late reaction literature I sent in a previous post as not necessarily being done by "idiots" and that you KNOW what all adverse reactions to drugs look like. If you aren't too engaged, would you like to come work for us so you can diagnose the enormous case load we have with your Godlike eye? I'll put a good package together for you.
To Adele,
Sorry to get to you last. But you must forgive me if I disagree with you that you are dead dead dead wrong about:
"That puts the burden of proof on the anti-vaxxers and denialists to show what we know so far after years of research is mostly wrong. They haven't done it yet."
When and if you, your sister or brother or whomever you love has children, I'm sure that you will insist that when a pharmaceutical giant comes knocking on your door with Homeland security in tow with guns drawn, you will want some kind of assurance that whatever poison they are injecting into your cherub's arm will do no harm. The burden of proof is in the court of anyone, and I mean anyone, who wants to inject foreign proteins, adjuvants, or any other shit into the bloodstream of an infant or your child. I have written on this extensively and you can find my work on how to predict epidemics, with references to small pox and every other goddamn vaccine posted on the Doctors For Emergency Perparedness website:
http://www.ddponline.org/vande.htm
Cheers,
andy
What other site?
DT said it much better than me. Antibiotic reaction didn't kill EJ any more than the purple people eater.
Andrew, thank you for your warning about pharmaceutical thugs, but every single one of my children was vaccinated on schedule just like I was when I was a kid. Hundreds of millions of people in this country were vaccinated as children. We're still alive and well. EJ isn't. Trusting the medical establishment is usually the right thing to do. There are bad doctors and it pays to stay informed, but I'll trust my kids' pediatrician over a conspiracy theorist who distorts published studies.
These antivaxxers are unbelievable! They talk about exposing kids to "foreign proteins and shit". Did you ever take an immunology course? A newborn gets exposed to bazillions of "foreign proteins and shit" every day. Immune overload is a lie. Everything outside your own body is "foreign". The entire antivax movement is built on fear and misunderstanding and preys on wellmeaning parents. Like I said before, its comfortable if you can blame someone when a child dies or when you miscarry. So you blame it on something you ate or a vaccine you had even without evidence. And people like the antivaxxers are there to help you support you and of course take your money. I mean contributions.
Dear Tara,
I found while I was searching for some articles that my name was being discussed on a site of yours by someone who calls themselves Orac:
"Comments
Is Andrew Maniotis involved somehow? He just showed up in the comments of my post. He didn't mention his HIV/AIDS denialism and didn't really defend Duesberg, but rather cited a whole bunch of his own papers.that begins with a header saying, Well, isn't this interesting..."
[How unfortunate-A Holocaust denier slipped through}
I then saw that many of your bloggers are still confused about the death of Eliza Jane Scovill, and I posted some info, for which I was dismissed by Adele because I contributed money from my father's funeral to Christine's organization in order to help folks who have been stigmatized. So this is the site I couldn't post on after trying for several days.
http://securebar.secure-tunnel.com/cgi-bin/nph-freebar.cgi/110110A/http…
And so I found your Aeteology site, and found Adele posted on there as well so I answered her concerns there. I apologize if this has caused any confusion.
Did you ever get a letter I sent to you last winter?
To Adele,
So how do you like my vaccine timeline and my hypothesis regarding how one can actually predict epidemics? What you say is true-newborns are exposed to a universe of antigens everyday-but not mg quantities directly into the bloodstream, and not without passive immunity protecting them until their own immature immune systems kick in.
By the way, everything outside our bodies is not "foreign."
I don't know what "the purple people eater is or who DT is."
Is this information I need to know about? Is it important?
Also, I would " trust my kids' pediatrician over a conspiracy theorist who distorts published studies. I agree, one should preferably avoid them. So we do agree on something here!
Also by the way, the antivaccine movement was begun in full force in England where mandatory vaccine laws were repealed because there was so much morbidity, mahem and death and disfigurement due to mostly the Jennerian doctrin and the small pox innoculations of that era. I believe it is in the timeline I sent so I won't repeat here. It is toward the beginning of the timeline if you don't have time to read the whole thing.
Do you know of a good immunology course I should take?
By the way, do you like to eat fish? Do you like your fish with a little mercury? You like and trust doctors and big pharma and the government agencies like the FDA, right? Well, I hope your children weren't injected with too many vaccines containing ethyl mercury (I known...I know....ethyl mercury is ok for the developing brain-but then, its a matter of dosages). Please have a look at my timeline, but briefly, did you know that:
Despite the 1999/2000 A Joint Statement by the U.S. Public Health Service, the AAFP, the AAP, and ACIP urging manufacturers to remove the preservative thimerosal (ethyl mercury) as soon as possible from vaccines routinely recommended for infants, the potent neurotoxins mercury or aluminum have been and still are used as vaccine preservatives, and studies show that despite their use, many vaccine lots are contaminated with bacteria. More problematic, there is a wealth of evidence that infants (particularly during the 1990's) were injected with as much as 42 times the amount of mercury that is said by the EPA, the ATSDR (Agency for Toxic Substances and Disease Registry), or FDA to be safe (O.1 micrograms/Kg. verus 62.5 micrograms/KG-see David Kirby's new book, Evidence of Harm, page 49):
"When FDA researchers finally did their math and converted the amount of ethylmercury in vaccines from volume percentages to actual weight, they found that most American Children were being exposed to levels in excess of federal limits, especially when calculated in single-day bolus doses. For example, a two-month-old child weighing 5 kilograms could have been exposed to 62.5 micrograms of mercury in a single day. This would have been 125 times more than the EPA limit for that child (0.5 micrograms/day), 42 times more than the ATSDR limit (1.5 micrograms/day), and 31 times more than the FDA limit (2.0 micrograms/day)."
The question is not whether mercury causes autism spectrum disorders, multiple schlerosis, arthritis, and other autoimmune syndromes. The question is, whether, as a parent, you want the Public Health Service to mandate a vaccine such as the hep B vaccine to be given to your child that contains a potent neurotoxin such as mercury at concentrations that exceed FDA, ATSDR, and EPA limits by as much as 42 times, so they won't acquire an STD when they grow up and become promiscuous, needle-sharing heroin users? How could these recommendations possibly be generated by anyone even if they don't like children?
(From Evidence of Harm, by David Kirby).
"On November 13, 2002, when the House of Representatives was about to pass the Homeland Security Bill, some unnamed agent had secretly inserted a last-minute provision into the bill, adding two brief paragraphs onto the massive document before the roll call. The provision would dismiss hundreds of civil suits filed by parents against Eli Lilly and other drug companies for allegedly allowing dangerous levels of mercury into their kid's vaccines. Very few members of Congress knew it was there."
"The language of the {two paragraphs} dismissing the lawsuits was nothing new. It had been drafted the year before-written as part of a larger vaccine injury bill-crafted by a Senator from Tennessee, Bill Frist, a conservative republican with strong ties to the vaccine industry..."
1989- 2003 Explosion of autism in U.S. The incidence of autism (and other related disorders) went from about 1 in 2,500 children to 1 in every 166. Up until about 1989 pre-school children got only 3 vaccines (polio, DPT, MMR). By 1999 the CDC recommended a total of 22 vaccines to be given before children reach the 1st grade, including Hepatitis B, which is given to newborns within the first 24 hours of birth. Many of these vaccines contained mercury. In the 1990s approximately 40 million children were injected with mercury-containing vaccines. The cumulative amount of mercury being given to children in this number of vaccines would be an amount 187 times the EPA daily exposure limit.
Now Adele, I wouldn't want you or your children to miss any vaccines so here I have posted the current recommendation schedual:
Cheers,
andy
Last week, the Centers for Disease Control and Prevention issued new immunization schedules, including the first separate ones for adolescents. The recommendations cover two new vaccines for teenagers: one for the virus that causes cervical cancer and the other for a bacterium that causes meningitis and other diseases.
The agency has updated its recommended list of vaccines several times over the past 15 years, always after lengthy debate. Each state, rather than the C.D.C., decides which vaccines to make compulsory for entry into school. And some new vaccines are recommended rather than required because their prices are so high.
The timing of injections is complex, and must be overseen by a doctor. But in general, these are the recommendations:
By age 6
Polio
Measles
Mumps
Rubella
Chickenpox
Diphtheria
Tetanus
Whooping cough
Hib (meningitis)
PCV (pneumonia)
Rotavirus (diarrhea)
Hepatitis A and B
Flu (annually)
By age 18
Cervical cancer* (Caused by human papillomavirus)
Meningococcus (bacterial infection)
From 18-65
Between ages 18-65, the vaccination you should get depends on risk factors
Flu (annually when available, always after age 50)
Tetanus and diphtheria (every 10 years)
Measles, mumps, rubella, chicken-pox (for everyone not previously infected)
Some high-risk categories:
MULTIPLE DISEASES: Military recruits, health care workers, emergency
responders, sewer workers
HEPATITIS: Gay men, sex workers, drug injectors
PLAGUE, RABIES: Veterinarians, animal handlers
ANTHRAX: Hide handlers
BY REGION: Travelers and immigrants may need vaccination, depending on their location. People with compromised immune systems should not take some vaccines.
By age 65
Pneumococcal pneumonia flu (annually)
*Girls only; an HPV vaccine for boys is being developed.
(Source by Centers for Disease Control and Prevention)
Robster, my statement about the webmaster not so much the paranoia of a crank you detect here: its the 25 years of absolute censorship that we have experienced...
Responding to suggestions of paranoia with paranoid delusions? Duesberg's lifestyle/behavior hypothesis was found lacking in evidence compared to the HIV/AIDS hypothesis. That is why the denialists have to rely on lowest tier journals.
...the US government scientists like Fauci and Gallo who won't debate us or allow us to publish a word we have written,
Debate suggests that the opposition has some level of credibility, which the denialists lack. Scientific debate occurs in scientific journals. If you had real evidence instead of hanging on to discredited hypotheses, publishing in journals wouldn't be a problem. The HIV denialists have certainly managed to publish quite a few books, so the "allow us to publish a word" claim is silly.
You shouldn't be so critical of Duesberg: he's not a liar.
If he isn't a liar, then he is deluded. Good scientists can admit that they are wrong in the face of overwhelming evidence. Duesberg isn't such an individual.
He's a member of the National Academy of Sciences, a Fogarty Scholar, a cancer researcher, a very compassionate individual (at least I have never known him to say a cruel word about anybody), a husband, and a rather insightful gentlemen. Everything he has said, accept two or three things about the AIDS era, have come true. Remember when Gallo said "HIV" is like getting hit by a truck-you need no co-factors. Why don't you read Montagnier. Or is there something unusual about his sexuality or his mother, or perhaps he likes to surf and watch girls like Karry Mullis was accused of doing? Why don't you read his Lancet article on how treatments in vitro for mycoplasm infections abbrogate "HIV" positivity in vitro for some strange reason.
Appeal to authority, prophetic capacity, and emotion, straw men, ad hominem, did I miss any? I have read some Montagnier, and do not find it to suggest that HIV is not the cause of AIDS in any manner.
But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7. For this to occur, Montagnier et al. would have us forget what is known about viruses.
Some cells die off in a large number. Some cells survive and proceed to become major producers of virus.
Some of the most far reaching science that has ever been developed first appeared in Medical Hypotheses.
ROTFLMAO. I'm calling your bluff. Name one.
Could I perhaps review some of your work sometime if you submit it to any of the journals I review for?
Not likely. You don't show up on any of the editorial boards that I would typically send papers to. Which ones let you review?
People (...), don't die of AIDS in 36 hours, with 10,800 T-cells, while gaining weight, with their organs swollen 50-150% of normal in a few hours due to the extravassation of fluids (mostly from the IV's they gave her in the hospital, with only the distension of the liver was noted upon admission
EJ had AIDS for more than 36 hours. She was very small for her age, and growing but growing slowly (expected for pediatric AIDS). If Christine had mentioned to the hospital that EJ might have been HIV+, they might have looked for more serious signs and symptoms, and PCP would have been checked for immediately. But denying the existence of HIV kind of precludes such doctor/ parent interactions.
How may of the T cells were CD4+ cells? That is the important number.
I guess Christine and her 3 pediatricians are liars and EJ had these organ abnormalities for weeks before she died and they simply hid the distended organs in some baggy clothes-that's it), turning pale, etc.
Well, the pediatricians are certainly remiss and partly at fault for not insisting on testing EJ, or including the possibility in their diagnostic progress. EJ's honesty or at least her grasp of reality, should certainly be questioned.
I will have to insist that we must agree to disaggree on the b-lactam late reaction literature I sent in a previous post as not necessarily being done by "idiots" and that you KNOW what all adverse reactions to drugs look like. If you aren't too engaged, would you like to come work for us so you can diagnose the enormous case load we have with your Godlike eye? I'll put a good package together for you.
Sarcasm much? As a toxicologist, I do know a little bit about what allergic reactions look like, and EJ's death was almost certainly not one, especially when compared to the accepted postmortem diagnosis of pediatric AIDS with PCP.
When and if you, your sister or brother or whomever you love has children, I'm sure that you will insist that when a pharmaceutical giant comes knocking on your door with Homeland security in tow with guns drawn, you will want some kind of assurance that whatever poison they are injecting into your cherub's arm will do no harm.
Wow. An appeal to fear? Are you for real? Ripping off antivax fanfic?
I have written on this extensively and you can find my work on how to predict epidemics, with references to small pox and every other goddamn vaccine posted on the Doctors For Emergency Perparedness website:
I gotta say, go and check out this site. Some of their agenda is reasonable (light residential DDT use, maybe some of the terror articles (don't have time to read them right now)) but their printing of anti-global warming statements, antivax junk including mercury, lots of HIV denialism, linking to junkscience dot com, JAPS, etc... It isn't a place that I would tell people that I was part of.
Andrew, Quoting Kirby? Playing the mercury militia game?
Sad.
Andy Maniotis is absolutely correct in his discussion of the problems with HIV/AIDS science, which can be described simply as an absence of good science, and about the adverse risks and dubious benefits of some of the recently invented childhood vaccinations such as Gardasil.
Rather than give us useful products backed by sound science, the drug giants use the lobby system to influence state legislatures, and television advertising to generate manufactured consent for their products.
Gardisil Objections Listed:
1. The vaccine is costly.
2. Lack of testing in 9-13 yr olds.
3. Lack of evidence of duration of protection
4. Efficacy has not been demonstrated and is unknown.
5. Benefit of Gardasil to 9-13 year olds is dubious. Cervical Cancer affects 45-55 year olds, 40 years later.
6. Questionable Safety when used in conjunction with other vaccines (Hep B and Meningitis ).
7. High rate of vaccine injury: the US Vaccine Adverse Event Reporting System is showing considerable serious injury from this vaccine, especially neurological and immune dysfunction. Included are reports of collapse, paralysis, Guillain-Barre syndrome, dizziness, vomiting, rash, syncope, seizures and headache.
8. Gardasil may actually cause an increase in cervical cancer due to a false feeling of security in the females who receive it and decline PAP smears.
9. Gardasil does not guarantee safety from HPV: Regular Pap screening tests with their incumbent costs will still be needed.
10. The incidence of cervical cancer is low, and it would cost $360 million to pay for vaccine to prevent only 1-2 deaths.
11. HPV is usually benign: The virus clears up on its own within 8-12 months.
12. Pap screening already works and has been very effective in reducing cervical cancer rates.
A common myth is that Vaccinations are mandatory.
They are NOT. There are three types of exemptions:
1) Medical exemption - all states.
2) Religious exemptions - 47 states.
3) Philosophical exemption - 22 states.
HPV Vaccine trial showed only modest efficacy of 20%.
"a cautious approach may be warranted in light of important unanswered questions about overall vaccine effectiveness, duration of protection, and adverse effects that may emerge over time." authors of above reference.
Andrew, I only have one "site" where I discuss any of this, and that's this blog. I don't know if accessing it through that securebar site messed up your comments or not, or if it was the server issue (we just had an upgrade on June 2nd to add an additional server and comments were down for several hours). Since Aetiology's inception, both here and at the former blogspot location, I've only banned maybe 5 comments total (out of close to 11,000 total comments according to moveable type), and those were from Harvey and "Lincoln"/Michael Geiger for being absolutely beyond the pale as far as insults. As others mentioned, some comments occasionally get sent to a junk folder if they contain multiple links or certain words commonly used by spammers, but I "rescue" those the next time I check the control panel. No one has been silenced here.
I for one am interested in how Dr. Maniotis proved that HIV integrase does not exist.
To establish my credentials in the relevant field, I have at various times in the past proven that:
PCR does not work
humans do not have chromosomes
plants do not have DNA
bacteria do not have DNA
Southern blots do not work
....
Hi Andrew,
I just have a couple of questions in response to your post "to Dale and Adele" and your subsequent post describing your opinion of the cause of EJ's death.
1. How does your experience with in vitro models of carcinogenesis qualify you to recognize a 'classic delayed hypersensitivity reaction' ?
2. In your reading of the extensive literature dealing with such reactions, how often are they estimated to occur in response to beta lactams in individuals with no prior exposure to these drugs?
3. In your reading what did you find to be the frequency of lethal allergic reactions to beta-lactams?
4. Could you provide some examples of " all these predictions of Peter Duesberg that have come true"?
Dear Tara,
There is no problem-I said I made a mistake re: the posting, and it posted the second time. Thank you for the openness you are maintaining on the site. Some good exchanges/ideas from various folks, No?
To Robster:
RE:
"That is why the denialists have to rely on lowest tier journals."
"Debate suggests that the opposition has some level of credibility, which the denialists lack. Scientific debate occurs in scientific journals. If you had real evidence instead of hanging on to discredited hypotheses, publishing in journals wouldn't be a problem."
The first problem I have with your thoughtful reply is that I don't know your real name, so how on earth could I send you a manuscript that you would never publish in your "elite" journals? Perhaps I could send it through a friend or two, who would relay it to you through a P.O box?
With respect to Medical Hypotheses, The Journal of Theoretical Biology, and others, that aren't considered worthy, and regarding your challenge, the idea that pathogenic viruses change DNA in a short time began as an article in the journal Medical hypothesis (Papadopulos-Eleopulos E, Turner VF, Papadimitriou J, Page B, Causer D, Alfonso H, Mhlongo S, Miller T, Maniotis A, Fiala C. A critique of the Montagnier evidence for the HIV/AIDS hypothesis.
Med Hypotheses. 2004;63(4):597-601), which asked the question why the AIDS establishment used reverse transcriptase as a marker for "HIV" for nearly 2 decades after Nobelist, Howard Temin who discovered reverse transcriptase (RT), and Nobelist and former NIH head Harold Varmus, claimed that reverse transcriptase "is a normal protein found in the uninfected cells of yeasts, insects and mammals [6]." More recently, other investigators have claimed RT is important for telomere replication at the tips of normal chromosomes [7], and has nothing to do with retroviruses. Once claimed by AIDS scientists to be a specific component required for "HIV" replication, RT is now seen in market magazines concerning biotechnology stocks [8, 9], and is thought to exist in a variety of normal, non-pathological contexts.
p24, another protein once thought to be unique to "HIV" is known to be expressed in the thymus glands of "HIV-negative children [10]." Other studies show that goats and cows test positive for proteins once thought to be derived from "retroviral HIV," and yet do not develop "GAIDS" or "CAIDS" [11] (Goat Acquired Immune Deficiency Syndrome or Cow Acquired Immune Deficiency Syndrome), while 50% of dogs also exhibit "HIV" structural proteins but do not develop "AIDS" either [12]. Extensive work testing the ability of "HIV" integrase to interact with chromosomes derived from normal endothelial cells showed that the enzyme has no activity when compared side by side with histone H1, or the topoisomerases [13].
If those open minded and non-censored journals such as Nature, Science, etc. are your only truth-harboring journals you have found, then try reading the work of Mina Bissell, who came up with the idea of dynamic reciprocity in the context of how normal breast epithelium and breast cancer cells relay information between the extracellular matrix, and the genome Bissell MJ, Hall HG, Parry G. How does the extracellular matrix direct gene expression?
J Theor Biol. 1982 Nov 7;99(1):31-68). Even Robert Weinberg has written reviews in praise of it in recent years because the genocentric model has failed utterly, despite the billions invested in the "oncogene" myth. Bissell's ideas, for example, published in this lowly journal, have materialized at the NCI and world-wide in the form of the marvelous models she and her group(s) has (have) devised to begin to make sense out of testing cancer drugs in 3-D contexts. Therapeutics for cancer, alas, should after all be tested finally on cells behaving as they do in tissues, and with her Journal of Theoretical Biology paper, she (and others) eventually established the experimental basis for the reversion of breast cancer using simple ECM molecules found in embryos, and other agents.
You can find something she helped me write recently in and on the journal cover of last month's The American Journal of Pathology (another low-tier journal that accepts our stuff from time to time).
(http://ajp.amjpathol.org/content/vol170/issue5/).
If you are interested in viruses, you might find it interesting that, using Bissell's system, we found by accident a new way to test for viral pathogenicity and DNA exposure in samples harboring less than 0.01PFU in 2 hours, based on DNA sequestration and exposure tests and cell lysis (which was the way we determined that breast cancer DNA reverts to normal, following Bissell's dynamic reciprocity hypothesis, which is why DNA is epigenitically reversible, and applicable to real virus infections, and why aneuploidy doesn't drive cancer-it follows it, in contrast to other celebrated hypotheses recently discussed at some length).
You can get the virus articles if you send my your email at: (http://www.ncbi.nlm.nih.gov/sites/entrez?
Db=pubmed&Cmd=ShowDetailView&TermToSearch=
17386925&ordinalpos=3&itool=EntrezSystem2.
PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_
RVDocSum)
Or you need to cough up some money...for the article.
I can't wait to test "HIV" in this new system ( I call it the RILA assay-Rapid Infectivity and Lysis Assay). It doesn't require PHA or IL2 to get a readout. Only a real viruses.
Finally, I'm not really "a denialist" who wants to debate anybody, as you put it. All I want is some clarification. You all are obviously very clever, experienced, folks, and have an ability to rapidly change the focus of the discussion (it is too deep at times for me to follow), to the point that I keep getting confused.
Therefore, I am asking you, no I am pleading with you, I am shouting it out to you to please, please tell me, once and for all:
IS AIDS A DISEASE OF TOO FEW LYMPHOCYTES, OR TOO MANY LYMPHOCYTES, AS IN THE CASE OF ELIZA JANE? COULD SOMEBODY PLEASE GIVE ME AN EITHER OR ANSWER!!!! I CAN'T HANDLE IT ANY LONGER!!
I KNOW YOU DON'T GOT TO HAVE "HIV" TO HAVE AIDS BECAUSE FAUCI INVENTED ICL AIDS, WHICH IS AIDS WITHOUT ANY "HIV" IN IT.
I KNOW "THE LIFE-SAVING" ANTIRETROVIRAL DRUGS SAVE VIRTUALLY EVERYBODY WHO TAKES THEM, AND THAT THERE IS NO CURE TO AIDS (Those good ol "HIV" vaccines ARE IN THE PIPELINE, THOUGH, to come I suppose-when they get their next installment of 875 million award for failing the AIDSVAX trial, which was severaly underfunded at 120 million).
I KNOW "HIV" HAS BEEN ISOLATED BECAUSE MONTAGNIER PLACED THE BLOOD SAMPLES FROM PATIENT 1 ON HIS LYMPHOCYTE CULTURES (Barre-Sinoussi, F,m J.C. Chermann J.C., Rey F., Nugeyre MT., Chamaret, S., Gruest J., Dauguet C., , Axler-Blin C., Vezinet-Brn F., Rouzioux, C., Rozenbaum R., & Montagnier L. 1983 Isolation of a T-lymphotropic retrovirus from a patient at risk for Acquired Immune Deficiency Syndrome. Science 230: 868-871),
WHO HAD HAD 2 CASES OF GONORRHEA, HAD BEEN TREATED FOR SYPHILIS THE YEAR BEFORE, HAD HAD HERPES I AND II, AND CMV-(MAKING HIS SERUM AN IDEAL CHOICE TO TEST THE FIRST "HIV" ISOLATES, AND THEN OF COURSE TO "LOAN IT" TO GALLO TO "AMPLIFY IT"), AND I KNOW "HIV HAS BEEN ISOLATED BECAUSE NO VACCCINE TO DATE, OF THE 30 TESTED, HAVE EVOKED HUMORAL, MUCOSAL, CELLULAR IMMUNITY, OR INDUCED T-CELL ACTIVATION.
I KNOW THAT, UNLIKE EJ'S CASE, THERE IS A WHOLE CONTINENT FULL OF CHILDREN WHO ARE ORPHANS AND DYING LIKE FLIES BY THE THOUSANDS/HOUR BECAUSE OPPORTUNISTIC INFECTIONS FREQUENTLY OCCUR IN AIDS PATIENTS WITH 10,800 LYMPHOCYTES, AND ALSO IN PERSONS HARBORING 1000 OR FEWER LYMPHOCYTES."
ALL THIS IS SO CONFUSING-I'D JUST BE HAPPY WITH AN ANSWER TO MY FIRST AND MOST TROUBLING QUESTION WITHOUT DEBATES, INSULTS, DISMISSALS OF MY QUESTIONS BECAUSE OF WHERE MY FATHER'S FUNERAL PROCEEDS WERE SENT, ETC.
ONE MIGHT THINK THAT THE THOUSANDS OF CHILDREN IN COHORTS IN THE 100,000+ AIDS PAPERS THAT ALL PROVE "HIV" CAUSES AIDS, T-CELL COLLAPSE, WASTING, ETC., THERE WOULD BE SOME EXPLANATION TO ATTEST TO THE FACT THAT WHILE IN EJ'S CASE, AIDS IS A DISEASE OF TOO MANY LYMPHOCYTES, IN VIRTUALLY EVERYBODY ELSE WHO HAS DIED, CHILD OR ADULT, IT IS A DISEASE OF TOO FEW LYMPHOCYTES. AFTER REALIZING (DUE TO YOUR LEARNED COMMENTS) THAT AIDS IS A DISEASE OF 10,800 LYMPHOCYTES, I JUST DON'T SEE ANYMORE HOW I COULD HAVE EVER THOUGHT THAT T-CELLS BELOW 1000/UL) COULD EVER HAVE BEEN MISTAKEN FOR AN AIDS CASE!
A PROBLEM FOR THE NEW DEFINITION:
DOES THE NEW AIDS DEFINITION SET AT 10,800 T-CELLS/UL AND ABOVE MEAN THAT ALL (SOME) (A FEW) (ONE) OF THE CHILDREN WHO HAVE LESS THEN 1000 SUFFER A DIFFERENT DISEASE, ESPECIALLY GIVEN THE FACT THAT CD4 COUNTS, OR BETTER YET AND MORE ACCURATE, ACCORDING TO THE WHO, TOTAL LYMPHOCYTES COUNTS THAT MEET THE DEFINITION OF AIDS MUST FALL ABOVE THE 10,800 CELLS/uL RANGE TO NOW BE CONSIDERED AN AIDS CASE? WHAT DID ALL THE REST OF THOSE THOUSANDS OF AFRICAN ORPHANS WHO ARE DYING EVERY DAY FROM TOO FEW LYMPHOCYTES DIE OF, WHO ARE FORTUNATE NOW TO RECEIVE BUSH'S GENEROUS ROLLOUT OF YET ANOTHER MILLION OR TWO DOSES OF THOSE LIFE-SAVING DRUGS FOR ANOTHER 30 BILLION (I HOPE THEY REMEMBER TO GIVE THE CHILDREN THIS TIME SOME WATER TO WASH DOWN THE PILLS WITH- THEY FORGOT TO THE LAST TIME WHEN CHRISTINE AMMAPOUR DID HER STORY AND FREAKED OUT BECAUSE THE CHILDREN DIDN'T HAVE ANY WATER TO WASH DOWN THEIR NEVIRAPINE WITH).
I THEREFORE PROPOSE FROM HERE ON OUT, THAT, CONTRARY TO THE WHO'S DEFINITION, THAT AIDS CASES ARE THOSE WHOSE T-CELLS ARE AT OR ABOVE 10,800/uL LIKE EJ'S, and all those children dying every day in Africa AND IN PLACES LIKE INCARNATION ARE DYING FROM SOMETHING ELSE.
Ok. I said it. I've calmed down now. Perhaps there is a better definition of AIDS. AIDS is a disease characterized by there being either too many or too few lymphocytes? Then where or what becomes the role of anti-retrovirals? If it is good to have too few lymphcytes because AIDS is really a disease of having 10,800 or more lymphocytes, then who SHOULD you drug, and what will the failed cancer drugs turned into anti-retrovirals (such as 3TC, AZT, ddI) accomplish?
I suppose that since EJ is now the classic AIDS case harboring too many lymphocytes, and because according to the BWelcome package insert AZT causes a profound depression and hematological toxicities to all blood cells, then one should expect a decline in the number of T-cells in true AIDS patients (like EJ) who harbor 10,800 or more lymphocytes as E.J. did, and one should try to bring them down to a lower level (1000 cells/ul or less) so they have some different disease that probably wouldn't be 100% fatal like real AIDS is (except of course in those genetically mutated Long-Term Non-Progressors (Shish!) according to our new way of defining AIDS as a disease of >10,800 cells/ul?
Therefore, we should be maximizing approaches that DECREASE, not INCREASE the number of T-lymphocytes to 1,000 or lower, since EJ is the classic AIDS case (who unfortunately harbored too many T-cells). Radiation might be a good way? It really knocks back the T-cells better than any old AZT! So we ought to nuke em, or just continue leaving depleted uranium rounds lying around there in northern Africa to punish them terrorist Muslims!
I'm glad the problem is resolved, unless there is something I missed?
Robster: Cheers,and thanks so much for the helpful information you provided.
Andy
Take a deep breath Andy...
"IS AIDS A DISEASE OF TOO FEW LYMPHOCYTES, OR TOO MANY LYMPHOCYTES, AS IN THE CASE OF ELIZA JANE? COULD SOMEBODY PLEASE GIVE ME AN EITHER OR ANSWER!!!! I CAN'T HANDLE IT ANY LONGER!!"
Then go to the library and look up "lymphocyte", or even use PubMed or wikipedia if your library is not convenient. You will find that there are doozens of types of lymphocytes. Some (including T-helper cells, macrophages and dendritic cells) carry more CD4 than CD8 molecules on their surface. The ones that carry mostly or exclusively CD8 and not CD4, are often referred to as "killer T-cells". A strong CD8+ T-cell response is often implicated in succuessful vaccine responses, if the vaccine was a live attenuated virus or DNA vaccine.
Anyway Andy, the immunodeficiency that is specific to lentiviral infections is the result of a profound CD4+ T-cell deficiency, without a similar loss of CD8+ T-cells. A few other people in this thread have attempted to explain that to you. Maybe some library research could help you regain a bit of sanity.
Dr. Mantiotis, you are mistaking a surrogate marker of cellular immune deficiency with immune deficiency itself. Peripheral blood CD4 T cell counts are a pretty good surrogate marker for the underlying changes in immune cell homeostasis that cause immune deficiency in HIV infection, but they're not perfect - it's still possible for someone with a relatively high CD4 T cell count to develop an opportunistic infection if the relevant antigen-specific memory T cell population is compromised such that the pathogen can reactivate and cause disease. There are reports of this occurring in both adults and children.
Peripheral blood total lymphocyte counts are not as good a surrogate marker as CD4 T cell counts because they include CD4 T cells, CD8 T cells, B cells, NK cells, NKT cells and gamma-delta T cells. In the Lancet study you cited, between 0.4-20% of children with a TLC of 6000 progressed to AIDS or died (depending on the age bracket) - you could email the authors and ask if there were cases at higher levels (they only present "selected" numbers in the paper). The relevance of those data to EJ is also limited by the fact that the children included in that meta-analysis would have received appropriate care including prophylaxis for opportunistic infections, and OI prophylaxis delays disease progression such that progression events occur when lymphopenia is more severe. You could also email an experienced clinician like James Oleske and ask if PJP has been known to occur in a child with a TLC of 10,000 or above.
The underlying changes in immune cell homeostasis that peripheral counts are a surrogate for include: depletion of naive CD4 and CD8 T cells, elevated CD4 and CD8 T cell activation, increasing memory CD4 and CD8 T cell dysfunction (loss of proliferative capacity and IL-2 production i.e. anergy) and a narrowing of the CD4 and CD8 T cell repertoire. There is also a progressive loss of long-lived central memory T cells accompanied by an increase in the proportion of short-lived effector memory T cells. You can't make a definitive statement about how far this dysregulation has progressed based on a peripheral blood TLC count. CD8 T cells expand in respond to HIV infection, which is why the CD4/CD8 ratio almost immediately skews. In the setting of an active opportunistic infection, any reserves of naive T cells specific for that antigen will expand, and naive T cells divide prodigiously in response to antigen.
The literature makes it clear that acute respiratory failure is the leading cause of ICU admission for HIV-infected children. The most recent study on this subject actually found that higher TLC at admission was associated with an increased risk of mortality.
J Trop Pediatr. 2007 May 25; [Epub ahead of print]
Children with Human Immunodeficiency Virus Infection Admitted to a Paediatric Intensive Care Unit in South Africa.
Rabie H, Boer AD, Bos SV, Cotton MF, Kling S, Goussard P.
Department of Paediatrics and Child Health Tygerberg Children's Hospital & Stellenbosch University, South Africa.
Background: Early data regarding the outcome of human immunodeficiency virus (HIV)-infected children in paediatric intensive care units (PICU) suggested mortality as high as 100%. Recent studies report mortality of 38%. Survival depends on the indication for admission. Objectives: To describe the prevalence, duration of stay, and outcome of HIV-infected patients in a single PICU over a 1-year period. Additional objectives included describing the indications for admission as well as the clinical and laboratory characteristics of HIV-infected infants and children requiring PICU admission. Method: Retrospective chart review of all children with serological proof of HIV admitted to PICU at Tygerberg Children's Hospital from 1 January to 31 December 2003. Results: Of the 465 patients admitted, 47 (10%) were HIV-infected. For HIV-infected children the median age on admission was 4 months. The median duration of stay was 6 days, significantly longer than for the non-HIV group (p = 0.0001). Fifty-seven percent had advanced clinical and immunological disease. Seventeen died in PICU and four shortly afterwards, poor PICU outcome was significantly associated with HIV status (p = 0.001). Lower total lymphocyte count (p = 0.004) and higher gamma globulin level (p = 0.04) were paradoxically the only findings significantly associated with survival. Acute respiratory failure (ARF) accounted for 76% of admissions, including Pneumocystis jiroveci in 38%. Fifty-one percent had evidence of cytomegalovirus infection. Conclusions: HIV-infected children requiring PICU can survive despite the lack of availability of antiretroviral therapy.
Intensive Care Med. 2004 Jan;30(1):113-8. Epub 2003 Nov 13.
Children with human immunodeficiency virus admitted to a paediatric intensive care unit in the United Kingdom over a 10-year period.
Cooper S, Lyall H, Walters S, Tudor-Williams G, Habibi P, de Munter C, Britto J, Nadel S.
Paediatric Intensive Care Unit, QEQM Wing, St Mary's Hospital, Praed Street, London, W2 1NY, UK.
OBJECTIVE: There is little published experience regarding the outcome of children with human immunodeficiency virus (HIV) infection treated on a paediatric intensive care unit (PICU). We describe the outcome of children with HIV infection in our hospital over a 10-year period. METHOD: We performed a retrospective analysis of all children with HIV infection admitted to our PICU between August 1992 and July 2002. Their ages ranged from 2 months to 11 years (median 4 months). Information collected included demographic data, clinical presentation, investigations, treatment and outcome. RESULTS: There were 42 children with HIV infection admitted to PICU during the study period, with 66 admission episodes. Sixteen (38%) children died in PICU, and 26 (62%) survived their last PICU admission. Of these, 5 died at a later date (between 1 and 32 months after discharge from PICU) and 21 survived to the time of reporting. The most frequent reason for PICU admission was respiratory failure, due either to Pneumocystis carinii pneumonia (45% of admissions) or to other respiratory pathogens (32%). Over 80% of current survivors had good outcomes in terms of growth and development; 6 children had evidence of spastic diplegia. CONCLUSIONS: Although there is significant mortality among children with HIV infection admitted to PICU, many of them survive their admission, and over 80% of the survivors have good outcomes with the currently available highly active anti-retroviral therapy. This provides evidence that intensive care treatment is appropriate for this group of patients in the United Kingdom.
An Esp Pediatr. 2000 Jun;52(6):537-41.
[Admissions of patients with AIDS to pediatric intensive care units]
Casanova Roman M, Rios Hurtado J, Garcia Martin FJ, Milano Manso G, Martinez Valverde A.
Unidad de Cuidados Intensivos Pediatricos. Unidad de Enfermedades Infecciosas e Inmunodeficiencias. Departamento de Pediatria. Hospital Materno-Infantil. Complejo Hospitalario Universitario Carlos Haya. Malaga.
OBJECTIVE: To describe the most significant clinical features of children with acquired immunodeficiency syndrome who required admission to a pediatric intensive care unit (PICU). METHODS: Retrospective study of 12 patients with AIDS who required 13 admissions, between January 1988 and December 1997. RESULTS: Mean age at admission was 15 months (1 month-6 years). Seven patients were under 1 year of age; four were diagnosed during their stay in the unit. The most common reason for admission was respiratory failure (six patients), followed by cardiac failure. Six patients needed mechanical ventilation (5 for respiratory failure). Two patients died during their stay, one of pneumonia due to Pneumocystis carinii infection and one of septic shock. CONCLUSIONS: One-third of patients was diagnosed with HIV Infection during their stay at the PICU. Opportunistic infection was the initial manifestation of the disease. Consequently, with this type of infection, clinical suspicion should be high. The survival rate of up to 84.6% of the admissions to our unit as well as the new, highly active antiretroviral therapy, generally make HIV-infected children suitable for treatment in intensive care units.
Crit Care Clin. 1988 Oct;4(4):831-44.
The acquired immunodeficiency syndrome: impact on the pediatric intensive care unit.
Wilkinson JD, Greenwald BM.
Cornell University, New York.
Increasing numbers of infants and children with AIDS are being admitted to the PICU, especially in certain geographic areas. Clear diagnostic criteria are available to aid in the diagnosis. As many as 50 per cent of these patients may be first diagnosed with AIDS during their PICU stay. Most patients are admitted because of ARF, but septic shock and CNS disorders are also common. Acute PICU mortality is in excess of 80 per cent, and presently the long-term mortality for this syndrome stands at 100 per cent. The economic impact of this epidemic is enormous and may become catastrophic if a national strategy to deal with these costs is not developed promptly. The PICU has an important role both in terms of resource use and cost containment. Awareness of unique stresses on medical and nursing staff caring for these children, as well as the unique psychoemotional needs of the patients themselves, is vital. Specific infection control, nutritional, and medical-legal strategies will facilitate safe, effective delivery of care to these infants and children in the PICU. The appropriate long-term role of the PICU in the care of children with an ultimately terminal disease has yet to be determined.
Andrew,
Wow, CAPS LOCK is cruise control for coooool. Heh.
The first problem I have with your thoughtful reply is that I don't know your real name, so how on earth could I send you a manuscript that you would never publish in your "elite" journals?
I don't use my real name as I don't want my student's first exposure to me to come from the impersonal route of a google search.
If I want an article that I can't get through a library subscription, interlibrary loan has yet to fail me. All I wanted to know is what journals do you review for.
You found a worthwhile article from Journal of Theoretical Biology, but not one from Medical Hypotheses (Perth group denialist paper). My statement was against the quality of Medical Hypothesis, as I don't have any familiarity with JTB. If they are publishing papers in support of HIV/AIDS denialism, then the quality of the journal must be suspect.
Finally, I'm not really "a denialist" who wants to debate anybody, as you put it. All I want is some clarification.
Meh. Framing. I hear the same from creationists and 911 conspiracy mongers. They all claim to just want questions answered. You are an HIV/AIDS denialist or dissident, or rethinker. Six of one, half dozen of the other...
IS AIDS A DISEASE OF TOO FEW LYMPHOCYTES, OR TOO MANY LYMPHOCYTES, AS IN THE CASE OF ELIZA JANE? COULD SOMEBODY PLEASE GIVE ME AN EITHER OR ANSWER!!!! I CAN'T HANDLE IT ANY LONGER!!
As a pathologist, are you aware that there are more than one type of lymphocyte? Are you aware that HIV infects and kills CD4+ T Cells (helper lymphocytes)? Why are you attempting to misrepresent the science, specifically stating that AIDS includes the presence of HIV and a CD4+ count of less than 200 cells per microliter of blood, not all lymphocytes? Of the CDC's list of AIDS defining illnesses or conditions in individuals under the age of 13, EJ had several, including hepatomegaly, anemia, PCP, and encephalopathy. Let me know if I missed any.
For those not familiar with the case of EJ, here is the coroner's report and an answer to al-Bayati's questioning of said report. This rebuttal discusses what amoxacillin reaction looks like, as well as what one would expect to see in a pediatric AIDS with PCP case. This should have put an end to the controversy, but denialists and conspiracy theorists have allergic reactions to reality (see above rant).
What you do with your or your late father's money is irrelevant to the evidence, which is clearly against the HIV/AIDS denialists and Maggiore's enablers.
Robster said: "For those not familiar with the case of EJ, here is the coroner's report and Bennet's an answer to al-Bayati's questioning of said report. This rebuttal discusses what amoxacillin reaction looks like, as well as what one would expect to see in a pediatric AIDS with PCP case. This should have put an end to the controversy, but denialists and conspiracy theorists have allergic reactions to reality (see above rant)."
The LA coroner Ribe had a reputation for deceit and dishonesty regarding previous autopsy reports as described in this report from the LA Weekly. "Prosecutors intentionally withheld information about Ribe's inconsistent testimony in other child-death cases"
The rebuttal to Al Bayati by Bennet is questionable for a number of reasons. One, Bennet is am AIDs apologist and heavily involved in the politics of AIDS and hardly an impartial observer. Bennet's credibility has been impugned on previous exchanges on various blogs and, quite frankly, he is not to be trusted.
Two, Bennet himself questions why neither a serum HIV serology report nor a HIV viral load report was included by Ribe in the autopy report. Both are elementary and standard tests for making the diagnosis of HIV, and both conspicuously absent suggesting strongly that the tests were done and results withheld because they were negative. Instead the coroner relied on P24 protein stains on the brain tissue which are not commonly used for diagnosis of HIV in the population of North America.
As Andy mentioned P24 can be found in thymus of HIV negative children.
P24 can be found in normal human placentas:Faulk WP, Labarrere CA. HIV proteins in normal human placentae. American Journal of Reproductive Immunology. 1991;25:99-104,. and it is well known that p24 is prone to "false-positive" reactions.
Regarding the misdiagnosis of pneumonia, whether from PCP or any other agent, here is a further microscopic evaluation of the lung tissue and a rebuttal to Nick Bennet's biased and canted comments.
The Ribe LA autopsy report was a political response not a medical one. There is a huge amount of money and reputations at stake in the politics of HIV. Why else would the tragic death of a little girl be turned into a political football? Andy has shown only a few of the many glaring inconsistencies and "problems" with HIV medical science. Its time to reevaluate the huge amount of tax payer dollars wasted on HIV Non-Science and as taxpayers we all say, " I'm Mad As Hell and Not Going to Take it Any More" Spend the money on more worthy projects.
To all,
Thanks guys for all the info.
I still am hung up on the following (no conspiracy theory cloaked or shuffling of feet here, just curiosity).
Despite the coroner's failure to provide a CD4+/CD8+ ratio in support of the "AIDS diagnosis," it should be emphasized that the accuracy of total lymphocyte counts in predicting death due to "AIDS-associated indicator diseases" is considered equal or even superior to measuring the CD4/CD8 ratio. Therefore, and despite the fact that CD4/CD8 ratios were NOT obtained (by those attributing her death to AIDS after the revised autopsy report was filed some 4 months after the death), absolute lymphocyte numbers were obtained at the hospital, and according to "AIDS experts," they are just as predictive of AIDS-related death in children, if not more so. In a recent study of 3917 children, it was reported that (1):
"For children older than 2 years, the 12-month risk of death and AIDS increased sharply at values less than 1500-2000 cells per microliter, with little trend at higher values." (Eliza Jane's count was 10,800 cells/microliter).
"Mortality risk was substantially higher at thresholds of total lymphocyte count recommended by WHO than at corresponding thresholds of CD4-cell percentage. When the markers were compared at the threshold values at which mortality risks were about equal, total lymphocyte count was as effective as CD4-cell percentage for identifying children before death..."
Do you disagree with the Paediatric Prognostic Markers Collaborative Study?
Were the children with relatively high lymphocyte quantities that supposedly died of AIDS given toxic antiretrovirals, making it appear they died of AIDS (with high lymphocyte counts) because they were "HIV" positive or had "high viral loads," which of course is an impossibility given Karry Mullis's reservations about the misuse and criminal denial of his own reservations about the use of his PCR to detect true viral load?
To Robster:
Ever read the Medical Hypothesis article before branding it AIDS denialism? Do you read things before judging them as heretical?
Thanks much,
Andy
1. HIV Paediatric Prognostic Markers Collaborative Study. Use of total lymphocyte count for informing when to start antiretroviral therapy in HIV-infected children: a meta-analysis of longitudinal data. Lancet. Nov 26;366(9500):1868-74, 2005.
Robster said: "For those not familiar with the case of EJ, here is the coroner's report and Bennet's an answer to al-Bayati's questioning of said report. This rebuttal discusses what amoxacillin reaction looks like, as well as what one would expect to see in a pediatric AIDS with PCP case. This should have put an end to the controversy, but denialists and conspiracy theorists have allergic reactions to reality (see above rant)."
The LA coroner Ribe had a reputation for deceit and dishonesty regarding previous autopsy reports as described in this report from the LA Weekly. "Prosecutors intentionally withheld information about Ribe's inconsistent testimony in other child-death cases"
The rebuttal to Al Bayati by Bennet is questionable for a number of reasons. One, Bennet is am AIDs apologist and heavily involved in the politics of AIDS and hardly an impartial observer. Bennet's credibility has been impugned on previous exchanges on various blogs and, quite frankly, his opinionins are not trustworthy.
Two, Bennet himself questions why neither a serum HIV serology report nor a HIV viral load report was included by Ribe in the autopy report. Both are elementary and standard tests for making the diagnosis of HIV, and both conspicuously absent suggesting strongly that the tests were done and results withheld because they were negative. Instead, the coroner relied on P24 protein stains on the brain tissue which are not commonly used for diagnosis of HIV in the population of North America.
As Andy mentioned P24 can be found in thymus of HIV negative children.
P24 can be found in normal human placentas: Faulk WP, Labarrere CA. HIV proteins in normal human placentae. American Journal of Reproductive Immunology. 1991;25:99-104,.
In fact P24 is NOT a protein entirely unique to HIV, and the P24 test is prone to "false-positive" reactions.
In order for PCP to cause pneumonia, there must be a LOW WBC count indicating immunosuppresion, not a high one. You can't have it both ways. A diagnosis of AIDS and immunosupression is incompatible with a normal lymphocyte count.
Regarding the misdiagnosis of pneumonia, whether from PCP or any other agent, here is a further microscopic evaluation of the lung tissue and a rebuttal to Nick Bennet's biased comments.
The 4 month delayed Ribe LA autopsy report was a political response because there is a huge amount of money and reputations at stake in the politics of HIV. Why else would the tragic death of a little girl be turned into a political football? Andy has shown only a few of the many glaring inconsistencies and "problems" with HIV medical science.
Its time to reevaluate the huge amount of tax payer dollars wasted on HIV by the NIH, and as taxpayers we all say, " I'm Mad As H_ll and Not Going to Take it Any More". After 20 years of highly expensive research at the expense of the taxpayer, we have had no vaccine, no mechanism of disease or cell death, no reasonable drug therapy, no heterosexual epidemic, and a series of failed predictions. HIV research money has become just another pork barrell project like the 200 milion dollar Alaska bridge to an island with 50 people. Inform your legislatures to turn off the money faucets for HIV research, and spend it on more worthy projects.
Sigh. Sigh. Oh my. This is why most scientists refuse to "debate" denialists.
Andrew, everyone here has read that Lancet study. Everyone here has also read several other papers. So we know a child can die of PCP with high total lymphocyte counts. It's rare, sure, but it has happened and has been documented in the papers we gave above and you didn't read. It's also rare for a HIV poz kid in the USA to never get tested, never to get treated, never to have a medical exam taking her potential infection into account, EJ.
Your thing about deaths of kids with high lymphocyte counts is classic Duesberg again. They died of "toxic antiretrovirals" you say. Even though retrovirals have reduced transmission and then mortality until pediatric AIDS in this country is alsmot gone! Their mothers were all drug addicts, you say, even though children of drug addicts don't get these diseases in these numbers unless their HIV positive too. Then you give us this strange Mullis thing. Mullis didn't invent quantitative real-time PCR did he or did I miss it? And so what if he did? Does His Royal LSDness's opinion make PCR complete crap like you say over the evidence from probably ten thousand technicians around the world? Have you done a real-time PCR before, Andrew? I have a bunch. Know what? It works. Have you done a reverse transcriptase assay, Andrew? I have. It works. Yeah, there are cellular RTs, but guess what? They don't mess up your RT! I always use these little things called controls. You know, sups from uninfected cells, and cells infected with a defective virus and whatever you can think of. Noone confuses viral RT with cellular stuff. Do you also post as Gene Semon or Nick Naylor or do you guys just share unscientific idaes?
Arguing with you Andrew is like arguing with a conspiracy theorist or a denialist that's why I call you both. You can say youre neither. Or your really just interested and inquisitive. I don't care. When a point is refuted three times with different arguments and you keep coming back to it with the same old objection, in all caps too, to me you're not a scientist or a colleague. My advice is you get a AM talk radio show. Have you been on coast-to-coast AM? There you can hang with your fans without the inconvenience of facts. Look into it. You have a wide range of conspiracy in your bag and some nice inflammatory rhetoric too so you could do real well. Maybe pick up some 911 stuff and talk about Ruby Ridge more and do shows on fish oil. Youll have the market sown up. Enjoy.
Oh, it's not just AIDS denial. It's all kinds of infectious disease denial...
To Robster, and Adele:
The LA coroner Ribe's reputation was not the best one. See this report from the LA Weekly. "Prosecutors intentionally withheld information about Ribe's inconsistent testimony in other child-death cases"
The author of the rebuttal you quote himself questions why neither a serum HIV serology report nor a HIV viral load report was included by Ribe in the EJ autopy report. Both are elementary and standard tests for making the diagnosis of HIV, and both conspicuously absent. Is it possible that the tests were done and results withheld because they were negative? Instead of the usual HIV tests, the coroner relied on P24 protein stains on the brain tissue, which are not commonly used for diagnosis of HIV in the population of North America or anywhere else on the planet.
As Andy mentioned P24 can be found in thymus of HIV negative children.
P24 can be found in normal human placentas:Faulk WP, Labarrere CA. HIV proteins in normal human placentae. American Journal of Reproductive Immunology. 1991;25:99-104,. and it is well known that p24 is prone to "false-positive" reactions.
Regarding the misdiagnosis of pneumonia, whether from PCP or any other agent, here is a further microscopic evaluation of the lung tissue which shows clear lungs with no evidence of pneumonia. See Figure 1 and 2 Page 6;
"Photograph of Eliza Jane Scovill's H.& E. stained lung section shows normal structures of the lung. Note that the alveolar spaces are free of exudates and the alveolar walls are free of inflammation and fibrosis." i.e. no pneumonia on microscopic examination. Take a look for yourself.
Adele has claimed that death from AIDS can occur with a normal white count. This paradoxical statement is no different from many other paradoxes of AIDs Mythology, so why not accept it as well? AIDS requires no logic. It works better if one suspends all logic.
The Ribe LA autopsy report was a political response rather than one grounded on good science. There is a huge amount of money and reputations at stake in the politics of HIV. Why else would the tragic death of a little girl be turned into a political football? Andy has revealed only a few of the many glaring inconsistencies and "problems" with HIV medical science. Its time to re-evaluate the huge amount of NIH dollars wasted on this 20 year project which has gone nowhere. Taxpayers of a democracy have a right and obligation to decide where the money goes. Its time to turn off the money.
I take it none of the HIV deniers are HIV+.
The equation HIV + No HAART = death is pretty reliable.
We're seeing one now. The guy knows full well what HIV and AIDS are. He just isn't facing the fact that he is probably infected and progressing.
Keeps showing up at the ER with opportunistic infections.
Losing weight. Doesn't look healthy.
Also seems to be coming down with neurological symptoms, not quite AIDS dementia but confused.
Best guess. He will be dead in 6 months to 2 years. This is a bad way to go.
With HAART he could recover, the confusion and infections would subside and he could live another 20 years. The few who are tying reality into pretzels don't have much at stake. In the real world, the stakes are much higher. In this case 2 years or 20.
Andrew, defender, another guy,
You note Ribe's actions a decade ago, launching ad hominem attacks on him, the entire coroner's and medical examiner's offices, but you associate with al-Bayati, who never examined EJ's body, and who has no training or accreditation for writing pathology reports, and claims that shaken baby syndrome is a vaccine side effect? Regardless, Ribe did not perform the p24 staining, Maurice Verity MD did, so your attacks on him miss the mark.
Without evidence for a coverup (outside of not agreeing with your discredited hypotheses), claims of a political attack are just more conspiracy mongering. The political attack comes from the denialist side, and from Maggiore's own employee.
As a report, al-Bayati's writing is weak reasoning, and as Orac has pointed out, more about producing doubt for the layperson on the cause of death than actually establishing a cause of death that would convince someone with a background in medical science. His report admits that Pneumocystis carinii was found in EJ's lungs, but dismisses the foamy infiltrates and presence of large amounts of fluid, and ignores references to consolidation in the coroner's report. He also seems ignorant that PCP often does not involve as much inflammation as other forms of pneumonia. Orac points out a wide variety of weaknesses in al-Bayati's analysis, and I recommend reading it.
defender wrote:
The rebuttal to Al Bayati by Bennet is questionable for a number of reasons. One, Bennet is am AIDs apologist and heavily involved in the politics of AIDS and hardly an impartial observer. Bennet's credibility has been impugned on previous exchanges on various blogs and, quite frankly, he is not to be trusted.
AIDS apologist? You mean someone who writes from an evidence based perspective? Bennet's bias is for evidence and reality, which are the bane of denialists of all shades, whether they deny evolution, climate change, germ theory of disease, or that HIV causes AIDS.
Two, Bennet himself questions why neither a serum HIV serology report nor a HIV viral load report was included by Ribe in the autopy report. Both are elementary and standard tests for making the diagnosis of HIV, and both conspicuously absent suggesting strongly that the tests were done and results withheld because they were negative. Instead the coroner relied on P24 protein stains on the brain tissue which are not commonly used for diagnosis of HIV in the population of North America.
Bennet points this out, yes, there were no serology reports, and that they would have been useful, but the heavy staining for p24 in EJ's brain is diagnostic. The use of controls was dishonestly omitted by al-Bayati in his report. The statement that stains of brain tissue are not used for diagnosis in N.America is fairly humorous. Blood is much more easily obtained from the living than is brain matter. However, the presence of p24 in the brain, combined with the presence of multinucleate giant cells, to anyone but denialists, is proof positive.
In fact P24 is NOT a protein entirely unique to HIV, and the P24 test is prone to "false-positive" reactions.
p24 false positives can be elicited in a variety of tissues. This is why you use controls to eliminate such problems, as was done by Dr. Verity. p24 is unique to the HIV capsid. I'll pull the papers tomorrow but would not be surprised to find the typical pseudoscience penchant for deliberate misinterpretation of evidence.
Andrew,
Risk factors are predictive of trends within a population, but no matter how uncommon something is in a population, if it happens to you, it ceases to be rare. A lack of understanding of statistics and epidemiology should be an indication that the HIV/AIDS denialists are pushing baloney.
Pediatric AIDS deaths with high total T cell counts are uncommon, but not unheard of. Amoxacillin reactions that take place two days after exposure are unheard of.
My first exposure to Medical Hypotheses was when it was cited by germ theory denialists, and I was thoroughly underwhelmed. I would be embarrassed to send a paper there.
Robster,
You presumably didn't notice that "Andy's defender" and "just another guy" have submitted 2 virtually identical posts, and are presumably the same person. Perhaps there is a prosaic explanation, but from past experience I find it typical for denialists to try and create the appearance that there are always more of them than there actually are. Some kind of perverse argumentum ad populum fallacy, I guess.
Mind you, I wouldn't be surprised if they were both Andrew's sock puppets.
To all!
Joke: Why did the drug resistant TB lawyer who has "drug resistant TB" and who has been in the news as being the one to irresponsibly infect 5 continents "RUN" a mile before he went to the hospital?
Answer(s): He's an ambulance chaser?
He wanted to be in the care of the best nurses?
He forgot to read how Koch's greatest contribution was to isolate TB on solid cultures more than 100 years ago (a lot of time for resistant TB to suddenly come up as the new Bush Budget is being supported by Fauci in front of Congressional committees-don't you think?) and define for the first time that in the case of TB, as with other microbes, like gives rise to like (only possible because of the solid medium he first discoved, unlike liquid cultures used by Pasteur, can demonstrate colonies of like organisms spreading radially from a single or small number of organisms that can be identified as such). At least in the case of TB (certainly not with many fungal microbes that can switch morphologies such as syphilis and other microbes under both culture and in vivo conditions) one can associate the rods one sees in solid cultures, with clinical disease, but still, the most important part is missing-why don't most people who acquire it get sick?
He is a healthy carrier?
I think this is a crux of much confusion, "the healthy carrier state," and as Tara points out, includes all pathogenic microbes, and their association, (if any) to disease states.
To Adele,
RE:
"They died of "toxic antiretrovirals" you say."
I didn't say that. I asked if anyone knew if those children in the studies I did read and that you say support the association of high T-cell counts and death from "HIV-caused" OI's were given any drugs in the PICU or elsewhere (such as corticosteroids,antibiotics, anti-virals, etc.,) that could and probably would have been given, and which all cause significant morbidity in small numbers of children (that match or nearly match the reported death rates mistaken for AIDS deaths) regardless of the T-cell counts?
RE:
"Even though retrovirals have reduced transmission and then mortality until pediatric AIDS in this country is alsmot gone!"
"In this country" is the thing you say that I must doubt and am worried about.
For instance,in The Journal, AIDS, for instance, it was published that Italian children born to ZDV-treated mothers "are more likely to have a rapid course of HIV-1 infection compared with children born to untreated mothers, as disease progression and immunological deterioration are significantly more rapid and the risk of death is actually increased during the first 3 years of life" [de Martino et al., Rapid disease progression in HIV-1 perinatally infected children born to mothers receiving zidovudine monotherapy during pregnancy. AIDS. 13 (8):927-933, May 28, 1999].
And certainly, not in Africa.
Virological failure or drug resistance are technical terms among "HIV=AIDS" proponents that simply means a drug doesn't work (fails to suppress virus-ignoring the fact of course that no drugs work against AIDS since it is 100% fatal and nobody wants to look at thousands of LTNP who never take drugs), or that disease progression is more rapid in those that take a particular drug, as it was reported a few months ago by none other than the infamous Max Essex group. In the New England Journal of Medicine, it was reported (and despite its known toxicity and withdrawal from the U.S. several years ago and despite the fudging of data by Tremont and the dismissal of the safety officer, Johnathan Fishbein who blew the whistle on Tremont fudging the nevirapine data):
"Nevirapine remains central to the prevention of mother-to-child transmission of human immunodeficiency virus type 1 (HIV-1) and to combination antiretroviral treatment throughout much of the developing world... Well over 875,000 women and infants have received a single dose of nevirapine. A single dose of nevirapine is the cornerstone of the regimen recommended by the World Health Organization (WHO) to prevent mother-to-child transmission among women without access to antiretroviral treatment and among those not meeting treatment criteria. However, nevirapine resistance is detected (with the use of standard genotyping techniques) in 20 to 69% of women and 33 to 87% of infants after exposure to a single, peripartum dose of nevirapine. Among 60 women starting antiretroviral treatment within 6 months after receiving placebo or a single dose of nevirapine, no women in the placebo group and 41.7% in the nevirapine group had virologic failure (P<0.001). Women who had received a single dose of nevirapine had significantly higher rates of virologic failure on subsequent nevirapine-based antiretroviral treatment than did women who had received placebo. This apparently deleterious effect of a single dose of nevirapine was concentrated in women who initiated antiretroviral treatment within 6 months after receiving a single dose of nevirapine. We did not find that a previous single dose of nevirapine compromised the efficacy of subsequent nevirapine-based antiretroviral treatment in women who started antiretroviral treatment 6 months or more after delivery. Among the 30 HIV-infected infants, a single dose of nevirapine (one each to mother and infant) as compared with placebo was associated with significantly higher rates of virologic failure and smaller CD4+percentage increases in response to subsequent nevirapine-based antiretroviral treatment"[Lockman S. et al., Response to Antiretroviral Therapy after a Single, Peripartum Dose of Nevirapine. The New England Journal of Medicine 356 january 11, 2007].
Woops! Someone ought to at least say to those 41.7% of those 875,000 African mother -infant pairs treated before 6 months that, "oh well, bad shit sometimes happens in forced drug studies designed to dump toxic drugs banned in the US on Black people," don't ya think?
RE:
Their mothers were all drug addicts, you say, even though children of drug addicts don't get these diseases in these numbers unless their HIV positive too."
I never said that. But it is true if you look at the lit, that "AIDS" did morph to "a plague" that is caused by a microbe that is like "getting hit by a truck-you don't need co-factors," according to Gallo as he ran away from countless interviews wearing his dark glasses, to pretty much widespread acceptance, even by "HIV=AIDS" proponents (excluding that denialist Montagnier of course), that co-factors such as profound drug addition are always part of the picture. I didn't say this though and I don't even think it is required to account for the so-called "HIV/AIDS" in the US or anywhere else. All one need do, is look at the disclaimers on all of the "HIV" test kits to know that the markers don't mean a goddamn thing-as in the case of Christine, and her 6 consecutive, non-agreeing "HIV" tests showed, before they branded her daughter an "AIDS" case.
RE:
"Then you give us this strange Mullis thing. Mullis didn't invent quantitative real-time PCR did he or did I miss it?"
I think he had something to do with it. Maybe they gave him the Nobel for his ability to surf and do drugs?
RE:
"And so what if he did?"
Then, Adele, I would suggest that at least you listen to what he has to say about his own Nobel-winning contribution, before trusting "Men Of The Year" like David Ho, who have, despite numerous warnings by those of us who do use PCR (check out some of my published work-I do use it too), that his viral load religion is a viral load of crap!
RE:
"Does His Royal LSDness's opinion make PCR complete crap like you say over the evidence from probably ten thousand technicians around the world?"
All I can say here is that you are giving those 10,ooo lab techs a bad name. I was a lab tech for 5 years. I always thought they were the backbone of any lab. Please don't malign lab technicians, please! In this regard, have you tripped with Karry? Do you know he uses LSD before spreading this kind of information?
Look Adele, there is a lot of pressure these days with Nobelists, you know. D. Carlton Gajducek, the Nobelist who claimed to discover prions in connection with Kuru plead guilty to multiple counts of child pedophilia, and was convicted (serving only of course a year's suspended sentence in Europe of course). It was his "brilliant science, for instance, that established the prion hypothesis (ya don't need nucleic acids for inheritance despite the fact that Pruisner's mice had diseases whether or not they had any "prions" present), and of course, he ruined the hamburger business in England, and elsewhere. I'd rather stick to LSD, as I don't like self-admitted and convicted child sexual abusers to tell me about slow viruses for those (like Gallo) that rescued the "slow virus hypothesis" for cancer that again failed after Gallo's HTLV-1 and HTLV-II booboos, and of course that still supports the mistaken use of the slow virus hypothesis for cancer (eg. HPV, Hep B, HTLV-1, etc). There ain't of course no slow viruses, as Peter has said, only slow virologists.
RE:
"Have you done a real-time PCR before, Andrew?"
Yep.
RE:
"I have a bunch. Know what? It works."
Yep. It does.
"Have you done a reverse transcriptase assay, Andrew? I have. It works. Yeah, there are cellular RTs, but guess what? They don't mess up your RT!"
Adele, read other Laureates like Varmus and Temin. Also check out the lit on market shares regarding probes that detect RT in just about every critter the God or the Great Designer designed.
Thanks for your info. So I can now safely tell my students that AIDS is a disease of too many lymphocytes, not to few.
I still think radiating these children should be considered to get their T-cell counts down. It really works better than AZT, nevirapine, and protease inhibitors (eg):
Estaquier, et al., reported in an article entitled, "Effects of Antiretroviral Drugs on Human Immunodeficiency Virus Type 1-Induced CD4+ T-Cell Death" (Journal of Virology, Vol. 76, No. 12, p. 5966-5973, June 2002) that:
"We treated PBMC from HIV-seronegative healthy donors with increasing concentrations of IDV, SQV, or ddI for 3 days and monitored T-cell proliferation and cell death. Both IDV and SQV decreased T-cell proliferation mediated by CD3 MAb in three independent experiments performed with healthy donor cells with a mean decrease for SQV of 53% ± 15% and a mean decrease for IDV of 48% ± 12% (Fig. 4A). Moreover, in the absence of T-cell activation, we observed that 10 µM IDV and SQV induced a loss in membrane mitochondrial potential (m) as assessed by flow cytometry using DiOC6."
Cheers,
Andy
BTW. Arguments don't necessarily refute things, even 3 of them. Experiments do. Is there a good animal model you know of whereby "HIV" can be injected, and AIDS results? Or is the best that has been achieved on this issue (and I know, SIV has always been a better model of "HIV" than "HIV" for 1,000,000,000 good reasons) still those 150 chimps that have new retirement homes?
Dr. Albert Sabin, Virologist:
"I think the views of a person like Dr. Duesberg are terribly, terribly important, and we must pay attention to them." (Oakland Tribune 31 Jan. 1988).
Dr. Heinz Ludwig Sänger, Emeritus Professor of Molecular Biology and Virology, Max-Planck-Institutes for Biochemy, München. Robert Koch Award 1978:
"Up to today there is actually no single scientifically really convincing evidence for the existence of HIV. Not even once such a retrovirus has been isolated and purified by the methods of classical virology." (Letter to Süddeutsche Zeitung 2000).
Awarded and respected AIDS scientists such as Dr. Kary Mullis, Biochemist, 1993 Nobel Prize for Chemistry, inventor of PCR used to detect "HIV" were also quoted as saying (Sunday Times, London, Nov. 28, 1993):
"If there is evidence that HIV causes AIDS, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
Andrew, we've been through the lymphocyte thing many many times. If you don't understand that total lymphocytes is not equal to CD4 counts after all the discussion here than I can't say anything more. You know what you're saying is fallacy, AIDS is NOT a "disease of too few lymphocytes" it's a disease of too few of a particular KIND of lymphocyte, and in pediatric AIDS its not even that all the time. You must know it's a fallacy. But you keep saying it to convince the people who are your real audience, the HIV positive people who don't have a PhD in biology and who you can fool into taking themselves off therapy and dying. Shame on you.
Insulting lab techs!!?? Andrew, youre just proving again you don't read any comments here. I AM a lab tech!! How many times have I said that?? I didn't insult 10,000 lab techs, I said that experience is alot better than Mullis opinion. I put lab techs ABOVE a Nobel-ist! And yes Kary Mullis did take LSD. Have you read his book? Looked at any interviews with him? It doesn't matter by itself you know but when you go around bragging about it and all the other stuff he did its good indication he's not all there.
And no Kary Mullis didn't invent quantitative real time PCR. He got a Nobel Prize for taking PCR mainstream. The people who did the concept did it back in the sixties. Mullis couldn't have done it himself without a load of colleagues who helped him. Look at the Wikipedia on Mullis if you don't believe me its documented.
But who cares? All I'm saying is a Nobel Prize doesn't make you god. If Mullis really thinks HIV can't be measured by RTPCR, who cares? I did a viral load RT-PCR last week. The infected cells had high copies. The cells that got a mutant virus had some copies but a lot lower. The cells with defective virus, no detectable virus. No virus, same thing. Me and my ten thousand fellow techs confirm Mullis was wrong on this every week. Full experiments, good controls. Oh, and RT? I did an RT on those samples too. Gues which ones had a significant reading? Only the infected ones! If your'e right, I should have got readings on the cells without virus. I didn't.
So there's your experiments, Andrew. Not that you'll accept them. And since you're so into misrepresenting everything I say, I repeat, I don't think you're a colleague or a conscientous scientist. You're a very bad logician and debater. I'll be following the good example of my senior colleagues so if I write anything more on this thread it will not be addressed to you. I'm sorry if its rude but Ive lost all respect for you and your misused intellect.
You want a forum for your wacko snake oil stuff? Go to late-night AM like I said. I'm not going to facilitate you anymore by responding to lies.
Andrew, your wilful misconceptions and misrepresentations might just consume this entire blog if you are not careful. I haven't got the time to go into refuting all of your various idiocies.
But this one caught my eye.....
Can I ask you truthfully if you have any concept of what this means? Have you deliberately glossed over the fact that the authors are talking about kids who are HIV infected despite their mothers taking prophylaxis, and this group is a rare and vanishing entity?
I'll simplify. Take 100 pregnant moms with HIV. With no drug intervention to reduce mother to child transmission, around 20 will deliver an HIV positive child, which will probably get AIDS and may die from HIV. (Result:- 20 AIDS/death, 80 kids alive and well).
Now take 100 pregnant moms with HIV. With drug intervention, maybe one (repeat, only one) will have an HIV positive child. (Result:- 1% will get AIDS/die, 99 kids alive and well) This Italian study suggests that there is a statistically increased risk for this single HIV-infected child for progressing faster to AIDS than the 20 HIV infected kids in the first group. (and there are reasons for this, including drug resistance, so this is potentially correctible).
Now no-one but an imbecile would imply that of the 2 groups of mothers they would chose to be in they would opt for the first. Yet you trumpet this study as though it spells the death knell for drug intervention in pregnancy. Now either you yourself believe this (in which case you are stupid and cannot fathom the implications of this paper), or you actually do know what it means (but wish to deliberately decieve others).
Since you are not stupid, I assume it must be the latter. Please correct me if I am wrong and if it is indeed the former.
DT, I did notice the similarity, but decided to let it go.
Andrew, with all the logical fallacies (non sequitor, repeated appeals to authority) and above noted misinterpretations of data (and Mullis's drug use), your above response was useless.
I will respond to one item, as it is the crux of denialist claims, and accompanied by a blatant appeal to authority.
Awarded and respected AIDS scientists such as Dr. Kary Mullis, Biochemist, 1993 Nobel Prize for Chemistry, inventor of PCR used to detect "HIV" were also quoted as saying (Sunday Times, London, Nov. 28, 1993):
"If there is evidence that HIV causes AIDS, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
Despite being a 14 year old quote, it is repeated constantly throughout the denialist camp. It is also completely false. The innumerable "scientific documents," also known as research and review articles, have long ago demonstrated that HIV causes AIDS. The denialists lie about this, moving the goalposts and ignoring every month's addition to this knowledge.
In fact, this quote could be reworked in a variety of ways, without changing its scientific impact.
"If there is evidence that Darwinian evolution contributes to the diversity of life, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
or
"If there is evidence that human activity contributes to climate change, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
or
"If there is evidence that the germ theory of disease is correct, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
or (don't laugh, an HIV/AIDS denialist argued on this very blog that gravity is fake)
"If there is evidence that Newtonian concept of gravity, and all gravitational theories based on it are correct, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document."
Some even claim that every setback for the denialists is a victory. Their worst abuse comes when an AIDS patient who had been convinced to stop treatment dies from AIDS related OIs, the denialists refuse to acknowledge their connection to the person, or claim that the patient had begun abusing drugs, leading to their death. In EJ's case, the untreated patient, infected by her mother (an apparently healthy carrier), her death was attributed by al-Bayati to an epically improbable linkage of parvovirus B19 and an amoxacillin reaction unlike any reaction seen before.
Robster has essentially admitted with the above rant that there no scientific publications exist which prove that HIV is the cause of AIDS, and offers a number of illogical and weak excuses for suspending the normal rules of infectious disease for the "special case" of HIV which consumes 8 Billion a year of NIH research money paid out to the "HIV believers".
Next, Robster like most of his colleagues, will probably prove his point by showing us a Government web site that says "all scientists believe that HIV causes AIDS". You don't have to be a Nobelist to understand what this means.
In 1983 nobody thought that HIV causes AIDS. In 1985, everybody believed that HIV causes AIDS. Where are the medical publications in the intervening 2 years which prove this? Lets not have lame excuses please.
Raven said:
"I take it none of the HIV deniers are HIV+. The equation HIV + No HAART = death is pretty reliable. We're seeing one now. The guy knows full well what HIV and AIDS are. He just isn't facing the fact that he is probably infected and progressing. Keeps showing up at the ER with opportunistic infections. Losing weight. Doesn't look healthy. Also seems to be coming down with neurological symptoms, not quite AIDS dementia but confused. Best guess. He will be dead in 6 months to 2 years. This is a bad way to go. With HAART he could recover, the confusion and infections would subside and he could live another 20 years. The few who are tying reality into pretzels don't have much at stake. In the real world, the stakes are much higher. In this case 2 years or 20."
Thank you for this anecdote from the ER. Perhaps you would like to share with the readers the complete medical chart on this gentleman including chem panel, liver enzymes, cbc, HIV antibody, nutritional status, etc. For example, is this ER gentleman a malnourished, homeless drug addict who is also psychotic? If so, it defies any form of logic to expect a toxic drug to provide any health benefit to a homeless psychotic drug addict, HIV positive or HIV Negative. I would advise you to provide him a roof over his head, three hot meals a day and wean him off the street drugs and other illicit activities as a more rational approach to health care for him. Or perhaps you have a double blind medical study which shows that toxic drugs given to drug addict street people prolongs their lives. I doubt it.
How about the well nourished HIV positive military recruits who are picked up on routine screening? Are they predestined to die an ugly death in 6 months ? I think not. How about the estimated 1 million Americans who are HIV positive and don't know it? Are they predestined to die an ugly death? I think not. They are walking around perfectly healthy like many other HIV positives who never take toxic drugs and are living normal lives for 15-20 years after HIV diagnosis.
Taxpayers are sick and tired of wasting money on a failed NIH research program on HIV that has wasted 100 Billion Dollars. Put the money to better use elsewhere.
Classic denial, "another guy" confuses HIV and AIDS.
Raven: gives an advanced AIDS case, OIs, multiple symptoms, says he'll die in months or a few years.
AG: wonders why all HIV positive people don't die in six months.
Me: shaking my head. How do they keep up this ignorance level?
To Adele,
Sorry for my questions. I won't bother you anymore. Thanks, though for all of the info.
Robster: RE:
"Can I ask you truthfully if you have any concept of what this means? Have you deliberately glossed over the fact that the authors are talking about kids who are HIV infected despite their mothers taking prophylaxis, and this group is a rare and vanishing entity?"
Wait a minute! Kids were infected DESPITE prophylaxis? I thought that "the life saving meds" were promoting lifespan now for 24 years (for a disease discovered 25 years ago!!!!
In a article published in Science, David Ho, Daniel Douck, and
Ronald Desrosiers were quoted as saying that the "HIV=AIDS" time course
should be shortened to span several months to a few years (Jon Cohn. "It's
The Gut, Stupid." 4 March Vol 307, p. 1395, 2005), and that "HIV" kills
the lymphoid tissues of the gut in a few days to months.
This proclamation was at variance with the CDC's long-standing contention
that "HIV" has an average latency of 5-10 years before progression to
AIDS.
A recent proclamation from Dr. Bruce R. Schackman, Chief of Health
Policy at Weill Cornell Medical College in New York (that beacon of AIDS
science) and lead author of a paper appearing in Medical Care, a journal
published by the American Public Health Association says that "HIV/AIDS"
patients can live an average 24 years, if they pay $385,000.
Can anyone appreciate what good news this really is for a disease that is
25 years old (or 22 years old once that "HIV," "a variant of a known
cancer virus" was found to be "the cause")? It means that, for 385,000
dollars, you can actually live longer with a disease (on average), than
the period of time that that disease is said to actually have been killing off our
species. If you do the math (unless I can't subtract very good-I could
use some help here folks), on average, there are people probably living
for 50 years who have a disease that is at most only 25 years old (1981-2
was when David Gottlieb first described it).
The logic of these proclamations is stunning in the context of the AIDS
ABC's (www.reviewingaids.org/awiki/index.php/Document:ManiotisABC):
A ("HIV") leads to B (decrease and inversion of CD4/CD8) which leads to
C (full blown AIDS):
CDC says:
A ("HIV infection") leads to B (drop and inversion of CD4/CD8 in 5-10 years), which leads to C (inevitable full blown AIDS/DEATH).
David Ho, Daniel Douck, and Ronald Desrosiers says:
A ("HIV infection") leads to B (drop and inversion of CD4/CD8 in a few months), which leads to C (inevitable full blown AIDS/DEATH).
Bruce R. Schackman says:
A ("HIV infection") leads to B (drop and inversion of CD4/CD8) which leads to
C (inevitable full blown AIDS/DEATH in 24 years on average).
The news don't get much better than this. Please pass this good news along....
However, there is a catch. Robster (I love your name and hope your students never learn about your extracurricular AIDS activities), maybe you are talking about them damn mutants! Like TAG's Harrinton once said about the power of prayer and the Chinese menu approach in the context of faith-based science and medicine currently dominating discussions regarding the "mutability" of the "HIV" virus, and the failure of ARV-therapy. Individuals who fail ARV therapy are told their virus has mutated and is no longer sensitive to the drugs. The impact of this hypothesis on persons living with "HIV" or "AIDS" is unfair, uninformed, and cruel. For example, Mark Harrington, a member of The Treatment Action Group (TAG) summoned "the power of prayer" over "HIV" mutability, and discussed "The Chinese Menu Approach" in a description of a meeting he attended on developments regarding anti-retrovirals that included AIDS leaders such as Marc Wainberg, Director, McGill AIDS Centre, and this summer's Chair of The Toronto International AIDS Conference-who possesses several "HIV" drug patents such as lamivudine (3TC), and grants from GlaxoSmithKlein, Bristol-Myers Squibb and Boehringer-Ingelheim. Also present at the meeting was Emilio Emini, Tufts University's John Coffin, Roche's Noel Roberts, the CDC's Harold Jaffe, Chiron's David Chernoff, the ACTG's Robert ("Chip") Schooley and John Mellors (developer and champion of the viral load tests now known to be invalid), as well as treatment activist Dawn Averitt-Doherty of Atlanta-based Woman's Information Service and Exchange (WISE):
"During the coffee break, I (Harrington) joined three activists outside to share nicotine and despair. What was the point of quitting smoking if we were still all passengers on the speeding train heading for the cliff? The Birmingham resistance data were wrenching. Our fears of multiple cross-resistance, from November 1995's 3TC and saquinavir FDA approval hearings, reared their ugly heads. Several months of post-Vancouver euphoria crumbled in a moment as it became clear that many of those who developed resistance to ritonavir and indirovine-as thousands clearly would-might have no protease inhibiting options ahead of them. Today's resistance news made for a toxic cocktail. As I left the auditorium I bumped into Emilio Emini."
"Harrington: So what do you do if you fail Crixivan?"
"Emini: [sighs] We don't know what to do."
"Harrington: Take two new nucleosides and nevirapine?"
"Emini: Yeah. And pray."
"No one had yet assessed the healing effects of prayer on viral load. This was what we'd come to. I rushed into the lobby of the Interior Department and ran into a colleague, who was wild with fear and disappointment."
"Sometimes the gap between how the researchers felt and how we felt became an abyss. They were excited about the endless possibilities opened up by the research advances of 1996; we were terrified about the limited treatment options facing people who had exhausted most of the current arsenal of antiretroviral therapy. What to do with those whose viral load refused to go undetectable? What to do with those who added a protease inhibitor to a failing two-drug regimen and appeared doomed to develop resistance, most of it-especially with ritonavir and indinovir-cross-resistant to all other protease inhibitors? What to do with those who jumped aboard last year's bandwagon, AZT+3TC, and now appeared likely to have developed 3TC resistance and, with it, cross-resistance to ddI, ddC and possibly 1592? The Chinese menu approach to antiretroviral treatment suddenly looked much less appetizing, and much less nourishing"[42].
These same results also have been advanced in frequent warnings on MedWatch:" Early virologic nonresponse (91%) and nucleoside reverse transcriptase inhibitor (NRTI) resistance (50-95%) has been observed at a high rate in a Gilead Sciences-sponsored clinical study. Participants in the study were treatment-naive (ie, no previous treatment for HIV) took a once-daily, 3-drug NRTI regimen. The NRTI regimen contained didanosine enteric coated beadlets (Videx EC), lamivudine (Epivir), and tenofovir (Viread)" [1].
"The new information is consistent with several recent clinical studies evaluating the use of 3 NRTIs simultaneously. Suboptimal virology response has also been reported with abacavir, didanosine, and stavudine, as well as another regimen containing abacavir, didanosine, and zidovudine. Similarly, early virologic failure and high resistance rates have been reported with abacavir, lamivudine, and tenofovir (see eMedicine Recalls and Alerts 8/1/03, Nonresponse Reported in HIV Infection Treated with 3-Drug Regimen Including Lamivudine, Abacavir, and Tenofovir"[1].
Other warnings on FDAMedWatch support Mr. Harrington's sentiments regarding liver toxicity, and also warn about neural tube defects in fetuses from woman who test positive and who are treated with "the life saving" AIDS medicines:
"Increased Liver Toxicity with Nevirapine (Viramune) and Higher CD4 Counts...Revised prescribing information for nevirapine (Viramune) includes a new recommendation against starting nevirapine treatment in women with CD4 cell counts above 250 cells/mL and males with CD4 counts above 400 cells/mL unless benefits clearly outweigh risks. The new recommendation is based on an increased risk of serious liver toxicity with higher CD4 cell counts prior to starting therapy with nevirapine"[2].
"Females and patients with higher CD4 cell counts are at increased risk of liver toxicity. Females have a three-fold higher risk of symptomatic nevirapine liver toxicity than males, and females with CD4 cell counts above 250 cells/mL have a 12-fold higher risk of symptomatic liver toxicity than females with CD4 cell counts below 250 (11% vs. 0.9%). Males with CD4 cell counts above 400 cells/mL have a five-fold higher risk of symptomatic liver toxicity than males with CD4 cell counts below 400 (6.3% vs. 1.2%)"[2].
"New Drug Interaction Warning with Rifampin and Combination of Ritonavir and Saquinavir. 'Drug-induced liver toxicity with highly elevated liver enzymes (greater than 20 times the upper limit of normal) has been observed in 39% of healthy volunteers receiving rifampin 600 mg once daily in combination with ritonavir 100 mg/saquinavir 1000 mg twice daily (ritonavir boosted saquinavir) [3].
Neural Tube Defects with First Trimester Efavirenz (Sustiva) Use.""The prescribing information for efavirenz (Sustiva) has been changed to include new information. The revision result of four reports linking neural tube defects in infants born to women with first trimester exposure to efavirenz. The four cases of neural tube defects include three cases of meningomyelocele and one Dandy Walker Syndrome. Pregnancy should be avoided in women receiving efavirenz...Efavirenz is an antiretroviral drug indicated for acquired immune deficiency syndrome (AIDS, HIV-1 infection). A registry has been established to monitor fetal outcomes born to women exposed to efavirenz.." [3].
Cheers,
Sorry forgot the refs.
[1] FDAMedWatch 1/19/2005.
[2] FDAMedWatch 2/9/2005.
[3] FDAMedWatch 6/10/2005.
Looks like whack-a-mole with "Gene Semon", the sequel. Ocean's Nineteen. I always wondered where "Nick" got his vocab.
"another guy,"
No, and that's the problem. It's the deniers who want to make HIV/AIDS a special case. I've discussed this extensively before, so let me cut and paste something I've written previously:
For the lurkers, the request Maniotis makes of literature is a slick trick. As Robster points out, it can be applied to any area of study, because it's never a single paper that makes the case, especially in the field of disease causation. You supply the deniers with, say, a dozen relevant papers that make a strong case for causation, and they'll push back the goalposts--"well, these papers didn't show X and Y, so we're still waiting for the evidence." Meanwhile, thousands of additional papers did indeed show X, Y, and Z to boot, but of course, we're always lacking a total picture (otherwise, we could all quit our jobs as researchers!) So they'll always ask for more, because anyone can see that the picture is never totally complete.
It's nothing but a rhetorical gimmick, but it's one you see crop up over and over among science deniers.
Tara,
You're absolutely and brilliantly right on moving the goalposts.
Sometimes Maniotis is so lazy he doesn't even do that. He just moons the spectators and yells out a funny joke for his two fans in the peanut gallery. Like "there ain't no slow viruses, only slow virologists" Or "Kids were infected DESPITE prophylaxis? I thought that "the life saving meds" were promoting lifespan now for 24 years (for a disease discovered 25 years ago!!!!"
Meanwhile his whole team on the field ignores the score, 1.8e9 to 0.
To Adele and Raven:
Try speaking to the issue instead of useless ad hominem attacks which serve to announce the emptiness of your position.
Show us the medical study that shows that giving toxic drugs to this hypothetical ER HIV+ patient with opportunistic infections, and multiple symptoms will prolong his life.
Are you referring to the Concorde study which showed no improvement in mortality from HAART?
Where are the references from 1983 to 1985 which prove that HIV causes AIDS?
Where are the references that show that toxic drugs prolong the life of drug addict street people? Toxic drugs are designed for only one thing: to kill cellular life.
Your twisted logic that toxic drugs will somehow miraculously save the homeless drug addict is a delusion. Go peddle your toxic drugs on a different continent, like South Africa, the only government on the planet that has rejected your delusion that toxic drugs can ever possibly remove a nucleotide sequence imbedded in the human genome.
Another guy cannot be serious. I'll respond for the lurkers.
your delusion that toxic drugs can ever possibly remove a nucleotide sequence imbedded in the human genome
No one ever claimed it! "Another guy" is science illiterate or pretending to be. Antivirals don't "cure" HIV infection they keep the virus from replicating. They do it damn well. Antiretroviral drugs have reduced mother to child transmission and then pediatric AIDS like we discussed above until pediatric AIDS is almost gone in NA and Europe. Antiretrovirals have slashed AIDS deaths by two thirds everywhere their available. These are toxic drugs like aspirin is a toxic drug and antibiotics are toxic drugs and water is a toxic drug.
Don't forget Ben Gay.
Adele: "Antivirals don't "cure" HIV infection they keep the virus from replicating." Excellent point. The drugs do nothing to remove the HIV sequence from the human genome.
Yes, of course the drugs are designed to stop viral replication. And viral replication is measured by viral load of course, and please show me a reference in the scientific literature where the discredited viral load measurement has any bearing on morbidity or mortality. It has none.
The question is: what other actions do these anti-viral drug have? For the lurkers, I will answer this question. The cytotoxic drugs do not have a specific action on HIV, they have a broad mode of toxicity on the entire organism which in this case is human being. We are not talking about mild toxicity which can be accepted as a trade off. We are talking about severe life threatening toxicity.
Contrary to your further comment, to give these same toxic drugs to pregnant mothers and cause horrible adverse effects on their unborn fetus is a hideous crime which ranks up there with the holocaust. No, I am not a holocaust denier. However, I am a denier of the holocaust you advocate by giving cytotoxic drugs to pregnant mothers. This is a crime of unimaginable proportions and some day punishment will be meted out to those individuals responsible similar to the Nuremberg trial.
http://www.law.umkc.edu/faculty/projects/ftrials/nuremberg/nuremberg.htm
Oh but you say we have miraculously eliminated mother to child transmission and made pediatric AIDs cases almost vanish with the use of these miraculous drugs. I say hogwash to that incredible lie. Using these drugs on pregnant mothers is a criminal act.
Another guy/Andy's defender:
I suggest you look here and see how pediatric cases have declined from a peak of nearly 1000 cases in 1992 to only 146 in 2003. The reason? Implementation of HIV drug treatment for mothers to prevent transmission.
You are the liar and you know it.
http://www.cdc.gov/hiv/graphics/images/l262/l262-3.htm
Wait a minute! Kids were infected DESPITE prophylaxis? I thought that "the life saving meds" were promoting lifespan now for 24 years (for a disease discovered 25 years ago!!!!
Was there meant to be some logic in this statement?
Maniotis apparently believes in homeopathic doses of allergens. There is no small amount of irony in this coming from a HIV Denialist that either claims that there isn't enough HIV present to be biologically active or that HIV has never been proven to exist.
The lie I was referring to is not the decline in ESTIMATED numbers of pediatric AIDS case. It is the lie that antiretroviral drugs had anything to do with this ESTIMATED decline.
These numbers are ESTIMATED on the referenced GOVERNMENT WEB SITE because nobody knows the ACTUAL numbers.
For the sake of the Lurkers, I again repeat that the administration of toxic drugs to pregnant mothers is a hideous crime and those responsible will eventually be brought to justice.
I could show you hundreds of studies. Put HIV into the pubmed.com (National LIbrary of Medicine) search engine and one gets 211470 papers. One is below. Someone diagnosed with HIV and not treated dies within about 4 years average. Treated live an average of 24 years.
1: Med Care. 2006 Nov;44(11):990-7.
The lifetime cost of current human immunodeficiency virus care in the United States.
Schackman BR, Gebo KA, Walensky RP, Losina E, Muccio T, Sax PE, Weinstein MC, Seage GR, Moore RD, Freedberg KA.
Department of Public Health, Weill Medical College of Cornell University, New York, New York 10021, USA. brs2006@med.cornell.edu
OBJECTIVE: We sought to project the lifetime cost of medical care for human immunodefiency virus (HIV)-infected adults using current antiretroviral therapy (ART) standards. METHODS: Medical visits and hospitalizations for any reason were from the HIV Research Network, a consortium of high-volume HIV primary care sites. HIV treatment drug regimen efficacies were from clinical guidelines and published sources; data on other drugs used were not available. In a computer simulation model, we projected HIV medical care costs in 2004 U.S. dollars. RESULTS:
********************************
From the time of entering HIV care, per person projected life expectancy is 24.2 years,
**********************************
discounted lifetime cost is Dollars 385,200, and undiscounted cost is Dollars 618,900 for adults who initiate ART with CD4 cell count < 350/microL. Seventy-three percent of the cost is antiretroviral medications, 13% inpatient care, 9% outpatient care, and 5% other HIV-related medications and laboratory costs. For patients who initiate ART with CD4 cell count < 200/microL, projected life expectancy is 22.5 years, discounted lifetime cost is Dollars 354,100 and undiscounted cost is Dollars 567,000. Results are sensitive to drug manufacturers' discounts, ART efficacy, and use of enfuvirtide for salvage. If costs are discounted to the time of infection, the discounted lifetime cost is Dollars 303,100. CONCLUSIONS: Effective ART regimens have substantially improved survival and have increased the lifetime cost of HIV-related medical care in the U.S.
You clearly have no medical knowledge whatsoever. No one claims that HAART will "remove a nucleotide sequence imbedded (sic) in the human genome". HAART reduces HIV viral load and keeps the immune system from failing as fast. For this patient the choice is 2 years or 20 years most likely. The longer he waits, the poorer the prognosis.
"CONCLUSIONS: The recent declines in morbidity and mortality due to AIDS are attributable to the use of more intensive antiretroviral therapies."
Antiretroviral drugs are one of the major success stories of modern medicine. I've copied two abstracts. I could have copied hundreds more. Why bother? If two don't get the point across, several hundred won't either.
One more for the road. In Alberta, HAART dropped the AIDS mortality by 80% in HIV+. So much so that many patients died of other causes.
I'll save Maniotis the effort.
Raven, all of those studies you cited are meaningless because the allopathic authors have to claim success or else they wouldn't get their pharmainc funding.
The Pallella Delany paper from NEJM 1998 was not a report of a clinical trial but was a retrospective survey which is of questionable credibility. Why not use a clinical trial to show that HAART extends or improves quality of life. Where is the clinical trial?
The Concorde study showed NO mortality benefit from HAART which is the REAL STORY of what happens when a toxic drug is given to sick people, they die from the toxic drug.
The only value of HIV drugs is as a money maker for the manufacturer. These drugs don't save lives, they kill them. That's what they were designed for and they do their job with precision. Iatrogenocide was a term coined in the 1980's. The true meaning of this word was realized by the later invention of HIV drugs.
another guy/defender,
Robster has essentially admitted with the above rant that there no scientific publications exist which prove that HIV is the cause of AIDS, and offers a number of illogical and weak excuses for suspending the normal rules of infectious disease for the "special case" of HIV which consumes 8 Billion a year of NIH research money paid out to the "HIV believers".
Reading comprehension. Try it. Also, no "normal rules of infectious disease" are "suspended." This is yet another lie from the denialists, and is an argument from incredulity/ ignorance.
One of the real reasons for HIV/AIDS denialism comes out in ag's screed. The denialists want in on the research money, even though they have no results to support their requests. When the behavior hypothesis was found to be post hoc, ergo propter hoc error (behavior is often linked, but not a cause), certain groups refused to update their research and understandably, were left behind.
They repeatedly point to a lack of a vaccine, while ignoring the difficulties in vaccine development. From the initial description of Poliomyelitus in 1840 (Andrew: Polio existed before this year), to the isolation of the poliovirus in 1908, the development of the first workable Polio vaccine wasn't produced for mass use until 1955.
The no vaccine tack is also a non sequitor, as many viruses don't have preventative vaccines. There is no hepatitis C vaccine, but this doesn't mean that the virus doesn't exist, or that the work on a vaccine has been a waste.
Next, Robster like most of his colleagues, will probably prove his point by showing us a Government web site that says "all scientists believe that HIV causes AIDS". You don't have to be a Nobelist to understand what this means.
This is a strawman argument, obviously some scientists don't agree with evidence based medicine, evolution, germ theory, etc. Contrarianism does not equal truth. Evidence does.
The website I would suggest to start looking at the scientific papers, as Raven suggested, is pubmed. Happy reading.
If so, it defies any form of logic to expect a toxic drug to provide any health benefit to a homeless psychotic drug addict, HIV positive or HIV Negative.
You obviously have no knowledge of toxicology. All things are toxic depending on the dose. Name a drug or chemical, and I can probably list a toxic effect based on dose. The side effects of some drugs overlap with the therapeutic window, but the facts are clear. HAART extends the lives of AIDS patients. Calling the drugs "toxic" only demonstrates that you don't understand how medicine works. Learn something about the field before you start organizing the lynch mob.
For example, Dihydrogen Monoxide (DHMO) can be incredibly toxic. Extended exposure to DHMO in its solid form damages tissue (sometimes requiring amputation), while inhalation of even small amounts of DHMO can cause asphyxiation. Not so long ago, a woman imbibed a large amount of liquid DHMO, as part of a radio contest. It led to an imbalance of electrolytes, and the effects of intoxication directly caused her death. It has also been found in every cancerous tissue ever examined. Yet, it is completely unregulated in consumer products, is a combustion engine byproduct, has effects on global climate, and can be found in common tap water! This industrial solvent and fire suppressing compound is so difficult to remove that even after careful washing of fruits and vegetables does not remove DHMO. The press has widely treated this as a non issue, and few articles are published about the deleterious health and environment effects of DHMO, pointing to a massive conspiracy.
Put it that way, and water sounds like a horrific chemical, rather than the most precious molecule on earth.
Andrew,
Wait a minute! Kids were infected DESPITE prophylaxis? I thought that "the life saving meds" were promoting lifespan now for 24 years (for a disease discovered 25 years ago!!!!
You are replying to the wrong person, but again, you don't understand statistics. Prophylaxis is not 100% effective, and nobody ever claimed it was. Quit being dishonest.
Also, nice cut and paste job from your barnesworld piece. You deliberately confuse the age of HIV with the date of discovery. Excellent cherry picking job you have done. You missed your calling. You should be working for tobacco companies, casting doubt on the tobacco cancer linkage!
(I love your name and hope your students never learn about your extracurricular AIDS activities)
I specifically talk about HIV/AIDS denialism in my classes, and mention the different tactics that science deniers use (consider yourself honored, I'll talk about bad stats use and ignoring evidence next time). One of my first classes is called "Baloney Detection" and is based on Sagan's writings. You would do well to read up on logical fallacies. Besides, why would I be ashamed for standing up for evidence based medicine? I just find that when discussing the evidence for evolution or other socially charged topics, some students close their minds as soon as they learn your political or religious leanings.
You really are obsessing over this, aren't you?
As to the rest of your cherry picked quotes (it would be nice if you would include links to the articles so we can see them in context), one on prayer, and the other on toxicity issues... First, prayer? So someone checked out an altie method that relies on divine intervention? That certainly doesn't invalidate the entire field of research (if it did, the denialists would have long ago disappeared).
As to the "eek, toxic" game, please, pick up a copy of Casarett and Doull's Toxicology, perhaps a good pathology text, maybe a pharmacology text to go with your badly needed stats and epidemiology books. My biggest disappointment with scientists who pick up the mantle of pseudoscience is that they do such a bad job of it (see Michael Behe). Your stats, your misquoting and misrepresenting of research, reliance on logical fallacies all suggest that you don't take your denialist hobby as seriously as you do your day job. Of course, if you did, you would have to abandon your intellectually and ethically bankrupt position. You really should stick to cancer research.
For who still believe in HAART, the failed HIV drug cocktail:
The 2006 Lancet study of 22,000 patients over the past 10 years on meds, entitled, "HIV Treatment Response and Prognosis in Europe and North America In The First Decade of HAART: A Collaborative Analysis" concluded with : "Virological Response after starting HAART improved over calendar years, but such improvement has not translated into a decrease in mortality." (see page 453)
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&cmd=Retrieve&dopt=Ab…
"The fall in death rates from AIDS when HAART was introduced came about because of a huge increase in the mid-1990s in the number of AIDS patients, including many who had no symptoms, because of a widening of the AIDS definition and because of drastic reductions in dosage of AIDS drugs such as AZT, after clear indications that these are lethal."
Belief in HAART is exactly that: a BELIEF in a failed drug cocktail.
The Concorde study showed NO mortality benefit from HAART which is the REAL STORY of what happens when a toxic drug is given to sick people, they die from the toxic drug.
Reading comprehension?
The Concorde study showed no benefit of early treatment with AZT (not HAART) compared to waiting until the onset of opportunistic infections or until CD4 counts dropped before iniating treatment.
If AZT were as toxic as you claim then it would be expected that there would have been a strong relationship between the amount of AZT taken and mortality. There wasn't.
Denialists claim that AZT kills within months ie. Kimberly Bergalis was "completely healthy" until she took AZT. The Concorde study actually refutes this claim.
I suspect that you haven't even read the studies. You just regurgitate what you read on Denialist websites.
test
Quite correct, Chris.
"another guy" is parroting (really plagiarism) from barnesworld and an alive and well press release (link isn't working in scienceblog's comment system.
He doesn't have any original thoughts.
There are hundreds of clinical trial studies of AIDS drugs. All 29 approved drugs had to go through clinical trials, phase I, II, III, FDA approval. This patient population was in advanced stages of AIDS with CD4 counts less than 100. Ritonavir still nearly doubled progression free survival.
For anyone HIV+, paying attention to quack denier websites rather than the medical literature will cost them a decade or two in lifespan. Free country, we all make choices. Strangely enough, in some community studies, about 20% of the patients choose not to start HAART or quickly drop out. They are usually counted in the "reasons why they died" categories. Whatever.
What's up with Barnesworld, anyhow? I see nothing has been posted for a month, not even under "recent" comments.
"another guy" is parroting (really plagiarism)
There is a distinct possibility that "another guy" is Hank Barnes/ D. David Steele in which case he isn't technically plagiarising. Parroting yes.
Nevertheless, his misinterpretation of the 2006 Lancet study has been corrected many times.
He does the same thing with the "Padian Study": just repeating his own personal interpretation over and over agian in the vain hope that he'll alter reality.
AG, how many foeti were spontaneously aborted how many babies born with birth defects or cancer because of antiviral "toxic drugs"? Evidence any have? You have to give more than that fallacy above, after the fact so because of it. WHy isn't there evidence? I guess because like tens of thou of docs and nurses and scientists and techs have all joined up no exceptions to suppress it?
Yeah you can go back to Duesbergs book from ten years ago or one of his reviewrants from ten years ago and find a table with studies of AZT in mice rats and other animals. Duesberg says they all used physiol. concentrations like AIDS patients got back then. And the animals had fetal deformity or death or cancer. Shows what kind of a scientist he was. Most of those studies had much higher concentrations of AZT than you ever get in human blood even if the humans take 1500/day. The worst effects at more physiol. conc. were on two cell stage embryos. In vitro. Where you can keep the concentration indefenitly at the PEAK it reaches for like five minutes in humans. So sure AG in one study AZT at a higher concentration then you keep in human blood is not good for two cell stage mouse embryos. Hard to fast fwd that into Nuremberg trials even if it does apply to humans and that's not certain.
Duesberg lied. Or he's just dumb and deluded.
LEts keep going. At the two cell stage or even weeks later no one knows they're pregnant. So why would they be taking AZT? Those AZT studies showed mice and rats aren't affected by high dose AZT later in pregnancy. Which is when a pregnant woman MIGHT have it if ever. Duesberg left that out somehow like AG leaves out a thousand studies that disprove them and every line of #1001 except for the one sentence they take out of context.
AG, do you really want to compare a two cell embryo or even a blastocyst to six million victims of the German Nazis? If you do you got more problems than denial.
If you are looking for modern day dispensers of genocide, one need look no further than South Africa, where in the early part of the decade the President and his Health Minister denied the option of drug therapy in pregnancy to stop their infants getting HIV. Around 100 000 babies were infected with HIV as a result. In SA, HIV in an infant is equivalent to a death sentence, and not just a quick one either, but a lingering painful death over months or years.
That's genocide for you.
(Fortunately, SA has now belatedly come to its senses, and many if not most pregnant moms are getting HIV drugs)
To Adele and Raven:
It has already been established from LANCET that giving HAART to your malnourished ER homeless addict can not possibly improve his health or longevity, nor have any impact on his mortality rate, contrary to your irrational belief in the "miracle of HAART" which is probably based on television advertising commercials and sensationalist newspaper pablum.
How about pediatric AIDS? What is it? It is the net effect on the developing fetus of maternal drug addiction.
Cocaine abuse during pregnancy is associated with various maternal and fetal problems. Cocaine, is a central nervous system stimulant. It has vasoconstrictive effects, significantly decreasing blood flow to the fetus, resulting in periods of decreased oxygen. Many cocaine users use other drugs, exposing the fetus to many drugs, compounding the problems. For women who use cocaine throughout pregnancy it has been proven that they are at a greater risk for premature births of their babes, and a greater chance of delivering still born babies.
Heroin easily crosses the placenta and fetal withdrawal may occur if the mother undergoes rapid withdrawal. An unborn fetus exposed to heroin has an increased rate of infection. Babies born to mothers who used heroin during pregnancy are also associated with a decrease in birth weight, and an increase in stillbirths. Babies born to mothers who have a heroin addiction must stay in the hospital to receive treatment for withdrawal symptoms which include hyperactivity, convulsions, diarrhea, fever, sleep abnormalities, and respiratory distress. Once discharged they may even experience abnormal breathing patterns during sleep, thus increasing the incidence of sudden infant death syndrome seen in these children.
The effects of maternal heroin addiction may persist in the offspring for an extended period of time, resulting in poor growth and development. They may demonstrate behavioral abnormalities, including impaired organization and perception skills, impaired motor inhibition and mental retardation.
What Adele and Raven calls pediatric AIDS, the AIDS symptoms and death in the HIV positive baby, is in fact a description of symptoms and death in the baby from maternal drug addiction.
On top of the pre-existing problems of maternal drug addiction, giving a cytotoxic drug in this scenario to the mother and unborn child is a criminal act. Those responsible for such a hideous crime will eventually be ferreted out and punished.
Your rant about how safe and benign AZT is to the blastocyst is sheer drug company baloney, reminiscent of the government studies showing radiation to be safe for mice during the era of open air nuclear testing. The planet eventually came to their senses and banned open air nuclear testing.
Dr. John W. Gofman, a pioneer in radiation research said in 1979,"In the mid-'50s--when the toxicity of low-dose radiation was still uncertain--we were testing nuclear bombs in the atmosphere and launching the Atoms for Peace Program...It should have been clear to me, even then, that both atmospheric bomb-testing and nuclear power constituted experimentation on involuntary human subjects, indeed on all forms of life."
With extraordinarily blunt self-criticism Gofman--a physicist and medical doctor--went on: "I am on record in 1957 as not being worried yet about radiation from nuclear test fallout. There is no way I can justify my failure to help sound an alarm over these activities many years sooner than I did. I feel that at least several hundred scientists trained in the biomedical aspect of atomic energy--myself definitely included--are candidates for Nuremberg-type trials for crimes against humanity through our gross negligence and irresponsibility." And, Gofman added, "Now that we know the hazard of low-dose radiation, the crime is not experimentation--it's murder."
The same message can be applied to the hideous crime of administering cytotoxic drugs to drug addicted mothers. The nation of South Africa is to be applauded for opposing this crime of poisoning pregnant South Africans with toxic drugs.
Andrew's latest pseudoname is wrong/lying again.
At physiological concentrations or even higher in the mouse, no evidence AZT harms embryos after implantation and pregnant HIV+ women wouldn't take it until a long time after that, like LATE in pregnancy. This is not drug company propaganda it's work from independent labs. There's limited info on most drugs used during pregnancy so yeah, there might be effects later in life, no one knows yet. Same for most drugs. Absolute worse case scene, kid has increased cancer risk late in life. Beats the heck out of giving her HIV at birth and her dying at three of PCP. Most mothers would agree.
AIDS in children is not from exposure to drugs, it's from exposure to HIV. The symptoms of pediatric AIDS like OIs are not the symptoms of kids exposed to crack or heroin in utero. What predicts if a child dies of AIDS? Whether she and her mother have HIV, not whether the mom was a drug addict. That's why denialists are so crazy about the Maggiore Scovill case.
Thousand of drug babies are born every year but only a handful get AIDS and those are the same babies who got HIV from their moms. Most kids of drug addicts do not have HIV and these kids never get AIDS. They do have health problems sometimes because surprise cocaine isn't healthy, but they don't get AIDS or AIDS symptoms. A majority of HIV+ moms were once or still are addicts BECAUSE that's how they got HIV, injecting drugs with tainted needles. It's coincidental not causative.
And, Andrew or whoever this person is should please use quotes when they copy stuff from internet sources.
It has already been established from LANCET that giving HAART to your malnourished ER homeless addict can not possibly improve his health or longevity, nor have any impact on his mortality rate...
I find it hard to believe that you have read and understood this study.
HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis.
The study compares people beginning HAART in 1995-96, 1997, 1998, 1999, 2000, 2001, and 2002-03. All groups in the study were taking HAART. All showed benefits.
The study simply cannot say what you claim. The absolute maximum that you could possibly say is that HAART for the group beginning treatment in 2002-03 was less effective/worse than that for the group that started treatment in 1995-96.
You can repeat your false claims about this study as much as you want, however, it will not and cannot change the possible conclusions that can be drawn from the study. The only thing that you can prove is your willingness to lie.
Adele is wrong or lying again, making false assertions with no data.
Where is the phoney drug company data that you rely on to make these balatantly false statements?
Post the references of your pediatric AIDS cases that occur in white middle class college educated medical consumers. There aren't any. All published pediatric AIDS studies use drug addict mothers who are black, minority, poor and uneducated.
This new book might provide the reader with a few more useful answers:
The Origin, Persistence, and Failings of HIV/AIDS Theory by Henry Bauer.
Henry H. Bauer is Professor Emeritus of Chemistry and Science Studies and Dean Emeritus of Arts and Sciences at the Virginia Polytechnic Institute and State University. He was born in Austria and educated in Australia. After researching electrochemistry at the Universities of Sydney, Michigan, Southampton, and Kentucky, he turned to general issues relating to scientific activity, in particular how to differentiate science from pseudoscience. He has taught both undergraduate and graduate programs in humanities and science and technology studies. Upon retirement from teaching at the end of 1999, he became Editor-in-Chief of the Journal of Scientific Exploration.
Bauer has challenged the HIV/AIDS hypothesis in several papers, based primarily on the fact that the data on HIV seroprevalence are incompatible with the notion that the HIV antibody tests are detecting a sexually transmissable virus.
In 2007, Bauer published The Origin, Persistence, and Failings of HIV/AIDS Theory, detailing his arguments against the HIV paradigm and his own explanations of how it is has persisted for so long despite its failings.
"Data have now accumulated from tens of millions of tests, the great majority on groups not thought to be at any great risk. When those results are collated and compared, they turn out to be incompatible with the widely accepted (but not unanimous) view that HIV tests detect the AIDS-causing virus that is presumed to have spread via sex and infected needles from the original centers of AIDS - New York, Los Angeles, and San Francisco." (Bauer 2005)
"In the overwhelming majority of reports, the ratio of F(HIV) [prevalence of HIV antibodies] to that among whites is: Asians, 0.5-0.9; Native Americans, 1.1-1.6; Hispanics, 1.5-3.0; and blacks, 2.5-6.0.
One has the choice of seeking for these observations a behavioral explanation or a non-behavioral one. Any behavioral explanation raises ghosts of such long discarded and properly discarded theories as phrenology, physiognomy, or Cesare Lombroso's Criminal Anthropology, which asserted a strictly determinist connection between behavior and physique (or genome). Fortunately, a less racist and more scientifically (as well as politically) correct explanation is available." (Bauer 2005)
"The orthodox rule is wrong and the paradigm is ready to be toppled." (Dellinger 2006)
Dear Tara,
What you state is inaccurate:
"Sure. Many AIDS deniers, for eample, use the aforementioned Christine Maggiore's life story as a case in point. She's tested HIV+, but as her organization notes, remains "alive and well."
She hasn't only tested positive:According to her book, she tested inconclusive, positive, inconclusive, positive, negative, and positive. If experiments run like that in my lab, I wouldn't publish them, would you? Something I learned about 3 times in a row, makes a trend, and 10 times in a row is better, etc.
Maybe she has a sensitive immune system, as her daughter apparently did, that would account for never testing the same way twice? I wouldn't advocate the state taking her beloved son away, or imprisoning her, if her "hyper-reactive" immune system may be her crime. I especially wouldn't advocate, as many of your denialist camp has, to imprision her because her daughter died 36 hours after imbibing amoxicillin, was gaining weight the last six months of her life, and had 10,800 T-cells, a coroner assigned to the case who is facing other charges for cooking at least 5 reports in the past (I could get you any slides you want to see-I just need to walk down the hall and ask any one of 50 different pathologists-to give me a slide showing PCP-if you get my drift)!
And again your wrong-I never asked for the paper or papers showing a probablility that "HIV" is associated with AIDS-defining diseases-that was clear with Montagnier's first paper describing patient 1, who had had 2 cases of gonnorhea, had been treated for syphilis, had had herpes 1, and 2, CMV, and provided the first "isolate." All I have been asking for is a little bit of consistent logic-doesn't have to be even published yet. How could a child die of an AIDS-defining illness, who was not on any antiretrovirals, if she had 10,800 T-cells, unless of course, T-cell numbers have nothing to do with AIDS?
Dear Adele,
I thought you weren't gonna fuss with me anymore! Glad your back.
RE:
"No one ever claimed it! "Another guy" is science illiterate or pretending to be. Antivirals don't "cure" HIV infection they keep the virus from replicating. They do it damn well."
Well, I suppose it depends on what your definition of well, is....
HIV Med 2002 Jul;3(3):195-9
Causes of death among HIV-infected patients in the era of highly active antiretroviral therapy, Bordeaux, France, 1998-1999.
Bonnet F, Morlat P, Chene G, Mercie P, Neau D, Chossat I, Decoin M, Djossou F, Beylot J, Dabis F; Groupe d'Epidemiologie Clinique du SIDA en Aquitaine (GECSA).
Federation de Medecine Interne, Maladies Infectieuses et Pathologie Tropicale, Hopital Saint-Andre Bordeaux, France. fabrice.bonnet@chu-bordeaux.fr
OBJECTIVES: To describe the causes of death in HIV-infected patients in the era of highly active antiretroviral therapy (HAART). METHOD: A retrospective survey conducted in Bordeaux, France. Medical records of all deaths that had occurred in 1998 and 1999 amongst patients followed within the Aquitaine cohort were reviewed by the same physician. Immediate and underlying causes of death were described, taking into account the morbidity at the time of death. RESULTS: Sixty-six deaths occurred in 1998, and 41 in 1999. Sixty-seven per cent of deceased patients were male. Median age at time of death was 43 years (range 25-71), median CD4 was 162 cells/microL (0-957); 28% of patients had a CD4 count > 200 cells/microL and 7% plasma viral load < 500 HIV-RNA copies/mL. Amongst morbidity present at the time of death, there were 23 bacterial infections, 16 non-Hodgkin's lymphomas, 16 cirrhoses, 15 non HIV-related malignancies, 13 central nervous system diseases and 10 myocardiopathies. The main immediate causes of death were: multiple organ failure (21%), coma (18%), septic shock (15%) and acute respiratory failure (14%). Underlying causes of death were AIDS-defining events (48%), non AIDS HIV-related infection (3%), hepatitis B- or C-associated cirrhosis (14%), non HIV-related malignancies (11%), cardiovascular events (10%), suicide and overdose (6%), treatment-related fatalities (4%), injury (2%) and unknown (2%). Patients dying from AIDS-related events were more often female, had a lower CD4 count, a higher level of HIV-RNA, a shorter history of HIV infection and were less often coinfected with hepatitis B and C viruses than those dying from other underlying causes. CONCLUSIONS: AIDS-related events are no longer the major causes of death of HIV-infected patients in the era of HAART. This evolving mortality pattern justifies an adaptation of both the epidemiological surveillance and the clinical monitoring of HIV-infected patients.
Hamilton JD et al. A controlled trial of early versus late treatment with zidovudine in symptomatic human immunodeficiency virus infection. NEJM. 1992;326(7):437-43.
"after starting antiretroviral treatment...the estimated probability of developing lymphoma ...by 36 months, [was] 46.4% (CI, 19.6% to 75.5%)...a direct role of therapy itself cannot be totally discounted...Zidovudine can act as a mutagen."
Buchbinder S et al. Long-term HIV-1 infection without immunologic progression. AIDS. 1994;8:1123.
"Leukopenia [white blood cell deficiency] occurred in 82% of the patients receiving early therapy and 77% of those receiving late therapy [AZT only when AIDS occurred]; 20% and 16%, respectively, had anemia. 14% and 10%, respectively, had severe leukopenia...and 5% and 2% had severe anemia requiring transfusion. Nausea (or vomiting) and diarrhea occurred more frequently in the early-therapy group than in the late-therapy group (40% vs. 23%, respectively; P <0.01)...The dosage of blinded study medication was reduced because of adverse reactions in 64 [38%] of the patients assigned to zidovudine (early therapy) and in 29 [17%] of those assigned to placebo (late therapy)...Once AIDS developed in patients receiving early therapy, more of them tended to have multiple AIDS diagnoses, a slightly higher proportion died, and the median survival time was slightly shorter than in similar patients who received late therapy."
Chaisson RE, Keruly JC, Moore RD. Sex, race, drug use and progression of human immunodeficiency virus disease. NEJM. 1995;333(12):751-6.
"A total of 172 (96 Immediate treatment, 76 Deferred treatment) participants died [169 while taking AZT, 3 while on placebo]...The results of Concorde do not encourage the early use of zidovudine in symptom-free HIV-infected adults. They also call into question the uncritical use of CD4 cell counts as a surrogate endpoint for assessment of benefit from long-term antiretroviral therapy...Representatives of the Wellcome Foundation [Glaxo Wellcome manufactures AZT] who were also members of the Coordinating Committee have declined to endorse this report."
Hogervorst E et al. Predictors for non- and slow progression in HIV type-1 infection: low viral RNA copy numbers in serum and maintenance of high HIV-1 p24-specific antibody levels. JID. 1995;171:811-21.
"The mortality rate was significantly higher among [a group of 1372] patients who had received antiretroviral therapy [principally AZT] before enrollment in the clinic."
Phillips AN, Smith GD et al. Viral load and combination therapy for Human Immunodeficiency Virus. NEJM. 1997 Mar 27;336(13), www.nejm.org/content/1997/0336/0013/0958.asp.
"participants of open-label ZDV [AZT] still had four to five times the incidence of ARC/AIDS/death of participants on blinded therapy [of which approximately half were on AZT and half on placebo]...The unadjusted hazard of ARC/AIDS/death was 4.6 times higher for participants [in the deferred group] who had received ZDV...after adjustment for latest CD4 this became 1.6...There was a suggestion of a benefit in terms of [slower] progression to ARC, AIDS or death [with AZT], no effect on progression to AIDS or death, and a suggestion of an increase in mortality."
Reinvang I et al. Only temporary improvement in impaired neuropsychological function in AIDS patients treated with zidovudine. AIDS. 1991;5(2):228-9.
"thirteen subjects of 146 tested who were negative for HIV antigen before treatment later had detectable levels of antigen during the 128 weeks of treatment."
Sheppard HW, Ascher MS, Krowka JF. Viral burden and HIV disease. Nature. 1993 Jul 22;364(6435):291-2.
"The large Anglo-French Concorde randomized trial of zidovudine in asymptomatic HIV-infected individuals shows that there is no significant clinical benefit in terms of survival or disease progression to AIDS or AIDS-related complex (ARC) in those who started zidovudine immediately rather than those who waited for the onset of symptomatic disease. The1749 participants were followed up for an average of 3 years."
Phillips, AN, Sabin CA. Zidovudine in Asymptomatic HIV Infection. NEJM. 1993 Dec 16;329:25, http://www.nejm.org/content/1993/0329/0025/1895.asp.
"the high level of plasma virus observed by Piatak et al, was about 99.9 per cent non-culturable, suggesting that it was either neutralized or defective. Therefore, rather than supporting a cytopathic model, this observation actually may help explain the relatively slow dissemination of the infected cell burden and thus the relative ineffectiveness of therapy with nucleoside analogues which target this process."
Sperling RS et al. Maternal viral load, zidovudine treatment and the risk of transmission of human immunodeficiency virus type 1 from mother to infant. NEJM. 1996;335(22):1621-9.
"AZT can be severely toxic, and there is compelling evidence that the drug probably doesn't help infected people live longer unless they already have full-blown AIDS...AZT clearly isn't a very effective anti-AIDS drug."
Swanson CE, Cooper DA. Factors influencing outcome of treatment with zidovudine of patients with AIDS in Australia. AIDS. 1990;4(8):749-57.
"Of the 524 subjects enrolled [in this study of people in the early stages of AIDS and HIV antibodies], 4 never received zidovudine [AZT], 41 completed the study, and 479 were withdrawn from zidovudine treatment [i.e. virtually everyone]. The reasons for withdrawal from zidovudine were the development of an opportunistic infection or a neoplasm [cancer]...(54 subjects); death (43); toxic reactions (183); withdrawal by the subject (169) and other reasons (30)...[of the] 183 subjects withdrawn...because of toxic reactions, zidovudine was discontinued earlier in more subjects in the standard-treatment group than in the low-dose group [40% vs. 29%]. Among the symptoms only headache was noted more frequently in the low-dose group...22 subjects (8%) in the standard-treatment group and 27 (10%) in the low-dose group had elevated levels of hepatic [liver] enzyme...178 subjects (34%) had a hemoglobin concentration below 5 mmol per liter [anemia]...134 subjects (26%) received red-cell transfusions (65 in the standard-treatment group and 69 in the low-dose group)...230 subjects(44%) had a [low] neutrophil [infection fighting white blood cells] count...134 (51%) in the standard-treatment group and 96 (37%) in the low-dose group...22 subjects (4%) had a [low] platelet [blood clotting cells] count."
Fischl MA et al. A randomized controlled trial of a reduced daily dose of Zidovudine in patients with the Acquired Immunodeficiency Syndrome. NEJM. 1990;323(15):1009-14.
"We report a patient who experienced acute cholestatic hepatitis on initial exposure to and rechallenge with zidovudine and, as a result, was unable to receive further therapy with the drug...Seven days [after starting AZT therapy] the patient presented with a 2-day history of intermittent fevers and abdominal discomfort...Seven days [after re-starting AZT therapy once the initial symptoms resolved] the patient again experienced fever, right upper quadrant pain, nausea, and headache...One month later [after discontinuing AZT] the liver function tests had almost completely returned to normal and remained without significant abnormalities."
Dubin G, Braffmann MN. Zidovudine-induced hepatotixicity. Ann Int Med. 1989;110(1):85-6.
"58% of all subjects with AIDS and AIDS-related complex receiving zidovudine experienced granulocytopenia of grade 3 or higher...Serious anemia occurred in 32% of all subjects receiving zidovudine...and could be typically managed by dose attenuation, temporary dose interruption of zidovudine therapy and/or red blood cell transfusions...12% of subjects...had an episode of thrombocytopenia [low platelet count] after the initiation of zidovudine therapy...Ten patients had liver enzyme levels elevated...and were managed with dose attenuations or interruptions of zidovudine therapy...One report of a grand mal seizure, two events associated with cardiac dysfunction, and five reports of myopathy were the only new serious potentially drug-related adverse events reported during extended periods of zidovudine administration."
Fischl MA et al. Prolonged zidovudine therapy in patients with AIDS and advanced AIDS-related complex. JAMA. 1989;262(17):2405-10.
"AZT was started at full dose in 260 patients, 64 with ARC and 196 with AIDS. In 58 of these patients, AZT had to be stopped at least once for a minimum of 7 days. In 142 other patients, dosage was reduced by half because of leucopenia (79), leucopenia and anaemia (32), anaemia (20), rash (3), vomiting (3), headaches and insomnia (2), myalgia (2), or hepatitis (1). 3 patients reduced the dose with no medical reason. Later on, progression of toxicity led to suspension of AZT (for at least 7 days) in 85 of the 142 patients whose treatment had been reduced to half dose. Thus AZT was stopped at least once in 143 (55%) patients who began the full-dose regimen. Because of their initial haematological status 105 (28.8%) patients were treated from the start with half-dose AZT - toxicity led to cessation of treatment in 71 (67.6%) cases"
Dournon E et al. Effects of zidovudine in 365 consecutive patients with AIDS or AIDS-related complex. Lancet. 1988 Dec 3;2:1297-1302.
Harmful Effects on Blood and Bone Marrow
"We found that 78.2% of the patients with mild or severe anaemia at baseline had received zidovudine [AZT]"
Mocroft A et al. Anaemia is an independent predictive marker for clinical prognosis of HIV-infected patients from across Europe. AIDS. 1999;13:943-50.
"The hematocrit [red blood cell count] decreased in the same patients...with three of eight patients requiring red-cell transfusion by the fourth week of treatment."
Hymes KB et al. The Effect of Azidothymidine on HIV-related Thrombocytopenia. NEJM. 1998 Feb 25;318(8):516-7.
"While effective drug therapy is continued in zidovudine[AZT]-treated HIV-infected patients...PROCRIT Reduces Transfusion Requirements and Helps Lift the Burden of Anemia."
Advertisement for PROCRIT. 1997.
"178 subjects (34%) had a hemoglobin concentration below 5 mmol per liter [anemia]...A greater proportion of subjects in the standard-treatment [high dose AZT] group had a first episode of severe anemia earlier in the study, as compared with the proportion in the low-dose group. 134 subjects (26%) received red-cell transfusions (65 in the standard-treatment group and 69 in the low-dose group)...230 subjects(44%) had a [low] neutrophil [infection fighting white blood cells] count...134 (51%) in the standard-treatment group and 96 (37%) in the low-dose group...22 subjects (4%) had a [low] platelet [blood clotting cells] count."
Fischl MA et al. A randomized controlled trial of a reduced daily dose of Zidovudine in patients with the Acquired Immunodeficiency Syndrome. NEJM. 1990;323(15):1009-14.
"Zidovudine is well known to produce haematological toxicity in vitro and in some patients...It is worrying that bone marrow changes in patients on zidovudine seem not to be readily reversed when the drug is withdrawn...These findings have serious implications for the use of zidovudine in HIV positive but symptom-free individuals."
Mir N, Costello C. Zidovudine and Bone Marrow. Lancet. 1988 Nov 19;1195-6.
"nearly one half of patients treated with AZT for [HIV]-associated disease develop transfusion-dependent anaemia due to bone marrow depression"
Dainiak N et al. 3'-Azido-3'-deoxythymidine (AZT) inhibits proliferation in vitro of human haematopoietic progenitor cells. British Journal of Haematology. 1988;69:299-304.
"Blood transfusion is often necessary in patients with AIDS, especially in those receiving AZT, a drug which produces severe anaemia in a proportion of recipients. Forty nine (36%) of 138 patients treated with AZT ... required blood transfusion at least once."
Costello C. Haematological abnormalities in human immunodeficiency virus (HIV) disease. J Clin Pathol. 1988;41:711-5.
"In the current study, transfusion-dependent anemia occurred in 6 of 15 patients with AIDS and Kaposi sarcoma who were receiving zidovudine therapy. All 6 affected patients required their first blood transfusion between 3 and 9 weeks after starting zidovudine therapy, and each required 4 to 14 units of packed erythrocytes to maintain a hemoglobin level above 100 g/L over a 12-week study."
Walker RE et al. Anemia and erythropoiesis in patients with the acquired immunodeficiency syndrome (AiDS) and Kaposi sarcoma treated with zidovudine. Ann Int Med. 1988;108:372-6.
"more than half of all AIDS patients may not benefit from the drug because it is more toxic for them than their AIDS infection. The most serious side effect of AZT is to suppress the bone marrow, leaving patients highly vulnerable to bacterial infections"
Kolata G. Imminent marketing of AZT raises problems; marrow suppression hampers AZT use in AIDS victims. Science. 1987 Mar 20;235:1462-3.
"Anemia...developed in 24% of AZT recipients and 4% of placebo recipients (P<0.001). 21% of AZT recipients and 4% of placebo recipients required multiple red-cell transfusions (P<0.001). Neutropenia (<500 cells per cubic millimeter) occurred in 16% of AZT recipients, as compared with 2% of placebo recipients (P<0.001)."
Richman DD et al. The Toxicity of Azidothymidine (AZT) in the Treatment of Patients with AIDS and AIDS-Related Complex. NEJM. 1987;317:192-197.
"Four patients with [AIDS], and a history of Pneumocystis carinii pneumonia developed severe pancytopenia [marked decrease in all types of blood cells]...12 to 17 weeks after the initiation of azidothymidine (AZT) therapy...Partial bone marrow recovery was documented within 4 to 5 weeks in three patients, but no marrow recovery has yet occurred in one patient during the more than 6 months since AZT treatment was discontinued."
Gill PS et al. Azidothymidine Associated with Bone Marrow Failure in the Acquired Immunodeficiency Syndrome (AIDS). Ann Int Med. 1987;107:502-505.
Muscle Disorders (including Heart)
"Long term therapy with [AZT] can induce a toxic myopathy associated with mitochondrial changes"
Chariot P, Gherardi R. Partial cytochrome c oxidase deficiency and cytoplasmic bodies in patients with zidovudine myopathy. Neuro muscul Disorders. 1991;1:357-363.
"typical mitochondrial myopathy has been reported to be expressed among many patients with AIDS treated with long-term azidothymidine (AZT) therapy" and "for AIDS patients, it is urgently necessary to develop a remedy substituting this toxic substance, AZT"
Hayakawa M et al. Massive conversion of guanosine to 8-hydroxy-guanosine in mouse liver mitochondrial DNA by administration of azidothymidine. Biochem Biophys Res Commun. 1991;176:87-93.
"A clinically significant myopathy that precedes the development of zidovudine associated mitochondrial myopathy has been a rarity in our experience."
Coker R et al. Exacerbation of HIV-associated myopathy by zidovudine. AIDS. 1991;5(2):229-31.
"Before 1986, when zidovudine (formerly called azidothymidine [AZT]) was introduced...the number of patients with HIV-associated myopathy was small, and myopathy [muscle disorders] was considered a rare complication of HIV infection. During the past two years [1988-1989], an increasing number of patients receiving long-term zidovudine therapy have had myopathic symptoms such as myalgia (in up to 8 percent of patients), elevated serum creatine kinase levels (in up to 15 percent), and muscle weakness. These symptoms generally improve when zidovudine is discontinued...We conclude that long-term therapy with Zidovudine can cause a toxic mitochondrial myopathy, which... is indistinguishable from the myopathy associated with primary HIV infection."
Dalakas MC et al. Mitochondrial myopathy caused by long-term zidovudine therapy. NEJM. 1990;322(16):1098-1105.
"In our review of our clinic patients who have received zidovudine therapy for more than 6 months, 16% (14 of 86 patients) have had persistently elevated creatine kinase values. Six percent of these patients (5 of 86) developed symptomatic myalgia and objective proximal muscle weakness. These 5 symptomatic patients had received zidovudine for an average of 45 weeks and had had creatine kinase elevations for several weeks before onset of symptoms. Of these 5 patients, 4 had creatine kinase values return to normal and symptoms resolve after zidovudine was withdrawn...Three patients were rechallenged with zidovudine: each had recurrent creatine kinase elevations at a dose of 600 mg/d. The zidovudine dose was increased to 1200 mg/d in 2 patients: after a few days, both developed recurrent muscle symptoms that again responded to dose reduction. ...Results of quadriceps muscle biopsies done on our patients who responded to zidovudine withdrawal showed severe myopathic changes without evidence of inflammatory infiltrates. Electron microscopy revealed many ultrastructural changes, including destruction of the sarcomere profile with z-band change in the form of streaming and rod bodies. Muscle mitochondria showed wide variation in size, swelling, degeneration and laminar bodies. ...There have been 40 case reports [to 1990] of patients who have developed myopathy while taking zidovudine (including our 5 symptomatic patients). Zidovudine therapy was discontinued in 34 of these patients and 26 improved."
Till M, MacDonnell KB. Myopathy with Human Immunodeficiency Virus type 1 (HIV-1) infection: HIV-1 or zidovudine?. Ann Int Med. 1990;113(7):492-4.
"A severe proximal myopathy, predominantly affecting the legs, seems to be a significant complication of long-term zidovudine therapy, even at reduced doses; it affected 18% of our patients who had received treatment for more than 200 days. Other drugs could not be implicated. The pathogenesis is obscure; the myopathy resolves on cessation of zidovudine, but not on dose-reduction, though there is then a risk of rebound encephalitis."
Buchbinder S et al. Long-term HIV-1 infection without immunologic progression. AIDS. 1994;8:1123 reported that:
"Only 38% of the HLP [Healthy long-term positives] had ever used zidovudine [AZT] or other nucleoside analogues, compared with 94% of the progressors."
Pluda et al. Development of Non-Hodgkin Lymphoma in a Cohort of Patients with Severe Human Immunodeficiency Virus (HIV) Infection on Long-Term Antiretroviral Therapy. Ann Int Med. 1990;113:276-282 claimed that AZT caused cancer:
"after starting antiretroviral treatment...the estimated probability of developing lymphoma ...by 36 months, [was] 46.4% (CI, 19.6% to 75.5%)...a direct role of therapy itself cannot be totally discounted...Zidovudine can act as a mutagen"
Costello (1988) reported the Journal of Clinical Pathology that, "Blood transfusion is often necessary in patients with AIDS, especially in those receiving AZT, a drug which produces severe anaemia in a proportion of recipients. Forty nine (36%) of 138 patients treated with AZT required blood transfusion at least once."
Harrison's Principles of Internal Medicine states: "[AZT], used for treating [HIV], often causes severe megaloblastic anemia caused by impaired DNA synthesis."
Writing in the journal Palliat Med. 1997 Mar;11(2):152-8, Kelleher P, Cox S, McKeogh M. published a report entitled, "HIV infection: the spectrum of symptoms and disease in male and female patients attending a London hospice," in which they concluded that:
"Lack of strong evidence exists for sustained immune reconstitution by current therapies [comprising AZT and other drugs, and AZT may] unmask silent opportunistic infections." Not only can AZT "unmask silent opportunistic infections, it can exacerbate clinically conspicuous ones."
AZT has some of the following caveats on the AZT package insert printed in bold and CAPITALIZED type:
"WARNING: RETROVIR (ZIDOVUDINE, AZT) MAY BE ASSOCIATED WITH HEMATOLOGIC TOXICITY INCLUDING GRANULOCYTOPENIA AND SEVERE ANEMIA PARTICULARLY IN PATIENTS WITH ADVANCED HIV DISEASE." (underline is mine).
"PROLONGED USE OF RETROVIR HAS BEEN ASSOCIATED WITH SYMPTOMATIC MYOPATHY SIMILAR TO THAT PRODUCED BY HUMAN IMMUNODEFICIENCY VIRUS. RARE OCCURRENCES OF LACTIC ACIDOSIS IN THE ABSENCE OF HYPOXEMIA, AND SEVERE HEPATOMEGALY WITH STEATOSIS HAVE BEEN REPORTED WITH THE USE OF ANTIRETROVIRAL NUCLEOSIDE ANALOGUES, INCLUDING RETROVIR AND ZALCITABINE, AND ARE POTENTIALLY FATAL."
Other benefits of AZT that have been listed on the AZT package insert also
include:
"Persistent headaches lasting longer than 1 month, anemia, dementia, diarrhea,
muscle wasting, candidiasis, non-specific oral lesions, severe fatigue,
enlarged liver and liver failure, heart failure, diabetes, unmasking of opportunistic
infections including CMV retinitis, spontaneous bleeding in hemophiliacs, lymphoma, severe skin rashes, Stevens-Johnson syndrome, and other toxic reactions, back pain, body odor, chest pain, chills, edema of the lip, fever, flu syndrome, hyperalgesia, syncope, vasodilation, bleeding gums, constipation, dysphagia, edema of the tongue, eructation, flatulence, mouth ulcer, rectal hemorrhage, lymphadenopathy, arthralgia, muscle spasm, tremor, twitch, anxiety, confusion, depression, dizziness, emotional lability, loss of mental acuity, nervousness, paresthesia, somnolence, cough, dyspnea, epistaxis, hoarseness, pharyngitis, rhinitis, sinusitis, acne, changes in skin and nail pigmentation, pruritus, rash, sweat, urticaria, amblyopia, hearing loss,
photophobia, taste perversion, dysuria, polyuria, urinary frequency, urinary hesitancy."
"Zidovudine was administered orally at three dosage levels to separate groups of mice and rats (60 females and 60 males in each group). Initial single daily doses were 30, 60, and 120 mg/kg/day in mice and 80, 220, and 600 mg/kg/day in rats. The doses in mice were reduced to 20, 30, and 40 mg/kg/day after day 90 because of treatment- related anemia, whereas in rats only the high dose was reduced to 450 mg/kg/day on day 91 and then to 300 mg/kg/day on day 279."
"In mice, seven late-appearing (after 19 months) vaginal neoplasms (5 nonmetastasizing squamous cell carcinomas, one squamous cell papilloma, and one squamous polyp) occurred in animals given the highest dose. One late-appearing squamous cell papilloma occurred in the vagina of a middle dose animal. No vaginal tumors were found at the lowest dose."
"In rats, two late-appearing (after 20 months), non-metastasizing vaginal squamous cell carcinomas occurred in animals given the highest dose. No vaginal tumors occurred at the low or middle dose in rats. No other drug-related tumors were observed in either sex of either species."
"It is not known how predictive the results of rodent carcinogenicity studies may be for humans. At doses that produced tumors in mice and rats, the estimated drug exposure (as measured by AUC) was approximately 3 times (mouse) and 24 times (rat) the estimated human exposure at the recommended therapeutic dose of 100 mg every 4 hours." " In the presence of metabolic activation, the drug was weakly mutagenic at concentrations of 1000 A?g/ml and higher. In an in vitro mammalian cell transformation assay, zidovudine (AZT) was positive at concentrations of 0.5 ug/ml and higher. In an in vitro cytogenetic study performed in cultured human lymphocytes, zidovudine induced dose-related structural chromosomal abnormalities at concentrations of 3 ug/ ml and higher."
"In two in vivo micronucleus studies (designed to measure chromosome breakage or mitotic spindle apparatus damage) in male mice, oral doses of zidovudine 100 to 1000 mg/kg/day administered once daily for approximately 4 weeks induced dose-related increases in micronucleated erythrocytes. Similar results were also seen after 4 or 7 days of dosing at 500 mg/kg/day in rats and mice." Nothing wrong with a few micronucleated cells or mitotic spindle damage.
"In a study involving 11 AIDS patients, it was reported that the seven patients who were receiving Retrovir (1200 mg/day) as their only medication for 4 weeks to 7 months showed a chromosome breakage frequency of 8.29ug/ml2.65 breaks per 100 peripheral lymphocytes. This was significantly (P< 0.05) higher than the incidence of 0.5ug/ml 0.29 breaks per 100 calls that was observed in the four AIDS patients who had not received Retrovir.
One also hears arguments stating that, "Not only is AZT safe and effective, but combined with protease inhibitors, the cocktail is virtually preventing everyone from advancing to "AIDS" who is compliant and takes all their meds on schedule." How in holy hell could this possibly be when when drug, AZT is toxic, carcinogenic, bone-marrow suppressive, etc., but added to highly toxic protease inhibitors, there is a beneficial effect?
For instance, Brinkman K et al., reported that "Mitochondrial toxicity induced by nucleoside-analogue reverse transcriptase inhibitors is a key in the pathogenesis of antiretroviral-related lipodystrophy." (Lancet. 1999 Sep 25;354:1112-15.1999):
"Highly active antiretroviral therapy (HAART) can induce a characteristic lipodystrophy syndrome of peripheral fat wasting and central adiposity. HIV-1 protease inhibitors are generally believed to be the causal agents, although the syndrome has also been observed with protease-inhibitor-sparing regimens. Here, we postulate that the mitochondrial toxicity of the nucleoside-analogue reverse-transcriptase inhibitors plays an essential part in the development of this lipodystrophy, similar to the role of mitochondrial defects in the development of multiple symmetrical lipomatosis."
Estaquier, et al., reported in an article entitled, "Effects of Antiretroviral Drugs on Human Immunodeficiency Virus Type 1-Induced CD4+ T-Cell Death" (Journal of Virology, Vol. 76, No. 12, p. 5966-5973, June 2002) that:
"We treated PBMC from HIV-seronegative healthy donors with increasing concentrations of IDV, SQV, or ddI for 3 days and monitored T-cell proliferation and cell death. Both IDV and SQV decreased T-cell proliferation mediated by CD3 MAb in three independent experiments performed with healthy donor cells with a mean decrease for SQV of 53% ± 15% and a mean decrease for IDV of 48% ± 12% (Fig. 4A). Moreover, in the absence of T-cell activation, we observed that 10 µM IDV and SQV induced a loss in membrane mitochondrial potential (m) as assessed by flow cytometry using DiOC6."
Martinez E et al., reported, "Risk of lipodystrophy in HIV-1 infected patients treated with protease inhibitors: a prospective cohort study" (Lancet. 2001;357(9256):592-8, 2001), and suggested that:
"Clinical research on lipodystrophy has usually rested on the idea that it was merely a complex adverse event related to individual antiretroviral agents or families of drugs...Our study suggests that the risk of lipodystrophy is mainly related to the total exposure to HAART and only to a lesser degree to specific antiretroviral drugs."
Tsiodras S et al., also described the "Effects of Protease Inhibitors on Hyperglycemia, Hyperlipidemia, and Lipodystrophy" (Arch Intern Med. 2000 Jul 10;160(13):2050-6, 2000), where they suggested that:
"Our study reports an independent association between PI [protease inhibitors] use and ... lipodystrophy, on the basis of a 5-year cohort study that encompassed the pre-PI and post-PI therapeutic eras. Although these metabolic changes were occasionally observed in patients not exposed to PIs, they were much more frequent after initiation of PI therapy."
Mauss concluded in an article he wrote entitled, "HIV-associated lipodystrophy syndrome. AIDS. 2000;14(suppl 3):S197-207, 2000, that:
"At present, HIV-associated liposystrophy is regarded by many investigators as a complication of antiretroviral therapy, in general, in combination with a variety of additional risk factors, and is not to be associated with any particular class of drugs...[even though]...treatment with dual nucleoside reverse transcriptase inhibitors appears to be associated with a lower prevalence of HIV-associated lipodystrophy as compared with triple-drug regimens including an HIV-protease inhibitor [which is perhaps why the syndrome was first called 'Crix belly', named after Crixivan, a protease inhibitor]"
Carr A, Miller J, Law M and Cooper D A., also reported, "A syndrome of lipoatrophy, lactic acidaemia and liver failure dysfunction with HIV nucleoside analogue therapy: contribution to protease inhibitor-associated lipodystrophy syndrome. (Aids 2000, 14 F25-F32, 2000) where they suggested that:
Miller et al., in an article entitled, "HIV lipodystrophy: prevalence, severity and correlates of risk in Australia" (HIV Med. 2003 Jul;4(3):293-301), that:
{In a cohort of} "One thousand, three hundred and forty-eight patients, lipodystrophy prevalence was 53%, and of these, 55% reported both peripheral lipoatrophy and central lipohypertrophy, 31% experienced peripheral lipoatrophy only and 14% had central lipohypertrophy only. The prevalence of any body habitus change was 62% in PI-experienced patients, 33% in PI-naive patients and 21% in antiretroviral-naive patients. Lipodystrophy severity was less in antiretroviral-naive patients and most severe in PI-experienced patients. Increasing severity of lipodystrophy was both positively and significantly correlated with elevated liver enzymes, decreased testosterone levels, decreased skin-fold thickness, lower levels of total and peripheral fat (DEXA) and higher levels of visceral fat (CT)."
Mora S, Sala N, Bricalli D et al., in an article entitled, "Bone mineral loss through increased bone turnover in HIV-infected children treated with highly active antiretroviral therapy" (AIDS. 2001 Sep 28;15(14):1823-9, 2001) claimed that:
"Bone mineral density (BMD) of total body and lumbar spine (L2-L4) was assessed by dual-energy X-ray absorptiometry in 40 children vertically infected with HIV: 35 taking HAART and 5 naive to any antiretroviral treatment (untreated). 6 HAART-treated children showed clinical evidence of lipodystrophy [abnormal fat redistribution]..."
Bica et al (2001) stated:
"In 1998-1999, 11 (50%) of 22 deaths were due to end-stage liver disease [a common side effect of AIDS drugs]... End-stage liver disease is now the leading cause of death in our hospitalized HIV-seropositive population."
Lederman MM, Valdez H. (2000), who are AIDS Researchers, recently published a study that claimed:
"Of recent HIV-related deaths occurring in the University Hospitals of Cleveland although OIs [Opportunistic Infections] constituted less than 25% of deaths in 1999, end-organ failures [which could well be caused by medication] constituted nearly half. Importantly, the median CD4 cell count among the patients who died in our clinic has risen, and about 20% of recent deaths have occurred among patients with plasma HIV RNA levels below the limit of detection."
The rising numbers of T-cells and undetectable viral load in the dying patients in this study show "just how effective AZT and HAART really is!!"
For a more up to date, 2006, look at HAART, from the National Institute of Health. HAART has saved 3,000,000 years worth of life, prevented an unknown but probably significant number of new infections because treated patients are much less able to transmit the virus, and has added an average of 13 years to patients lives. Under optimal conditions, it can add up to 20 years. Free country, everyone makes choices. Four years or 20 years.
I should add that medicine progresses rapidly. Who knows what treatments will be available 20 years from now?
Dear Raven,
Since you brought up the NIH, perhaps you should ask Jonathan M. Fishbein, M.D his opinion of the NIH and nevirapine specifically. He is the whistleblower who uncovered the nevirapine corruption and mismanagement at the NIH, the same people who gave us your "computer model" for how many lives are saved by toxic drugs. Next they will give us a computer model which explains why there is no water in the ocean. This is actually quite easy, go down to the beach, walk to the edge of the water, pick up a few rocks, take them back to the lab and analyze them. No water ? Ergo, there is no water in the ocean says the NIH computer model.
Sure you can believe the NIH: HAART has saved 3,000,000 years worth of life, or you can believe the LANCET a peer reviewed medical journal which says NO MORTALITY BENEFIT on 22,217 patients using the "miracle drug" cocktail called HAART.
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&cmd=Retrieve&dopt=Ab…
I will believe a study published in LANCET any day over a NIH computer model.
"INTERPRETATION: Virological response after starting HAART improved over calendar years, but such improvement has not translated into a decrease in mortality."
You wish to believe the NIH, be my guest. I dont.
Read this book, Science Sold Out: Does HIV Really Cause AIDS? by Rebecca Culshaw
LANCET a peer reviewed medical journal which says NO MORTALITY BENEFIT on 22,217 patients using the "miracle drug" cocktail called HAART.
This is not what the paper says. You can keep on repeating your misinterpretation but it will not make it true.
I will spell it out for you in small words.
The paper compared the outcomes of people iniating HAART between 1995 and 2003. The introduction of HAART saw a dramatic reduction in mortality. It had been hoped that improvements in HAART between 1995 and 2003 had translated into a further reduction in mortality. Unfortunately this was not the case.
Write to the authors and ask them whether they agree with your interpretation of the study.
For those who wish to read the LANCET article for themselves, rather than try to make any sense of the twisted logic of the previous AIDS apologist, here is a pdf:
http://www.antiagingforme.com/html/pdf/AIDS_Lancet2006.pdf
For those who believe the drug company HAART propaganda, ask why this LANCET study of 22,000 over 10 years shows that while HAART works quite well to reduce viral load and increase CD4 count, doing so fails to translate into a MORTALITY BENEFIT. i.e the theory is seriously flawed.
But of course, when the drug company profits pile up at the rate of $5,000 per month of HAART treatment, suddenly the drugs dont look so toxic, and the adverse side effects don't seem too hideous, in fact the drugs might even seem to appear "miraculous". Miraculous at making money that is.
For those who wish to read the LANCET article for themselves, rather than try to make any sense of the twisted logic of the previous AIDS apologist, here is a pdf:
Go ahead and read the article.
All groups were on HAART. Nowhere do they compare people on HAART with people not on HAART. It is simply not possible based on this study to claim that this demonstrates that HAART does not work.
Why do keep on claiming that this paper says something it clearly cannot.
People believe all sorts of weird things. It sometimes kills them. It is not unusual for anorexia patients to starve to death eventually in the mistaken belief that they are "too fat". Saw one myself.
From the way new IDs keep popping up with the same style and lack of logic, there is probably just one multi-ID person who chooses to deny reality. Feed the troll if you want for very minor amusement. The flat earthers are much more entertaining.
Ever notice how AIDS Apologists get snippy when the cost of a month of HAART treatment is mentiond? ($5,000 profit per month for the drug maker) Or is it because somebody's lunch ticket is blowing in the wind ?
In all of the HAART mortality studies, post-HAART era Mortality is compared to the pre-Haart era Mortality. The drug used during the pre-HAART era was AZT which was so successful at killing patients, even the docs refused to use it. Stop killing homeless drug addicts with AZT and give them the less toxic HAART instead and, of course, your drug study funded paper can now report improved mortality.
151 Children in South Africa were given HAART. 10 percent died shortly after starting HAART. In other words, the children were killed by HAART:
http://www.biomedcentral.com/content/pdf/1471-2431-7-13.pdf
Drug company profits from HAART are blood money, made from the deaths of these poor children.
Death from Liver toxicity, Mitochondrial dysfunction, disturbed neuro-development are a few of the adverse effects of your "miracle drug cocktail" HAART.
Ever see the face of a HAART user, there is a grotesque lipodystrophy "mask" which looks like the Phantom of the Opera.
There is another way, see this web site: livingwithouthivdrugs dot com
Back to the "liver toxicity" again, I see. How many times has that one been explained to Andrew I wonder? It goes like this.
Dog's Best Flies Maniotisfrog: Rebecca Someone said most AIDS patients die of HAART liver toxicity and she's right because sixteen Nobel prize winners agree with her.
Scientist: Well actually no Nobel prize winner agrees with that, because most AIDS patients on HAART today die of something besides AIDS because HAART is keeping them alive long enough to die of something else. A minority of AIDS deaths have liver toxicity and they're the people with Hepatitis B or C and usually injection drug users who have really messed up theyr livers.
DBF Maniotisfrog: Hah!! Hepatitis B and C don't exist. They're surrogate markers of drug use just like "HIV". And injection drugs can give you AIDS, but they can't hurt your liver.
S: No, injection drugs don't give anyone AIDS, but they can hurt the liver and especially if tainted needles pass Hep.
Dog's Best F. Maniotisfrog: Hah Hah! Here are sixty abstracts I pasted from somewhere and some stuff I copied from the internet and pretended it was mine. They prove I'm right. I think.
S: No, most of those studies aren't relevant. You can't just look at part of the abstract you have to read the whole study. Please stop taking stuff outta context.
DBFM: Well youre a Nuremberg criminal and when the spaceships come down, surely very soon, any day now when they prove EJ wasn't positive, we'll take you to the mothership and inject you with mercury from dead salmon that you killed with AZT.
Just wacko.
I'm with Raven. Since Andrew has now admitted to being these various denialists on here, I think he did anyway he's kind of vague so I'm not sure, and even if he didn't the other person is just as logically challenged, I'm done with this discussion. Someone else'll have to feed flies to the frog's best Andrewdog.
Well, the sockpuppet brigade is out in full force (of one).
Ever notice how AIDS Apologists get snippy when the cost of a month of HAART treatment is mentiond? ($5,000 profit per month for the drug maker) Or is it because somebody's lunch ticket is blowing in the wind ?
Who got snippy? The drugs work, they extend lives. Personally, I'd love to see them cost less. Sockpuppet is using ad hominem, poisoning the well and strawman arguements.
BTW, apologists are individuals that take an extreme position that is unpopular or negatively viewed by the population being examined. By definition, the denialists are acting as apologists for the Duesberg/ Perth groups.
151 Children in South Africa were given HAART. 10 percent died shortly after starting HAART. In other words, the children were killed by HAART:
Another lie. The 13 who died during the trial had advanced AIDS before they began treatment (6 of 13 were WHO stage 4, 7 were stage 3, 10 were in the 5th or lower weight percentile for their age, 10 had chronic gastroenteritis). Earlier treatment and special care for children with gastroenteritis were suggested. If the drug was causing the deaths, mortality should have continued to rise as the trial continued. It didn't. The mortality rate dropped off, with deaths by month listed as 3 in month 1, 5 in month 2, 3 in month 3, 1 in month 4 and 1 in month 5, with no more deaths in the 24 months of the trial. 3/4 of all children in the trial had marked weight gains in the first month of treatment. This isn't what you would predict if the drug was killing the patients. It is, however, what you would predict if the drug was preventing deaths, understanding that some already ill patients may not make it. The treatment cost was $10 US per month. Read the paper.
This is the same thing that creationists do. They link to a paper that they say proves a young earth or a special creation, but when you read the paper, it becomes clear that they are lying about what the paper says.
Death from Liver toxicity, Mitochondrial dysfunction, disturbed neuro-development are a few of the adverse effects of your "miracle drug cocktail" HAART.
But the clinically important effect is that the patients live longer and experience fewer opportunistic infections. This is constantly omitted by the denialists.
Dear Adele,
Thanks for the rather bizarre fictional satire which belongs over at science fiction blogs.
For the lurkers fed up with Orwellian DoubleSpeak, try this web site for better quality info:
reviewingaids dot org
I'm getting really tired of the wild and deliberate distortions of Maniotis and his various sock puppets.
This is one of the latest, courtesy of "dog's breakfast":
Of course the article says no such thing. AIDS kids in SA have a high mortality rate. In this study, following HAART, the 1 year survival was 90% - a pretty astounding result showing effectiveness of the drugs. And those who died were not "killed by HAART" as "dog's breakfast" claims.
The Kaplan Meier (presented in Figure 3) mortality survival estimate at 12 months was 90.9% (95%CI 84.8- 94.6). Paediatric mortalities are summarized in Table 4. All 13 deaths occurred within the first 5 months of HAART initiation. No deaths were attributed to metabolic disorders or other drug-related adverse effects. Autopsy data were not available, but the most commonly reported causes of death were chronic gastroenteritis (n = 6) and TB (n = 4). Other causes of death included: sepsis syndrome (n = 1), suspected PCP (n = 1), and a respiratory tract infection (n = 1).
So these kids died of opportunistic infections, not HAART drugs. You'd think that with the entire internet at their disposal that the HIV denialists could come up with a study that actually shows what they claim..... but no. They are incapable of finding even one.
Dear Adele,
Please don't be mad at me. I learn quite a bit from all your posts. You don't have to call me andydog and stuff though. Andy will do fine.
BTW... These "viruses" aren't just surrogate markers of drug use-I suppose in many cases they are and this has been shown again and again, but there are at least 70 other reasons for testing positive including such "diseases" as multiple pregnancies, lupus, a recent flu injection (about 2% according to Klausner will test positive after a flu shot), lupus, malaria, etc, parisitic infections, etc.
Get some rest Adele!
Dear Raven,
What are hypothetical people with AIDS in the NIH study that is posted in response to the studies I posted?
E.G.
"For each year of the six eras, the investigators ran simulations of HIV disease progression in two equal-sized groups of hypothetical people with AIDS. One group received no therapy, while the other group received all available therapies of that era."
RE:
"The total cumulative survival benefit across all eras from all forms of HIV therapy was 2.8 million years."
2.8 million years is a long time. I guess this means if you started treating Lucy (the Australopithicine), she would still be alive today!
I must admit, compared to the studies I posted, this one done by the NIH is really a hum dinger to end all arguments or questions about immune suppression, and how to treat it.
Perhaps this should not come as so much of a surprise because Dr. Fauci, before the AIDS era, claimed that immune suppression is caused by doctors! Doctors cause immune suppression, Fauci claimed, if they subject their patients to multiple transfusions, transplant surgery, or corticosteroid administration, as these drugs and treatments can non-specifically induce AIDS-specific drops in T-cells with high frequency (1, 2). Fibrosis of the lung due to to heavy crack cocaine use also was considered a potent inducer of the AIDS-defining illness, PCP, by Fauci and others before the AIDS era. These qualifications serve to undermine the "HIV=AIDS" hypothesis, because A ("HIV"), does not generate B (immune suppression), because iatrogenically applied glucocorticoids, transfusions, blood factor concentrates in hemophiliacs, and other factors may induce a precipitous drop in B, and consequently lead to C. Thus, this is AIDS denialism, as it denies the existence of "HIV," or the need to detect "HIV," altogether, in a patient with low (B), while suggesting that doctors, and illicit drug use, cause "AIDS-like" immune suppression.
Some AIDS researchers such as Gisselquist et al. who have studied Africa and African AIDS extensively also claim that "HIV/AIDS" is caused mostly by doctors! The reasons in support of the Gisselquist et al. claims published in the journal AIDS and elsewhere include:
"An expanding body of evidence challenges the conventional hypothesis that sexual transmission is responsible for more than 90% of adult HIV infections in Africa. Differences in epidemic trajectories across Africa do not correspond to differences in sexual behavior. Studies among African couples find low rates of heterosexual transmission, as in developed countries. Many studies report HIV infections in African adults with no sexual exposure to HIV and in children with HIV-negative mothers. Unexplained high rates of HIV incidence have been observed in African women during antenatal and postpartum periods. Many studies show 20%-40% of HIV infections in African adults associated with injections (though direction of causation is unknown). These and other findings that challenge the conventional hypothesis point to the possibility that HIV transmission through unsafe medical care may be an important factor in Africa's HIV epidemic. More research is warranted to clarify risks for HIV" [3].
"The assumption that historic and continuing high rates of epidemic increases among African adults are almost exclusively due to sexual transmission requires much higher rates of heterosexual transmission in Africa than in the developed world. However, a recent study of HIV incidence in serodiscordant couples in Africa (only 1.2% reported consistent condom use) estimated a rate of transmission per coital act of only 0.0011, comparable to rates of 0.0003-0.0015 from similar studies in the US and Europe [3].
"A study in Kinshasa in 1985 found 39% (17 of 44) of HIV-positive inpatient and outpatient children 1-24 months old to have HIV-negative mothers; only five of 16 (with information) had been transfused... In a later report from Rwanda, 7.3% (54 of 704) of mothers of children with AIDS were HIV-negative; transfusions were identified as the risk factor for 22 of the 54 children... rates of unexplained incidence among African women are comparable to rates of maternal mortality from puerperal fever of 6% to 16% observed by Semmelweis during 1841-46 in the First Clinic at the University of Vienna's obstetric department. "[3].
"Starting in the 1950s Africans experienced a massive increase in medical injections associated with mass injection campaigns targeted at yaws, with introduction and spread of parenteral therapies to treat other diseases, and with plummeting prices for antibiotics and injection equipment. For example, UNICEF administered 12 million injections for yaws in Central Africa alone during 1952-57. From the 1950s into the 1980s, unsafe injections may have contributed to the silent spread of HIV in Africa in much the same way that unsafe injections for schistosomiasis and other treatments in Egypt established hepatitis C as a major blood-borne pathogen, infecting about 15% to 20% of the general population at the end of the 1990s"[3].
"Our observations raise the serious possibility that an important portion of HIV transmission in Africa may occur through unsafe injections and other unsterile medical procedures"[3].
"More recently, nearly 400 children attending a single hospital in Libya apparently contracted HIV" [3].
Currently, there are 5 nurses and 1 doctor thought responsible for this transmission of "HIV" to these 400+ children (the Tripoli Six), and they are scheduled to be executed by firing squad in Libya.
1. Fauci, A.S. Mechanisms of Corticosteroid Action on lymphocyte Subpopulations I. Redistribution of circulating T and B lymphocytes to the bone marrow. Immunology 28: 669-679. 1975.
2. Fauci, A.S., Dale, D.C., and Balow, J.E. Glucocorticosteroid therapy: Mechanisms of Action and Clinical Considerations. Annals of Internal Medicine 84: 304-15, 1976.
Thanks so much!
Cheers,
Andy
Sorry-forgot ref. 3...
3. Editorial with Gisselquist, statistics quoted from: International Journal of STD & AIDS Royal Society of Medicine, October 2002 Africa HIV/AIDS through unsafe medical care. Also available: Africa Policy E-Journal. www.africaaction.org/docs02/hiv0210t.htm
Andrew, use of contaminated needles as a route of HIV transmission supports the HIV/AIDS theory, not removes support. Also, can you at least try to come up with something far less silly than HIV is a biomarker for drug abuse? It is complete malarky, as evidenced from non-abusing patients, blood transfusion as a route of transmission and health care workers becoming infected after an accidental needlestick (never mind all the thousands of papers contradicting you).
In fact, some of the best proof comes from studies regarding the CCR5Delta32 mutant receptor. This mutant can decrease the capacity for HIV to infect the cells of the CCR5Delta32 carrier. Even when repeatedly exposed to HIV, CCR5Delta32 carriers tend to resist infection, while those who have two copies of the mutant are almost impossible to infect with HIV and consequently, don't develop AIDS.
Duesberg's abuse hypothesis is based on a spurious correlation, and if you were honest, you would admit it.
-------------------
Does anybody remember the name of the AIDS patient who bought into the denialist lies, and later died from an OI? The denialists said that he had started abusing illegal drugs causing his death, instead of the OI. I think it would be a worthwhile read for observers.
I see they have passed the point of making stuff up and are now just babbling nonsense. A subset of HIV/AIDS patients are pediatric, babies born to HIV+ mothers. Untreated, they can progress rapidly to death. Rather unbelievable that newborn babies are roaming the streets buying drugs and shooting up.
Besides which, many HIV+ have no history of injecting or abusing drugs.
Besides which, many HIV+ have no history of injecting or abusing drugs. -- raven
Oh really?
What about all of the harmful prescription medications that Americans are ingesting at a record pace, and I'm not just talking about HIV meds being harmful. Duesberg was on the right track but he failed to realize, and therefore, failed to stress strongly enough, just how damaging certain prescription medications can be to one's immune system, even though they considered "safe" and FDA-approved. Of course, that situation is only now becoming apparent, so perhaps we can forgive Dr. Duesberg that small fault.
For those readers who prefer to deal with the dangerous realities of our dysfunctional and failing healthcare system, I highly recommend the following two books:
Selling Sickness
and
Overdosed America
For those readers uninterested in reality, how's the housing market looking in your area?
Kevin
Andy,
I really hope that you teach your students to read the scientific literature more carefully and critically than you apparently do yourself. First, as already pointed out above, Gisselquist does not question that HIV causes AIDS, he merely questions the most common routes of transmission in countries such as some of those in Africa in which sterility of injection apparati is sometimes questionable. Second, although there are indeed circumstances in which HIV tests will produce false positives, they are rare and there are protocols for detecting them (i.e. retesting). Third, a little scientific detective work has already shown that the Tripoli Six couldn't possibly have infected the Libyan children in question.
Now THERE'S a man who is unmistakeably NOT Andrew so I can't help but say hi to our old friend Kevin. Hi Kevin! My houses value went up three percent last year how bout yours? Not as good as twelve but heck, my oldest will be working for pharma in five or ten years so I'm still alive?
Since we've seen illegal drug use doesn't cause AIDS, something must cause it right so why not prescription drugs says Kevin. I bet almost everyone with HIV and AIDS has taken a prescription drug or a drug of abuse or been exposed to a toxic chemical sometime. Obviously chemicals cause AIDS in Kevin's toxic world. I would just worry maybe there's someone in the world with HIV and AIDS who never had drug even aspirin. That would kinda falsify things. So Kevin here's my suggestions. Theory one says everyone with HIV has a mother who's a woman. Having a woman for a mother will give you HIV! More consistent than the drug thing, right. Theory two says the real estate market causes AIDS. Follow me here. Everybody with HIV and AIDS lives where? On the LAND! Land is what? REAL ESTATE! So real estate causes HIV and AIDS. Everyone dive in the ocean!
Sorry. More seriously. CDC said in 2004 almost half of Americans were taking a prescription drug currently. As prescription drug use has gone up, life expectancy has gone up. Individual studies on specific drug says there's some causation there. For AIDS, as prescription drug use goes up, AIDS deaths go down. When they switched single to multiple therapy, massive decrease in death. Some people ARE overmed just like some people use to much bengay, thanks Tara, that was interesting. Balanced out though drugs have done alot of good things.
Gotta go. Time for my Real Estate investment seminar.
Dear Raven,
RE:
"Andrew, use of contaminated needles as a route of HIV transmission supports the HIV/AIDS theory, not removes support."
I'm hip! But not because something never isolated called "HIV" is causing it:
The hepatitis B vaccine causes false positive "HIV" test results [Lee, D, Eby W, Molinaro, G.. HIV false positivity after Hepatitis B vaccination. Lancet 339: 1060, 1992].
Flu vaccines cause "HIV" postivity about 2% of the time according to Klausner (Simonsen L, Buffington J, Shapiro CN, et al. Multiple false reactions in viral antibody screening assays after influenza vaccination. Am J Epidemiol 141:1089-1096,1995):
Christian Erickson, Todd McNiff, and Jeffrey Klausner have recently warned that influenza vaccinations generate false positive HIV results (Christian, P. Erickson,Todd McNiff, Jeffrey D. Klausner. Influenza Vaccination and False Positive HIV Results New England Journal of Medicine,Number 13 , Volume 354:1422-1423, March 30, 2006):
"A case-control study 2 of 101 blood donors [Simonson et al's study referenced above) who had been vaccinated against influenza and 191 matched controls showed that recent inoculation with any brand of influenza vaccine was significantly associated with a false positive screening assay for HIV antibodies. Guidelines of both Johns Hopkins and the New York State Department of Health list influenza vaccination as a known cause of indeterminate results on Western blotting for HIV antibodies (Reasons for false-positive, false-negative, and indeterminate results in assays for the detection of antibodies against HIV)."
How can the flu vaccine cause the human body to generate proteins that are specific to "The AIDS Virus" (A) if the proteins or nucleic acid sequences of "HIV" are unique, and as Gallo recently proclaimed, "one molecule of "HIV" couldn't be found in a stadium filled with people who were negative for the virus!"
But "HIV" is no flu virus! This is AIDS denialism, and it serves to erode confidence in the "HIV=AIDS" paradigm. If 2 of 101 flu vaccine subjects tests false positive for "HIV," then in a population of 300 million, this would exceed by 6 fold the true rate of "HIV" infection currently thought to exist in the U.S. by your computer model people at the NIH, with their hypothetical AIDS patients (currently about 1 million hypothetical people are said to be living with "HIV"). Its going to be more more and more difficult to convince flu vaccinees that they have acquired "HIV," as opposed to merely having developed a false-positive reaction to flu vaccines.
Also, it is good to know that:
"An interesting finding was the labeling of subcapsular/medullary epithelium in normal uninvoluted thymus by a number of antibodies to HIV-1 gag p17 and p24 proteins. Compatible with this labeling was the staining of epithelial stalks in hyperinvoluted thymuses irrespective of disease category. The previously reported cross-reactivity between HIV-1 core protein and thymosin alpha 1 cannot fully explain this observation, because the epithelium in the hyperinvoluted state is negative for thymosin alpha 1.
Am J Pathol. 1989 Jun;134(6):1329-38.
The thymus in acquired immune deficiency syndrome. Comparison with other types of immunodeficiency diseases, and presence of components of human immunodeficiency virus type 1.
Schuurman HJ, Krone WJ, Broekhuizen R, van Baarlen J, van Veen P, Golstein AL, Huber J, Goudsmit J.
Department of Internal Medicine University Hospital, The Netherlands.
The authors studied thymus specimens taken at autopsy from eight acquired immune deficiency syndrome (AIDS) patients and compared these with those taken from four patients with congenital immunodeficiency (unrelated to an intrinsic thymus defect) and seven patients after allogeneic bone marrow transplantation. In all cases, histology showed a severely involuted architecture, compatible with a debilitating disease before death. There were no major differences between thymus tissue in AIDS patients and in the other patients studied. This argues against the claim expressed in the literature that the epithelial microenvironment incurs particular HIV-1-induced injury in AIDS. This conclusion is substantiated by immunohistochemistry for HIV-1 gag and env proteins, and by hybridohistochemistry for gag/pol and env mRNA of HIV-1. Positive cells were observed only in low numbers, both inside the epithelial parenchyma and in the (expanded) perivascular areas. An interesting finding was the labeling of subcapsular/medullary epithelium in normal uninvoluted thymus by a number of antibodies to HIV-1 gag p17 and p24 proteins. Compatible with this labeling was the staining of epithelial stalks in hyperinvoluted thymuses irrespective of disease category. The previously reported cross-reactivity between HIV-1 core protein and thymosin alpha 1 cannot fully explain this observation, because the epithelium in the hyperinvoluted state is negative for thymosin alpha 1. This study confirms and extends previous reports on the endogenous presence of epitopes of retroviral antigens in thymic epithelium.
RE:
"Also, can you at least try to come up with something far less silly than HIV is a biomarker for drug abuse?"
Sorry Raven...I'll try harder next time. Maybe Dr. Fauci can help us out here:
As of January 1, 1997, the number of infants and children in USA diagnosed with AIDS was 6,891 and ninety percent of these cases had mothers who were drug users (Fauci A.S., Braunwald, E., Isslbacher, K.J., et al. Harrison's. Principles of Internal Medicine. (McGraw-Hill Companies, Inc. New York USA, ed. 14, 1998).
Cheers,
Andy
151 Children in South Africa were given HAART. 10 percent died shortly after starting HAART. In other words, the children were killed by HAART. How do we know that these unfortunate died from HAART drugs? After all, HAART is supposed to save AIDS patients with the Lazarus effect right? The sick are supposed to miraculously get up out of bed and walk to the door to greet the doctor. Unfortunately, the response found in these unfortunate sick kids to this miracle drug HAART cocktail was death. The sickest kids died from HAART toxicity within the first 5 months of the study. The surviving children were the healthy ones able to withstand the toxic efects of the drug cocktails.
For the lurkers: ask the question in terms of Darwin's natural selection. The sickest children (end-stage tuberculosis and gasteroenteritis) were naturally selected out by the HAART drugs, only the fittest survived.
AZT and HAART have been soundly rejected by the government of South Africa. They are correct.
"Obviously chemicals cause AIDS..." -- Adele
We finally agree on something, Adele...I realize it's only 4 little words, but it's a start. However, the bulk of your simple-minded musings is just that, bulk, and they remind me of one of my favorite Chinese proverbs:
"When a finger points at the moon, the imbecile looks at the finger."
Describes you and your position on HIV/AIDS quite nicely, I think. Someday, we'll all realize that "Yes, AIDS does indeed have multiple causes", and you wanna know what the real irony is, Adele, HIV won't make the cut...
_______________________________________
"Gotta go. Time for my Real Estate investment seminar."
I certainly wouldn't at all be surprised to learn that you are joining the "real estate frenzy" at this tragically late stage. One could even describe the real estate market in this country as having full-blown AIDS. Is that term even used, anymore? And could someone get a CD4 count, STAT!
Notwithstanding, when you're fighting off foreclosure, Adele, do promise to remember my frequent admonishment of your ignorance as a "kind" gesture to a less fortunate wit and not with the vitriol that you deserve.
Kevin
Yo Andy? You wrote How can the flu vaccine cause the human body to generate proteins that are specific to "The AIDS Virus" (A) if the proteins or nucleic acid sequences of "HIV" are unique, and as Gallo recently proclaimed, "one molecule of "HIV" couldn't be found in a stadium filled with people who were negative for the virus!"
Check out an introductory Immunology text book and look up "cross reacting antibodies". Because the proteins and the nucleic acid sequences of HIV are unique but under some circumstances some individuals can temporarily have cross reacting antibodies.
I also note, Andy, that although you cut and pasted from the Klausner one page note you failed to include this gem "In accordance with accepted screening algorithms, [1] we thus considered the patient to be HIV-negative with a high level of confidence."
I'll leave it to you to reread the paper to discover why they considered the patient to be HIV-negative.
Forty mules, you are parroting the idiocy of dog's breakfast, which I have already responded to. It is just barely possible you are not one and the same person so I will repeat:
You said:
I said:
"The Kaplan Meier (presented in Figure 3) mortality survival estimate at 12 months was 90.9% (95%CI 84.8- 94.6). Paediatric mortalities are summarized in Table 4. All 13 deaths occurred within the first 5 months of HAART initiation. No deaths were attributed to metabolic disorders or other drug-related adverse effects. Autopsy data were not available, but the most commonly reported causes of death were chronic gastroenteritis (n = 6) and TB (n = 4). Other causes of death included: sepsis syndrome (n = 1), suspected PCP (n = 1), and a respiratory tract infection (n = 1)".
So these kids died of opportunistic infections, not HAART drugs. You'd think that with the entire internet at their disposal that the HIV denialists could come up with a study that actually shows what they claim..... but no. They are incapable of finding even one."
HAART takes a few months to work. The kids who died all died within 5 months of starting HAART, because they started treatment at a very advanced stage of illness. After 5 months none died (despite what you would consider to be increasing cumulative doses of "highly toxic drugs"). Overall mortality was only 9% after a year - quite an astounding response rate for pediatric AIDS cases.
You said:
You are a little out of date. South Africa has now accepted the irrefutable proof that HAART works and has set up major upscaling projects to ensure its population can now get the drugs.
http://www.aegis.org/news/re/2007/RE070533.html
You see, even a dyed-in-the-wool denialist like Msimang can change her spots when faced with the evidence. Question is why can't you?
"President Thabo Mbeki has finally put paid to speculation about Health Minister Manto Tshabalala-Msimang's future in his cabinet, announcing that she was due to be officially back at work on Wednesday.
While her political obituary was written in some quarters and her successor openly speculated about, she has survived ill health and repeated calls for her axing, and cocked yet another snook at her detractors and those who had hoped for a cabinet shuffle." S Africa News.
Nothing has changed in South Africa. Manto was out sick with a liver transplant and is now back at work as health minister with the president's full support. She was snubbed by the AID conference and pulled out.
South Africa suffered under white rule long enough before their liberation from Aparteid. They are now free to reject or accept what they see fit. They have reexamined HIV and toxic drug treatments and rejected it. This hasn't changed since the presidental panel convened by Thabo Mbeki.
Africa needs assistance, and they are willing to humor the AIDS activists to get it.
Andrew, You sink to Perth level denialism? Pitiful.
You cite the Fauci text, replying to Raven regarding my comment...
As of January 1, 1997, the number of infants and children in USA diagnosed with AIDS was 6,891 and ninety percent of these cases had mothers who were drug users.
So lets use this to test your pet hypotheses.
The Duesberg hypothesis suggests that non drug users, men who don't have sex with other men, and individuals being treated for hemophilia shouldn't get HIV.
10% of the mothers were not drug users, they weren't men, and it is unlikely that they were all hemophiliacs (in fact, this would have been noted in the study). Therefore, the Duesberg hypothesis does not properly account for this group (although denialists will always use hand waving and claims that these mothers lied about their drug abuse).
The HIV/AIDS theory, on the other hand, does account for mothers transmitting the HIV virus vertically (mother to child) and for other routes of exposure, including drug abuse, sex with an infected partner, contaminated blood products, transplants from infected individuals, contaminated medical devices...
Furthermore, as an infectious agent, every exposure does not lead to infection, and person to person transmission can be tracked via epidemiological studies. If AIDS was due to drug abuse, there would be no such pattern to transmission. HIV testing predicts which individuals will develop AIDS, while drug abuse is only a risk factor, and not a strong predictor (despite what the denialists claim).
Of course, the denialists like sockpuppet will move the goalposts to include all drugs, which only serves to further weaken their already weak correlation. The alternative medicine types can't offer treatment backed up by evidence, but they are full of dishonest fear mongering and attacks on modern medicine.
LOL, gone from making stuff up, to babbling nonsense, to outright nonlogic.
There are a lot more than 6,891 women who use use drugs in the USA. Must be in the millions or tens of millions. So why aren't there millions of babies who end up with AIDS?
Rather simple, HIV is an infectious disease and most drug users don't have it, most of them who do, do not transmit the virus, and proper treatment around birth can prevent most of those.
Since when are these hypothetical acquired drug abuse blood markers hereditary? Got a link or any credible studies on women who acquire "blood markers" that are then suddenly hereditary. And cause AIDS in children, a disease that preHAART usually kills children within a year. PreHAART, time to onset of AIDS/death in newborns runs around 2.5 years. So what is this hypothetical, acquired but hereditable agent that causes AIDS and most of the time kills babies within a few years (untreated)? Sounds like an infectious agent doesn't it? Of course, it is HIV, the AIDS virus.
Forty mules, you say:
"Nothing has changed in South Africa. Manto was out sick with a liver transplant and is now back at work as health minister with the president's full support. She was snubbed by the AID conference and pulled out.
South Africa suffered under white rule long enough before their liberation from Aparteid. They are now free to reject or accept what they see fit. They have reexamined HIV and toxic drug treatments and rejected it. This hasn't changed since the presidental panel convened by Thabo Mbeki."
Your reading comprehension must be severely limited. You say that South Africa has rejected "toxic" drugs. Well that maybe so, but it seems that they have finally accepted HAART as being necessary for their own population and being a core element of their HIV/AIDS strategy.
From Nature, May 3rd 2007
The plan is to treat 80% of those requiring HAART by 2011.
Also see:
http://www.mg.co.za/articlepage.aspx?area=/breaking_news/breaking_news_…
http://blogs.guardian.co.uk/news/archives/2007/03/14/south_african_aids…
http://www.businessday.co.za/articles/topstories.aspx?ID=BD4A410536
Can you explain how this is "rejecting AIDS drugs?"
Even the most schizoid denialist would have a problem explaining away this obvious contradiction.
""The alternative medicine types can't offer treatment backed up by evidence, but they are full of dishonest fear mongering and attacks on modern medicine."" Robster, FCD
You claim that alternative medicine can't back up treatments with evidence, but you fail to address the main reason for that lack of evidence, namely that "alternative treatments" are not being properly studied. Perhaps, you should actually read some of the "attacks on modern medicine". The arguments being presented are so logical and so steep in common sense that such texts are generally to the point, so it shouldn't take too much effort for you to self-educate.
That said, the numerous problems with our current health care system are glariingly apparent to anyone with an ounce of common sense. I suggest you start with Overdosed America: The Broken Promise of American Medicine. It'll clear up a lot of your own confusion and denial, Robster, FCD. Incidentally, it is receiving rave reviews on Amazon like many other books on the topic and deservedly so. Whether or not you and the rest of the goon squad on this site will ever get over your own deep-seated struggles with denial, the general public is beginning to catch on to the truth of most "attacks on modern medicine" and it's not because they are gullible. To the contrary, they are just now waking up and it's about damn time!
Kevin
Yes the problems with "American medicine" are apparent to anyone who reads rave reviews on Amazon. Any of you with children probably know the "Eragon" story that's now at two books and sigh is going to hit us with another one someday. Its the worst tripe of a story I ever read sorry to anyone who likes it but a complete knock-off and boring too. I wish I could keep it from my kids because they probably lost a million brain cells just reading it. But it gets rave reviews on Amazon!
Rave reviews don't mean anything but there are real problems with helath care and Robster could tell us about a lot of them. We all have problems with health care. But don't forget as health care costs and prescription drug use has climbed so has life expectancy and quality of life.
Some people prefer to get down on all fours and graze on various therapeutic grasses. Good for them. I'll stick with my well-educated doctors thank you.
"Yes the problems with "American medicine" are apparent to anyone who reads rave reviews on Amazon. " Adele
Once again, Adele misses the point...still staring at the finger when the moon is beautiful.
One can assume that those who were inspired enough to write a review on Amazon actually READ THE BOOK, as I did (have you?). Though, I must admit that it was quite gratifying to read such reviews and to know that perhaps there is hope for a better future, even though we are currently regressing in so many areas. Regardless, it's the actual information in the book that I'm suggesting you, and your ilk, attempt to process. Of course, you're too narrow-minded and/or ignorant to understand the importance of actually reading the material that runs counter to your dogma. Just a like a fundamentalist, you and Robster and a host of others on this site have already formed an opinion about "modern medicine" that is far too fragile to endure incisive criticism. Oh the irony! It's exactly the fault that your ilk wants to ascribe to dissidents, yet the truth is that dissidents can't escape HIV/AIDS propaganda, even if we tried.
Rave reviews don't mean anything....
You really are an imbecile...it's the quality of the "reviews" that is important, just like the quality of the source material and both can vary tremendously from one work to the next, so your use of comparison . You obviously must have poor taste in a great many things, Adele, if such a simple dinstinction must be explained to you. That said, it should be noted that the author of the exceptional book that I am recommending, Overdosed America by Dr. John Abramson, teaches at Harvard Medical School, so I'm not saying that ALL doctors are ignorant shills...just the majority ;-)
But don't forget as health care costs and prescription drug use has climbed so has life expectancy and quality of life.
You keep trying to claim that our "quality of life" is so much better but the facts don't support your pollyanna. Americans make up roughly 5% of the world's population, yet we consume nearly 50% of the world's medications. That would be support for your rhetoric if we didn't rank near the bottom in virtually all health categories when compared with every other developed nation. That's a fact, Adele. All those prescriptions sure are making everyone happy, healthy and wealthy, aren't they? Or, are they just making a precious few happy...healthy...and wealthy....Read the book and then perhaps you'll be educated enough to participate in an intelligent discussion on the matter.
So what exactly is your degree in, Adele?
Propaganda?
Kevin
So, Kevin... How exactly should we study alternative medicine? Do we just throw out the rules of science that the supernatural is not a valid explanation? Is skepticism preventing the altie-meds from working?
The only fundamental that I hold fast to is this. The world can be understood without relying on supernatural cop-outs, but through careful experimentation and rational observational study. Alternative medicine rarely relies on evidence, and when it does, it either leaps to a "common sense" but invalid conclusion or demonstrates efficacy, wherein it ceases to be alternative and becomes evidence based.
I am not familiar with the book you are pushing, so I looked at it. If it comes down to a focus on prevention and public health programs, I don't have a problem with it. I'd like to see much more of a focus on prevention, as treatment is more expensive and is less effective than just not getting sick in the first place. Will it be on my reading lists? Perhaps, if I see a copy in the library or in the used book store. Right now, I have a couple evolution texts and Carl Zimmer's Parasite Rex in front of any suggestion coming from an altie.
Your reasons that we should read it, however, are specious. First, creationist and inteligunt desine books often have high ratings and rave reviews, but that doesn't mean that what they have to say is valuable regarding the progress of science. Second, citing the author's position at Harvard is an appeal to authority, a logical fallacy that suggests that the author's views should automatically be accepted without review.
All those prescriptions sure are making everyone happy, healthy and wealthy, aren't they? Or, are they just making a precious few happy...healthy...and wealthy....
False dichotomy, strawman, appeal to envy. It does, however hit on the altie bias that they should be the one making the most money. The alties are just as greedy as anybody else, and when evidence based medicine gets money and respect, it really cheeses the alties off. Some alties do manage to hit it big, with scams just as slick as any Nashville televangelist, or with a slick book and no responsibility to the "patient" beyond the cash register.
Read the book and then perhaps you'll be educated enough to participate in an intelligent discussion on the matter.
Why don't you crack open a textbook and learn something about the scientific process?
Speaking of cop-outs, our friend Robster demonstrates his limited understanding of the term with the following:
... citing the author's position at Harvard is an appeal to authority, a logical fallacy that suggests that the author's views should automatically be accepted without review.
First, let me say the I am not interested in debating your "applied logic" skills any further, but I can assure you that you chose that angle of attack in response as an opportunity to avoid actually analyzing the unflattering details about your beloved "modern medicine". Therefore, your long-winded reply was severely lacking in insight, but I guess I'll have to play along. Nevertheless, I can assure that I understand the benefits of using logic and that I have sufficient training in that area; however, I also understand the limits engaging in language games when there are more pertinent details to discuss. Perhaps, you should add some Wittgenstein to your reading list?
My mentioning of Dr. Abramson's affiliation with Harvard was entirely relevant. It would seem that he is a tenured, principled gentlemen who has reached a point in his life where being censured and/or threatened with professional sabotage is not a concern, and perhaps he is bright enough to understand the severely depraved state of our current health care system, and, futhermore, he most certainly understands the deleterious effects of our pill-popping culture of "care". You, like many of the hacks working in "science" or "medicine" today are threatened by the criticisms he raises and for good reason, because he's absolutely right. If you weren't such a toady, Robster, perhaps you could connect the dots, and I wouldn't have to waste my time explaining the significance of Dr. Abramson's harsh criticisms, particularly in light of his affiliation with a major research university.
You ask:
How exactly should we study alternative medicine?
Your question is almost as incomplete as your understanding. Of course, we don't throw out the rules of science; to the contrary, we need remove the ever-increasing obstacles being employed by greed-motivated non-scientists so that those rules can once again govern scientific inquiry. That can only be done by completely overhauling the current funding system. I don't have time right now to continue explaining the obvious, but I highly recommend you move Dr. Abramson's book up your vaunted reading list...
Kevin
Well we haven't hit bottom in idiocy but we are way past sanity here. The life span of the average American in 1900, when modern medicine was young, was 47. About the same as trash heaps like Somalia and Afghanistan.
Fast forward to 2007. The average life span of an American is now 77. An improvement of 3 decades. The evidence speaks for itself.
There is always room for improvement in anything, including medicine. One of the problems right now is demand is starting to outpace ability to pay for care. There are lots of bureaucrats and administrators who would be ecstatic if lots of people went alternative and left them alone.
Alternative has to be used with common sense. We saw a patient, picked up a primary breast tumor on a screening early from a high risk group. Prognosis at that time was 90% cure. Went alternative, 1.5 years later dead of metastatic disease at age 34. Who is to say whether she was happy with her choice, but most would have chosen differently.
Kevin, logic is important here. A person's ideas stand or fail regardless of their status, although training can be important. Andrew is clearly trained and fairly successful in cancer research, but he is clearly out of his element when it comes to HIV and AIDS. For one of the best examples of great and brilliant researchers who had nutty ideas, see Linus Pauling's vitamin C nuttery.
You, like many of the hacks working in "science" or "medicine" today are threatened by the criticisms he raises and for good reason, because he's absolutely right.
Yep. Shakin in my little booties, between his criticisms and your scare quotes.
The problems with medicine are too little prevention and too much stress on late stage treatment from medicare and HMOs, which itself acts as a feedback loop against prevention. The structure of the system needs a complete reworking. It isn't the drugs or the pharma profits that are the root problem. The root is that people choose to live unhealthful lifestyles, and the system doesn't work to change that. Of course, proper prevention would cut into the need for quite as many drugs, just one of the benefits of prevention.
If you weren't such a toady, Robster, perhaps you could connect the dots...
Really making me want to read it, Kevin.
Your question is almost as incomplete as your understanding.
So you don't have a clue.
we need remove the ever-increasing obstacles being employed by greed-motivated non-scientists so that those rules can once again govern scientific inquiry.
You really don't know how grant funds are allocated, do you? Scientists rank grant applications based on what they think the best and most attainable projects are.
That can only be done by completely overhauling the current funding system.
And sending money to alties despite a lack of evidence or even a scientifically valid explanation of how their concept might work? They already have NCCAM, and a fat lot of nothing has that bunch given us beyond proof that altie meds don't work.
After carefully reviewing some of the statements made by different people above, it seems apparent that a principal source of conflict arises from a clash between those who want to view a picture of reality through reviewing all the available data, versus those who have strong religious beliefs in the catechisms promulgated by The Church of Modern Medicine.
Let me give two examples:
Example I-Raven
RE:
"Alternative has to be used with common sense. We saw a patient, picked up a primary breast tumor on a screening early from a high risk group. Prognosis at that time was 90% cure. Went alternative, 1.5 years later dead of metastatic disease at age 34. Who is to say whether she was happy with her choice, but most would have chosen differently."
When Raven for example, (I take it that Raven is some kind of health professional with experience with cancer patients) says that a woman of 34 died of breast cancer died because she trusted alternative approaches, raven fails to include the track record or even mention of patients who receive standard chemo/radiation/ or other "standard mainstream therapies," and also die. This omission, or distortion, is probably a result of the tragedy of being aware of any 34 year old dying of cancer, but it is a gross distortion of the information that must be taken into account and not, ignored. As a medical professional, I'm sure raven is well aware of this track record, but yet, choses to support the Church's side regardless of what she/he? has probably seen with his/her own eyes.
It is generally acknowledged in the cancer community that directed and often-aggressive chemotherapies, radiation therapies, or immune therapies constitute irrational assaults on the cancer patient. Not only do these "rational," target-directed approaches not increase life expectancy in most cancer patients, they cause significant harm in the form of myelosuppression, immune dysfunction, epithelial cell destruction, nervous system stress or destruction, loss of salivation and taste in head and neck radiotherapy, burns of the skin, massive infections, and gastrointestinal collapse, castration, cachexia, and consequent mal-absorption of food, and other side-effects leading to morbidity and death. According to a recent New England Journal Of Medicine meta-analysis of Phase 1 Oncology Trials (where toxicity is typically assessed) between 1991 and 2002:
"In a survey of 460 Phase I trials of standard toxic cancer chemotherapy agents given to slightly less than 12,000 patients, the partial and complete response rates were reported to have changed from 4-5% to 10% during 1991-2002, with 3% showing a complete response, and 7% showing a partial response."
3% complete response does not mean a 3% "cure" rate, but simply, the rate of complete tumor regression, as measured by the best current methods of tumor detection during the period studied. Although the meta-analysis claimed that as many as 44.7% of patients showed some "benefit" from their therapy, and that there was a 0.5% death rate attributable to Phase I dose escalation itself, suggesting minimal overall toxicity, the "benefits" they measured were not defined and included surrogate endpoints. The data they present also must be qualified because a host of different cancer types were assessed, in which blood-borne cancers that are now more responsive than ever before to targeted therapies, heavily weighted their analysis toward the positive value of the 3% complete response rate they reported. The overall success rate of complete response is not encouraging, not to mention the fact that a cure rate is not even considered, or discussed. When discussion does occur, it is typically about the successes, as shown recently by a new target, the abl receptor, targeted by Gleevec (imatnib mesylate), although re-analyses of Gleevec's success have not looked as miraculous as before. However is should be borne in mind that this drug combats a "free-swimming" blood-borne population of tumor cells, instead of solid tumors.
A survey of oncology reviews about the toxicity and lack of efficacy of current Phase I,II, and III trials for specific cancers treated with traditional chemotherapeutic agents, radiation, and targeted immunotherapy can be obtained on a daily basis at the website of the peer-review institute at: ntkwatch@peerview-institute.org.
These clinical trial assessments show much lower response rates with solid tumors from trails aimed at specific types of cancer. For example, The European Organization for Research and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832, The World Health Organization Melanoma Program Trial 15, and the North American Perfusion Group Southwest Oncology Group-8593, in a trial of 832 melanoma patients, reported that:
"The results of this study show that regional infusion of chemotherapy to the limb in proximity to a melanoma lesion in the attempt to reduce the risk of future tumor recurrences is associated with significant adverse events, and no benefits. Eight hundred thirty-two patients were enrolled in the study; 412 underwent surgery consisting of resection of the melanoma lesion, and 420 underwent surgery followed by isolated limb perfusion with the anticancer drug melphalan plus mild hyperthermia. Progression of disease and overall survival did not differ between the two groups. Toxicity (including two limb amputations) occurred significantly more often in patients who underwent chemotherapy compared to those who did not. These data do not support the use of adjuvant chemotherapy in the management of patients with early cancer" [Prophylactic isolated limb perfusion for localized, high-risk limb melanoma Results of a multicenter randomized phase III trial. European Organization for Research and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832 The World Health Organization Melanoma Program Trial 15, and the North American Perfusion Group Southwest Oncology Group-8593. Koops HS; et al. J Clin Oncol, 16(9):2906-12 1998 Sep].
In a different kind of prospective randomized trial of the treatment of patients with metastatic melanoma using chemotherapy with cisplatin, dacarbazine, and tamoxifen alone or in combination with interleukin-2 and interferon alfa-2b, it was reported recently that:
"This was a randomized study to determine whether the addition of immunotherapy to chemotherapy results in better tumor control in patients with advanced melanoma. One hundred-two patients were enrolled; 52 patients received chemotherapy only, and 50 patients received chemotherapy plus immunotherapy (interferon alpha and interleukin-2). Although tumor responses were observed more frequently in the chemo-immunotherapy group (44% vs. 27%), this group also experienced higher treatment-related toxicity and showed a trend of decreased survival. Both regimens produced tumor responses that were only partial and short lasting" [Prospective randomized trial of the treatment of patients with metastatic melanoma using chemotherapy with cisplatin, dacarbazine, and tamoxifen alone or in combination with interleukin-2 and interferon alfa-2b. Rosenberg SA, et al. J Clin Oncol, 17(3):968-75 1999 Mar].
These outcomes, although bleak for the cancer patient, are as problematic for the cancer survivor. An Institute of Medicine report was recently released calling for a paradigm shift regarding how cancer patients are managed over the long term, and asking for ways to reduce the toxicity and often morbid long-term side effects of conventional chemotherapies and radiation. (Institute of Medicine Report: Cancer Survivorship: Improving Care and Quality of Life, November 7, 2005; http://www.iom.edu/report.asp?id=30869).
"Some 10 million Americans are now cancer survivors. Large numbers are living longer than ever because of remarkable advances in early detection and treatment. But many survivors receive less than optimal follow-up, and improvements in care are necessary, the Institute of Medicine, part of the National Academies of Science, advised in a major report released Monday, November 7, 2005".
As presented in the Chicago Tribune:
"The negative consequences of cancer and its treatments are substantial and under-appreciated," said Dr. Sheldon Greenfield, panel chairman and director of the center for health policy research at the University of California, Irvine. "Many [patients] suffer permanent and disabling symptoms that impair normal functioning ... [but] there is much that can be done to avoid, ameliorate or arrest these late effects."
"The Institute of Medicine study, which focuses on adult cancer survivors, highlights a profound shift in thinking about this once-deadly disease. Until recently, researchers and clinicians had one goal: saving more lives. With improved survival rates, however, cancer increasingly is being viewed as a chronic illness like diabetes or hypertension, presenting a new set of challenges."
"Some are medical. The very toxic therapies that assault tumors and help save lives put patients at risk of new problems down the road, including second cancers, heart disease, sexual dysfunction, cognitive impairment, infertility, and chronic inflammation, research shows. For any given patient, experts note, the risk of long-term complications depends on the type and location of the cancer, the nature and duration of treatment and other factors."
"For instance, women with breast cancer who receive chest radiation therapy are at risk of developing lung cancer later, according to research cited in the report. Chemotherapy using agents known as anthracyclines increases the odds of contracting leukemia. And tamoxifen, a commonly used therapy for women with estrogen receptor-positive tumors, increases the risk of stroke, blood clots, and endometrial cancer."
Nevertheless, a survey of the FDA's list of approved drugs entering mainstream cancer chemotherapy clearly reveals a tendency to repeat the failures of the past. The FDA granted marketing applications to 71 oncology applications between January 1, 1990, and November 1, 2002 [Johnson R. Williams G, Pazdur R. End points and United States Food and Drug Administration approval of Oncology Drugs. Journal of Clinical Oncology, Vol 21, No 7, 2003: pp 1404-1411]. New additions to the FDA lists include cytotoxic drugs, monoclonal antibodies that have no efficacy and significant toxicity, immune-modulating drugs that oxidize cells and cause severe morbidity, and, a plethora of accessory drugs to boost erythrocyte production or T-cell production, anti-diarrhea medications, or medications to correct the myriad of complications due to the current toxic regimens the patient experiences due to toxicity.
It is truly surprising that despite these kinds of results from studies that directly target tumors (and these examples are representative of hundreds of similar trials not discussed here), new ideas or strategies that could potentially combat cancer more effectively and less toxically, are seldom given a chance, or are suppressed. When new approaches or treatments are permitted a phase I trial, it is only after a targeted drugging, radiation, or targeted immunotherapy campaign has failed numerous times, and after the patient is considered "terminal." In this context, how can new rational approaches be scientifically tested? How can new rational therapies begin to accrue toxicity and efficacy (or non-efficacy data) after a patient's immune system has been assaulted numerous times, and when the disease has advanced to the point where death is imminent?
At least the oncology community gives their cancer patients breaks from DNA chain terminating drugs like AZT (which was designed to treat cancers but didn't work because of its toxicity and inefficacy, instead of brow beating them like the AIDS establishment does "HIV/AIDS" patients, by telling them they are irresponsible, or doomed if they so much as even consider taking a drug holiday to allow their bone marrow, digestive system, and immune system to recover.
Example II. Robster
RE:
"Reading comprehension. Try it. Also, no "normal rules of infectious disease" are "suspended." This is yet another lie from the denialists, and is an argument from incredulity/ ignorance.
When Robster, for example says that "the denialists" cry that "the normal rules of infectious diseases are suspended (in the case of "HIV/AIDS") using incredulous arguments and ignorance (I gather he teaches students at the college level somewhere), it becomes crystal clear through his language that Robster feels that an end is justified by the means even if it means he must distort or manufacture information in order to demonstrate his piety before The Church's alter.
E.G.:
"From the initial description of Poliomyelitus in 1840 (Andrew: Polio existed before this year), to the isolation of the poliovirus in 1908, the development of the first workable Polio vaccine wasn't produced for mass use until 1955."
This statement, for instance, is meant to excuse the failure of the 30-80 "HIV" vaccines that have failed, and I stress, failed (not to prevent a single AIDS case) to demonstrate evidence of humoral, cellular, or mucosal immunity, or even to stimulate T-cells, casting doubt on any claim that what has been "isolated" and called "HIV" components in those 30-80 failed vaccines derive from an exogenous virus, that has on the other hand, supposedly induced humoral, cellular, mucosal immunity, and T-cell responses in those 50 million hypothetical persons claimed to test "HIV" positive on ELISA's WB's, or PCR.
'
Instead the polio example is given as glib assurance that although it is hard to make vaccines (may take over 50 years), but finally it was "the great success story of all time, other facts are omitted, presumably not maliciously (after all, Robster, or whatever his name really is, is a teacher who is trying to educate students), but intentionally to pay homage to The Church and its teachings. For instance, although Simon Flexner at Rockafeller is credited to having "isolated" polio in the first decade of the 1900's, what he "isolated' he thought was spread through breathing, instead of feces. Then there was the great polio epidemic in 1916 where all public policy programs regarding "the healthy carrier state" became implemented in quarantines, and prevention of all children under 15 to attend movie theatres or carnivals that summer, etc. The author Paul De Kruif himself (Microbe Hunters) was trying to convince FDR before WWII to invest in public health programs emphasizing nutrition, instead of spending all the money on bombs, planes, and war, to no avail. Polio, and the way it is spread, still isn't understood. There is some clear cut issues that Robster, if not hypnotized by The Church's power, may relate as a basis for his beliefs that the "HIV" vaccine will eventually work.
1950 (September) Ralph R. Scobey, M.D., president of the Poliomyelitis Research Institute. Inc. Syracuse, New York (Archives of Pediatrics, Sept. 1950) lists 170 diseases of polio-like symptoms and effects but with different names such as: epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, and others. There are also such common nutritional deficiency diseases as beriberi, scurvy, Asiatic plague, pellagra, prison edema, acidosis, and others. "No drugs, medicines or medical treatments have ever been able to cure any of these diseases and no germs have been isolated as the cause. But they all respond to fasting, cleansing, proper diet and improved circulation. The similarity of these diseases to polio is too obvious to go unnoticed. They are, in reality, all one disease with varying stages of intensity and different names. It is ridiculous to assume that polio is caused by a virus and the rest of them are caused by nutritional deficiency. Inasmuch as nerve cells react in much the same way to various poisons, further research will probably show that in these cases polio micro-organisms are not always present, but intoxication (poisoning) may be produced through faulty metabolism or by the absorption of poisons from without" (Ralph Scobey, 1950).
1951 The man who became most responsible for the view that poliomyelitis was contagious was Dr. Simon Flexner, author of the famous (or infamous) Flexner Report, which led the way to the closing of the naturopathic and homeopathic colleges in the United States. Said Flexner: "It was not easy to establish in an individual case precisely how the disease was acquired; it was difficult to bring evidence that was not at all convincing that this disease was contagious." In discussing Flexner's report, L. Emmett Holt stated: "Even five years ago, if anyone had suggested that the disease under discussion was an infectious or contagious one, it would have been looked upon as a
joke" (Scobey, Archives of Pediatrics, May 1951).
1953 Dr. Kumm was appointed Director of Research of the National Foundation for Infantile Paralysis (NFIP). The NFIP was funded by its "March of Dimes" program, and it sponsored the hasty development of the Salk vaccine in the early 1950s, at the height of the DDT/polio controversy. Dr. Kumm also "served as a civilian consultant to the Surgeon General . . . directing field studies of the use of DDT. . ." (American Journal of
Digestive Diseases, 20:330, 1953).
1955 IPV (inactivated polio vaccine) licensed (was later modified in 1987).
1955 On April 24, 1955, an infant with paralytic poliomyelitis was admitted to Michael Reese Hospital in Chicago, Illinois. The patient had been inoculated in the buttock with Cutter vaccine on April 16, and developed flaccid paralysis of both legs on April 24.
1955 (May)"With the announcement that Cutter was withdrawing its vaccine, there ensued a nationwide panic. The AMA put out the warning to all its members to stop using Cutter vaccine, although regrettably some doctors never received word. Many states and cities announced immediate cessation of mass immunizations, even though their vaccine had come from manufacturers other than Cutter. Local health departments began to track down every single dose of Cutter vaccine, which, it was soon discovered, had traversed the entire country. Throughout May and June, cases of polio caused by Cutter's vaccine spread beyond the Far West and began to appear in every region of the country. The epicenter of the devastation was in California and the rural state of Idaho. Ninety-nine cases of polio would eventually be attributed to Cutter vaccine in California, with the incidence of polio among Cutter vaccinees exceeding the textbook definition of a wild polio epidemic by nearly threefold. In Idaho, with eighty-eight polio cases attributed to Cutter vaccine, the rate was fifteen times greater. Before it was over, the 'Cutter incident,' as it was euphemistically called in scientific circles, resulted in 260 people contracting polio and almost 200 cases of paralysis. Eleven people died. A devastating epidemic had been caused by two particularly bad batches of vaccine" (The Virus and The Vaccine-The True Story Of A Cancer -Causing Monkey Virus-Contaminated Polio Vaccine, And the Millions Of Americans Exposed, by Debbie Bookchin and Jim Schumacher, St. Martin's Press, 2004).
1956 Dr. Albert Sabin tests experimental polio vaccine on 133 prisoners in Ohio.
1957 "Canada suspended its distribution of Salk's vaccine. By November all European countries had suspended distribution plans, apart from Denmark. By January 1957,
17 US states had stopped distributing the vaccine. The same year The New York Times reported that nearly 50 per cent of cases of infantile paralysis in children between the ages of five and 14 had occurred after vaccination" (Bookchin and Schumacker, 2004).
1961 OPV (oral, live-virus Salk polio vaccine) licensed.
1961 "Merck stopped shipping Purivax (its 'purified' version of the Salk vaccine) as soon as its own tests in May 1961 confirmed that the vaccine was contaminated with SV 40... Its unilateral withdrawal of vaccine from the market had not been well received by the DBS (Division of Biological Standards). If Merck recalled vaccine, then everyone else would have to. That would have resulted in public panic and would have run counter to the Technical Committee's May 18 directive that polio vaccination 'continue to be pursued with vigor with the materials presently available.' In June, after the Girardi cancer results had come in, Hilleman (Merck's science director) had tried one more time to get all vaccine production halted. That suggestion was rebuffed. Merck had already suspended production and was trying to figure out how to screen SV40 out of the vaccine when DBS tests on vaccine samples indicated that Parke-Davis supplies were also badly
contaminated. Parke-Davis now also stopped vaccine manufacture. The truth
was that by the time the Associated Press reported the 'news' in late July, both companies had not produced vaccine for several weeks. Parke Davis eventually resumed production, but Merck would soon decide that producing a polio vaccine that at times might be contaminated was not worth the risk." (Bookchin and Schumacker, 2004).
1962 "The Wistar human tissue study appeared in midsummer 1962, shortly before the human tissue study that Enders had completed at Hilleman's urging. Enders and his collaborator, another Harvard researcher, Harvey Shein, reached essentially the same conclusions as the Wistar group, with a different kind of tissue, human kidney cells. Koprowski had rushed the Wistar study into press hoping to scoop Enders and gain some publicity for Wistar. But in the end, despite being second, the Enders study attracted a good deal more attention because it was published in the prestigious Proceedings of the National Academy of Sciences. A lengthy New York Times story on August 10, 1962, reported the Enders study:
'A cancer-causing virus has for the first time produced cancer like changes in human cells... Changes that the virus produced in cultures of human kidney cells included greatly accelerated growth patterns and chromosomal aberrations...'
"By the fall of 1962, as news of the most recent SV40 research spread, the anxiety that had been growing in scientific circles about the simian virus rearched its zenith. 'It was the worst thing in the world,' Hayflick recalls of the news. 'Please tell me: What else could we find worse in monkey kidney cells?' In Britain, Wellcome Laboratories decided to stop inactivated vaccine production and switch entirely to live polio vaccine production."
"As in the United States, however, both the British and Canadian governments decided not to recall old stocks of Salk vaccine. Britain had a surplus of 6 million injections in 1961. In Sweden, the concern was about Sabin-type vaccine. There were plans to give monkey gamma globulin to four thousand children who had received oral vaccine in the belief that it would contain antibodies against any simian viruses, including SV40, which might have contaminated the oral doses. In the Soviet Union, site of the most extensive use of Sabin's vaccine, tests were conducted to determine the spread of SV40. Many of the technicians and scientists involved in Chumakov's massive vaccination trial proved to have been infected by the virus, and the Soviets were now fearful of SV40's possible
long-term effects. Among American research and health officials, a joke with gallows-type humor began to make the rounds: The Soviets would lose the 1964 Olympics because their athletes would all have tumors thanks to SV40" (Bookchin and Schumacker, 2004).
1972 Jonas Salk, inventor of the IPV, testified before a Senate subcommittee that nearly all polio outbreaks since 1961 were caused by the oral polio vaccine.
1992 America's Centers for Disease Control (CDC) in Atlanta admits in that the polio live-virus vaccine had become the main cause of polio in the United States. Specifically, the CDC asserted that, from 1973 to 1983, 87% of all (non-imported) cases of polio resulted directly from vaccine administration. Even more amazingly, it was asserted that every non-imported case of polio in the United States from 1980 to 1989 was vaccine-induced (Strebel, P. M., et al., Epidemiology of Poliomyelitis in the U.S. One Decade after the Last Reported Case of Indigenous Wild Virus Associated Disease, Clinical Infectious Diseases, CDC, February 1992, pp. 568-579).
1997 Polio is not eradicated by vaccination, but likely lurks behind a disease redefinition and new diagnostic names like viral or aseptic meningitis.......According to one of the 1997 issues of the MMWR, there are some 30,000 to 50,000 cases of viral meningitis per year in the United States alone. That's where it is thought that 30,000 - 50,000 cases of polio disappeared after the introduction of mass vaccination.
"Today, various other forms of the word "polio" are still used to describe the effects of poisoning, though usually with regard to paralysis in animals. A search of Medline ("polio" and "poison") finds about 45 contemporary articles where poisoning causality is attributed to polio. The terminology found was: "polioencephalomalacia", "poliomyelomalacia", "polyradiculoneuritis", "neurological picture similar to that of poliomyelitis", "polioencephalomyelomalacia", "lumbal poliomyelomalacia", "cerebrocortical necrosis (polioencephalomalacia)", "Lead poisoning in grey-headed fruit bats (Pteropus poliocephalus)", "multifocal-poliomyelomalacia", "spinal poliomalacia", "Polio and high-sulfate diets", "atypical porcine enterovirus encephalomyelitis: possible interraction between enteroviruses and arsenicals", "polioencephalomalacia and photosensitization associated with kochia scoparia consumption in range cattle", "bovine polioencephalomalacia." Viral or aseptic meningitis, Guillaine Barre Syndrome (GBS), Chinese paralytic syndrome, chronic fatigue syndrome, epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, ME, post-polio syndrome, acute flaccid paralysis (Jim West, Health and Research Publications, http://www.geocities.com/harpub/).
2002 Figures from the US Centers for Disease Control and Prevention showed there were 1,920 confirmed cases of polio reported by laboratories in 2002, up from 483 the previous year.
2004 (February) West Africa polio campaign is boycotted by Nigerian states.
A mass poliomyelitis vaccination campaign got under way to immunise 63 million children across west Africa but was boycotted by four predominantly Muslim states in Nigeria, where leaders claim the oral vaccine causes sterility and spreads AIDS BMJ (328:485 2004). The west African campaign was intended as a final push to stamp out the disease in the region and is part of the World Health Organization's 15 year drive to halt transmission of the poliomyelitis virus across the world by 2005. According to Dr Haruna Kaita, the head of the medical team that conducted the test in India, the vaccines contain "undeclared contaminants that can cause malfunctioning of the testes and cause infertility in women." The team also found "some toxic substances."
"Polio controversy started long ago," said Dr Kaita. "If you find one batch defective, you should condemn all batches. What these people [proponents of the vaccine] are saying is unethical, illegal, and criminal, and they know that these things are contaminated and they have the potential to cause human hazards. They should be banned rather than cause diseases in innocent children."
2006 (April) Associated press releases article claiming that Bangladesh will vaccinate about 18 million children aged 5 and under to combat polio, which recently re-emerged after authorities believed it had been eradicated five years ago, the country's health minister said Saturday. Bangladesh carried out extensive vaccination programs in 1995-2004, with the last polio case reported in August 2000, according to the government and WHO.
2006 (Sept 1) Polio reported on the rise in Nigeria Lagos, Nigeria despite near-universal vaccination. Nigerian authorities on Friday reported a sharp rise in the number of polio cases in Africa's most populous country over recent months, despite a government immunization drive.
"A total of 784 cases of the disease were registered in 17 states at the end of July, the National Programme on Immunisation said. In June the figures were 501 cases in 15 states, compared to 244 cases in 18 states for the same period in 2005, it said in a statement."
"From June 29 to July 3, Nigerian health officials in collaboration with United Nations health agencies launched an ambitious five-day Polio Plus immunization campaign of 10-million children in northern Nigeria aimed at eradicating the deadly disease from the country by the end of 2006."
2006 (December) Despite the 2004-5 west African polio eradication campaign intended as a final push to stamp out the disease in the region and is part of the World Health Organization's 15 year drive to halt transmission of the poliomyelitis virus across the world by 2005, the CDC, and WHO report that Nigeria now leads the world in new polio cases http://www.who.int/vaccines/immunization_monitoring/en/diseases/poliomy….
-Country: Nigeria
-Year: 2006
-AFP cases (acute flaccid paralysis) reported: 4937
-Non-polio AFP rate:6.7%
-AFP rate with adequate specimens: 88
-Total confirmed polio cases: 1044
-Wild-virus confirmed polio cases: 1043
-Polio cases attributed to vaccine: 9
After carefully reviewing some of the statements made by different people above, it seems apparent that a principal source of conflict arises from a clash between those who want to view a picture of reality through reviewing all the available data, versus those who have strong religious beliefs in the catechisms promulgated by The Church of Modern Medicine.
Let me give two examples:
Example I-Raven
RE:
"Alternative has to be used with common sense. We saw a patient, picked up a primary breast tumor on a screening early from a high risk group. Prognosis at that time was 90% cure. Went alternative, 1.5 years later dead of metastatic disease at age 34. Who is to say whether she was happy with her choice, but most would have chosen differently."
When Raven for example, (I take it that Raven is some kind of health professional with experience with cancer patients) says that a woman of 34 died of breast cancer died because she trusted alternative approaches, raven fails to include the track record or even mention of patients who receive standard chemo/radiation/ or other "standard mainstream therapies," and also die. This omission, or distortion, is probably a result of the tragedy of being aware of any 34 year old dying of cancer, but it is a gross distortion of the information that must be taken into account and not, ignored. As a medical professional, I'm sure raven is well aware of this track record, but yet, choses to support the Church's side regardless of what she/he? has probably seen with his/her own eyes.
It is generally acknowledged in the cancer community that directed and often-aggressive chemotherapies, radiation therapies, or immune therapies constitute irrational assaults on the cancer patient. Not only do these "rational," target-directed approaches not increase life expectancy in most cancer patients, they cause significant harm in the form of myelosuppression, immune dysfunction, epithelial cell destruction, nervous system stress or destruction, loss of salivation and taste in head and neck radiotherapy, burns of the skin, massive infections, and gastrointestinal collapse, castration, cachexia, and consequent mal-absorption of food, and other side-effects leading to morbidity and death. According to a recent New England Journal Of Medicine meta-analysis of Phase 1 Oncology Trials (where toxicity is typically assessed) between 1991 and 2002:
"In a survey of 460 Phase I trials of standard toxic cancer chemotherapy agents given to slightly less than 12,000 patients, the partial and complete response rates were reported to have changed from 4-5% to 10% during 1991-2002, with 3% showing a complete response, and 7% showing a partial response."
3% complete response does not mean a 3% "cure" rate, but simply, the rate of complete tumor regression, as measured by the best current methods of tumor detection during the period studied. Although the meta-analysis claimed that as many as 44.7% of patients showed some "benefit" from their therapy, and that there was a 0.5% death rate attributable to Phase I dose escalation itself, suggesting minimal overall toxicity, the "benefits" they measured were not defined and included surrogate endpoints. The data they present also must be qualified because a host of different cancer types were assessed, in which blood-borne cancers that are now more responsive than ever before to targeted therapies, heavily weighted their analysis toward the positive value of the 3% complete response rate they reported. The overall success rate of complete response is not encouraging, not to mention the fact that a cure rate is not even considered, or discussed. When discussion does occur, it is typically about the successes, as shown recently by a new target, the abl receptor, targeted by Gleevec (imatnib mesylate), although re-analyses of Gleevec's success have not looked as miraculous as before. However is should be borne in mind that this drug combats a "free-swimming" blood-borne population of tumor cells, instead of solid tumors.
A survey of oncology reviews about the toxicity and lack of efficacy of current Phase I,II, and III trials for specific cancers treated with traditional chemotherapeutic agents, radiation, and targeted immunotherapy can be obtained on a daily basis at the website of the peer-review institute at: ntkwatch@peerview-institute.org.
These clinical trial assessments show much lower response rates with solid tumors from trails aimed at specific types of cancer. For example, The European Organization for Research and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832, The World Health Organization Melanoma Program Trial 15, and the North American Perfusion Group Southwest Oncology Group-8593, in a trial of 832 melanoma patients, reported that:
"The results of this study show that regional infusion of chemotherapy to the limb in proximity to a melanoma lesion in the attempt to reduce the risk of future tumor recurrences is associated with significant adverse events, and no benefits. Eight hundred thirty-two patients were enrolled in the study; 412 underwent surgery consisting of resection of the melanoma lesion, and 420 underwent surgery followed by isolated limb perfusion with the anticancer drug melphalan plus mild hyperthermia. Progression of disease and overall survival did not differ between the two groups. Toxicity (including two limb amputations) occurred significantly more often in patients who underwent chemotherapy compared to those who did not. These data do not support the use of adjuvant chemotherapy in the management of patients with early cancer" [Prophylactic isolated limb perfusion for localized, high-risk limb melanoma Results of a multicenter randomized phase III trial. European Organization for Research and Treatment of Cancer Malignant Melanoma Cooperative Group Protocol 18832 The World Health Organization Melanoma Program Trial 15, and the North American Perfusion Group Southwest Oncology Group-8593. Koops HS; et al. J Clin Oncol, 16(9):2906-12 1998 Sep].
In a different kind of prospective randomized trial of the treatment of patients with metastatic melanoma using chemotherapy with cisplatin, dacarbazine, and tamoxifen alone or in combination with interleukin-2 and interferon alfa-2b, it was reported recently that:
"This was a randomized study to determine whether the addition of immunotherapy to chemotherapy results in better tumor control in patients with advanced melanoma. One hundred-two patients were enrolled; 52 patients received chemotherapy only, and 50 patients received chemotherapy plus immunotherapy (interferon alpha and interleukin-2). Although tumor responses were observed more frequently in the chemo-immunotherapy group (44% vs. 27%), this group also experienced higher treatment-related toxicity and showed a trend of decreased survival. Both regimens produced tumor responses that were only partial and short lasting" [Prospective randomized trial of the treatment of patients with metastatic melanoma using chemotherapy with cisplatin, dacarbazine, and tamoxifen alone or in combination with interleukin-2 and interferon alfa-2b. Rosenberg SA, et al. J Clin Oncol, 17(3):968-75 1999 Mar].
These outcomes, although bleak for the cancer patient, are as problematic for the cancer survivor. An Institute of Medicine report was recently released calling for a paradigm shift regarding how cancer patients are managed over the long term, and asking for ways to reduce the toxicity and often morbid long-term side effects of conventional chemotherapies and radiation. (Institute of Medicine Report: Cancer Survivorship: Improving Care and Quality of Life, November 7, 2005; http://www.iom.edu/report.asp?id=30869).
"Some 10 million Americans are now cancer survivors. Large numbers are living longer than ever because of remarkable advances in early detection and treatment. But many survivors receive less than optimal follow-up, and improvements in care are necessary, the Institute of Medicine, part of the National Academies of Science, advised in a major report released Monday, November 7, 2005".
As presented in the Chicago Tribune:
"The negative consequences of cancer and its treatments are substantial and under-appreciated," said Dr. Sheldon Greenfield, panel chairman and director of the center for health policy research at the University of California, Irvine. "Many [patients] suffer permanent and disabling symptoms that impair normal functioning ... [but] there is much that can be done to avoid, ameliorate or arrest these late effects."
"The Institute of Medicine study, which focuses on adult cancer survivors, highlights a profound shift in thinking about this once-deadly disease. Until recently, researchers and clinicians had one goal: saving more lives. With improved survival rates, however, cancer increasingly is being viewed as a chronic illness like diabetes or hypertension, presenting a new set of challenges."
"Some are medical. The very toxic therapies that assault tumors and help save lives put patients at risk of new problems down the road, including second cancers, heart disease, sexual dysfunction, cognitive impairment, infertility, and chronic inflammation, research shows. For any given patient, experts note, the risk of long-term complications depends on the type and location of the cancer, the nature and duration of treatment and other factors."
"For instance, women with breast cancer who receive chest radiation therapy are at risk of developing lung cancer later, according to research cited in the report. Chemotherapy using agents known as anthracyclines increases the odds of contracting leukemia. And tamoxifen, a commonly used therapy for women with estrogen receptor-positive tumors, increases the risk of stroke, blood clots, and endometrial cancer."
Nevertheless, a survey of the FDA's list of approved drugs entering mainstream cancer chemotherapy clearly reveals a tendency to repeat the failures of the past. The FDA granted marketing applications to 71 oncology applications between January 1, 1990, and November 1, 2002 [Johnson R. Williams G, Pazdur R. End points and United States Food and Drug Administration approval of Oncology Drugs. Journal of Clinical Oncology, Vol 21, No 7, 2003: pp 1404-1411]. New additions to the FDA lists include cytotoxic drugs, monoclonal antibodies that have no efficacy and significant toxicity, immune-modulating drugs that oxidize cells and cause severe morbidity, and, a plethora of accessory drugs to boost erythrocyte production or T-cell production, anti-diarrhea medications, or medications to correct the myriad of complications due to the current toxic regimens the patient experiences due to toxicity.
It is truly surprising that despite these kinds of results from studies that directly target tumors (and these examples are representative of hundreds of similar trials not discussed here), new ideas or strategies that could potentially combat cancer more effectively and less toxically, are seldom given a chance, or are suppressed. When new approaches or treatments are permitted a phase I trial, it is only after a targeted drugging, radiation, or targeted immunotherapy campaign has failed numerous times, and after the patient is considered "terminal." In this context, how can new rational approaches be scientifically tested? How can new rational therapies begin to accrue toxicity and efficacy (or non-efficacy data) after a patient's immune system has been assaulted numerous times, and when the disease has advanced to the point where death is imminent?
At least the oncology community gives their cancer patients breaks from DNA chain terminating drugs like AZT (which was designed to treat cancers but didn't work because of its toxicity and inefficacy, instead of brow beating them like the AIDS establishment does "HIV/AIDS" patients, by telling them they are irresponsible, or doomed if they so much as even consider taking a drug holiday to allow their bone marrow, digestive system, and immune system to recover.
Example II. Robster
RE:
"Reading comprehension. Try it. Also, no "normal rules of infectious disease" are "suspended." This is yet another lie from the denialists, and is an argument from incredulity/ ignorance.
When Robster, for example says that "the denialists" cry that "the normal rules of infectious diseases are suspended (in the case of "HIV/AIDS") using incredulous arguments and ignorance (I gather he teaches students at the college level somewhere), it becomes crystal clear through his language that Robster feels that an end is justified by the means even if it means he must distort or manufacture information in order to demonstrate his piety before The Church's alter.
E.G.:
"From the initial description of Poliomyelitus in 1840 (Andrew: Polio existed before this year), to the isolation of the poliovirus in 1908, the development of the first workable Polio vaccine wasn't produced for mass use until 1955."
This statement, for instance, is meant to excuse the failure of the 30-80 "HIV" vaccines that have failed, and I stress, failed (not to prevent a single AIDS case) to demonstrate evidence of humoral, cellular, or mucosal immunity, or even to stimulate T-cells, casting doubt on any claim that what has been "isolated" and called "HIV" components in those 30-80 failed vaccines derive from an exogenous virus, that has on the other hand, supposedly induced humoral, cellular, mucosal immunity, and T-cell responses in those 50 million hypothetical persons claimed to test "HIV" positive on ELISA's WB's, or PCR.
'
Instead the polio example is given as glib assurance that although it is hard to make vaccines (may take over 50 years), but finally it was "the great success story of all time, other facts are omitted, presumably not maliciously (after all, Robster, or whatever his name really is, is a teacher who is trying to educate students), but intentionally to pay homage to The Church and its teachings. For instance, although Simon Flexner at Rockafeller is credited to having "isolated" polio in the first decade of the 1900's, what he "isolated' he thought was spread through breathing, instead of feces. Then there was the great polio epidemic in 1916 where all public policy programs regarding "the healthy carrier state" became implemented in quarantines, and prevention of all children under 15 to attend movie theatres or carnivals that summer, etc. The author Paul De Kruif himself (Microbe Hunters) was trying to convince FDR before WWII to invest in public health programs emphasizing nutrition, instead of spending all the money on bombs, planes, and war, to no avail. Polio, and the way it is spread, still isn't understood. There is some clear cut issues that Robster, if not hypnotized by The Church's power, may relate as a basis for his beliefs that the "HIV" vaccine will eventually work.
1950 (September) Ralph R. Scobey, M.D., president of the Poliomyelitis Research Institute. Inc. Syracuse, New York (Archives of Pediatrics, Sept. 1950) lists 170 diseases of polio-like symptoms and effects but with different names such as: epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, and others. There are also such common nutritional deficiency diseases as beriberi, scurvy, Asiatic plague, pellagra, prison edema, acidosis, and others. "No drugs, medicines or medical treatments have ever been able to cure any of these diseases and no germs have been isolated as the cause. But they all respond to fasting, cleansing, proper diet and improved circulation. The similarity of these diseases to polio is too obvious to go unnoticed. They are, in reality, all one disease with varying stages of intensity and different names. It is ridiculous to assume that polio is caused by a virus and the rest of them are caused by nutritional deficiency. Inasmuch as nerve cells react in much the same way to various poisons, further research will probably show that in these cases polio micro-organisms are not always present, but intoxication (poisoning) may be produced through faulty metabolism or by the absorption of poisons from without" (Ralph Scobey, 1950).
1951 The man who became most responsible for the view that poliomyelitis was contagious was Dr. Simon Flexner, author of the famous (or infamous) Flexner Report, which led the way to the closing of the naturopathic and homeopathic colleges in the United States. Said Flexner: "It was not easy to establish in an individual case precisely how the disease was acquired; it was difficult to bring evidence that was not at all convincing that this disease was contagious." In discussing Flexner's report, L. Emmett Holt stated: "Even five years ago, if anyone had suggested that the disease under discussion was an infectious or contagious one, it would have been looked upon as a
joke" (Scobey, Archives of Pediatrics, May 1951).
1953 Dr. Kumm was appointed Director of Research of the National Foundation for Infantile Paralysis (NFIP). The NFIP was funded by its "March of Dimes" program, and it sponsored the hasty development of the Salk vaccine in the early 1950s, at the height of the DDT/polio controversy. Dr. Kumm also "served as a civilian consultant to the Surgeon General . . . directing field studies of the use of DDT. . ." (American Journal of
Digestive Diseases, 20:330, 1953).
1955 IPV (inactivated polio vaccine) licensed (was later modified in 1987).
1955 On April 24, 1955, an infant with paralytic poliomyelitis was admitted to Michael Reese Hospital in Chicago, Illinois. The patient had been inoculated in the buttock with Cutter vaccine on April 16, and developed flaccid paralysis of both legs on April 24.
1955 (May)"With the announcement that Cutter was withdrawing its vaccine, there ensued a nationwide panic. The AMA put out the warning to all its members to stop using Cutter vaccine, although regrettably some doctors never received word. Many states and cities announced immediate cessation of mass immunizations, even though their vaccine had come from manufacturers other than Cutter. Local health departments began to track down every single dose of Cutter vaccine, which, it was soon discovered, had traversed the entire country. Throughout May and June, cases of polio caused by Cutter's vaccine spread beyond the Far West and began to appear in every region of the country. The epicenter of the devastation was in California and the rural state of Idaho. Ninety-nine cases of polio would eventually be attributed to Cutter vaccine in California, with the incidence of polio among Cutter vaccinees exceeding the textbook definition of a wild polio epidemic by nearly threefold. In Idaho, with eighty-eight polio cases attributed to Cutter vaccine, the rate was fifteen times greater. Before it was over, the 'Cutter incident,' as it was euphemistically called in scientific circles, resulted in 260 people contracting polio and almost 200 cases of paralysis. Eleven people died. A devastating epidemic had been caused by two particularly bad batches of vaccine" (The Virus and The Vaccine-The True Story Of A Cancer -Causing Monkey Virus-Contaminated Polio Vaccine, And the Millions Of Americans Exposed, by Debbie Bookchin and Jim Schumacher, St. Martin's Press, 2004).
1956 Dr. Albert Sabin tests experimental polio vaccine on 133 prisoners in Ohio.
1957 "Canada suspended its distribution of Salk's vaccine. By November all European countries had suspended distribution plans, apart from Denmark. By January 1957,
17 US states had stopped distributing the vaccine. The same year The New York Times reported that nearly 50 per cent of cases of infantile paralysis in children between the ages of five and 14 had occurred after vaccination" (Bookchin and Schumacker, 2004).
1961 OPV (oral, live-virus Salk polio vaccine) licensed.
1961 "Merck stopped shipping Purivax (its 'purified' version of the Salk vaccine) as soon as its own tests in May 1961 confirmed that the vaccine was contaminated with SV 40... Its unilateral withdrawal of vaccine from the market had not been well received by the DBS (Division of Biological Standards). If Merck recalled vaccine, then everyone else would have to. That would have resulted in public panic and would have run counter to the Technical Committee's May 18 directive that polio vaccination 'continue to be pursued with vigor with the materials presently available.' In June, after the Girardi cancer results had come in, Hilleman (Merck's science director) had tried one more time to get all vaccine production halted. That suggestion was rebuffed. Merck had already suspended production and was trying to figure out how to screen SV40 out of the vaccine when DBS tests on vaccine samples indicated that Parke-Davis supplies were also badly
contaminated. Parke-Davis now also stopped vaccine manufacture. The truth
was that by the time the Associated Press reported the 'news' in late July, both companies had not produced vaccine for several weeks. Parke Davis eventually resumed production, but Merck would soon decide that producing a polio vaccine that at times might be contaminated was not worth the risk." (Bookchin and Schumacker, 2004).
1962 "The Wistar human tissue study appeared in midsummer 1962, shortly before the human tissue study that Enders had completed at Hilleman's urging. Enders and his collaborator, another Harvard researcher, Harvey Shein, reached essentially the same conclusions as the Wistar group, with a different kind of tissue, human kidney cells. Koprowski had rushed the Wistar study into press hoping to scoop Enders and gain some publicity for Wistar. But in the end, despite being second, the Enders study attracted a good deal more attention because it was published in the prestigious Proceedings of the National Academy of Sciences. A lengthy New York Times story on August 10, 1962, reported the Enders study:
'A cancer-causing virus has for the first time produced cancer like changes in human cells... Changes that the virus produced in cultures of human kidney cells included greatly accelerated growth patterns and chromosomal aberrations...'
"By the fall of 1962, as news of the most recent SV40 research spread, the anxiety that had been growing in scientific circles about the simian virus rearched its zenith. 'It was the worst thing in the world,' Hayflick recalls of the news. 'Please tell me: What else could we find worse in monkey kidney cells?' In Britain, Wellcome Laboratories decided to stop inactivated vaccine production and switch entirely to live polio vaccine production."
"As in the United States, however, both the British and Canadian governments decided not to recall old stocks of Salk vaccine. Britain had a surplus of 6 million injections in 1961. In Sweden, the concern was about Sabin-type vaccine. There were plans to give monkey gamma globulin to four thousand children who had received oral vaccine in the belief that it would contain antibodies against any simian viruses, including SV40, which might have contaminated the oral doses. In the Soviet Union, site of the most extensive use of Sabin's vaccine, tests were conducted to determine the spread of SV40. Many of the technicians and scientists involved in Chumakov's massive vaccination trial proved to have been infected by the virus, and the Soviets were now fearful of SV40's possible
long-term effects. Among American research and health officials, a joke with gallows-type humor began to make the rounds: The Soviets would lose the 1964 Olympics because their athletes would all have tumors thanks to SV40" (Bookchin and Schumacker, 2004).
1972 Jonas Salk, inventor of the IPV, testified before a Senate subcommittee that nearly all polio outbreaks since 1961 were caused by the oral polio vaccine.
1992 America's Centers for Disease Control (CDC) in Atlanta admits in that the polio live-virus vaccine had become the main cause of polio in the United States. Specifically, the CDC asserted that, from 1973 to 1983, 87% of all (non-imported) cases of polio resulted directly from vaccine administration. Even more amazingly, it was asserted that every non-imported case of polio in the United States from 1980 to 1989 was vaccine-induced (Strebel, P. M., et al., Epidemiology of Poliomyelitis in the U.S. One Decade after the Last Reported Case of Indigenous Wild Virus Associated Disease, Clinical Infectious Diseases, CDC, February 1992, pp. 568-579).
1997 Polio is not eradicated by vaccination, but likely lurks behind a disease redefinition and new diagnostic names like viral or aseptic meningitis.......According to one of the 1997 issues of the MMWR, there are some 30,000 to 50,000 cases of viral meningitis per year in the United States alone. That's where it is thought that 30,000 - 50,000 cases of polio disappeared after the introduction of mass vaccination.
"Today, various other forms of the word "polio" are still used to describe the effects of poisoning, though usually with regard to paralysis in animals. A search of Medline ("polio" and "poison") finds about 45 contemporary articles where poisoning causality is attributed to polio. The terminology found was: "polioencephalomalacia", "poliomyelomalacia", "polyradiculoneuritis", "neurological picture similar to that of poliomyelitis", "polioencephalomyelomalacia", "lumbal poliomyelomalacia", "cerebrocortical necrosis (polioencephalomalacia)", "Lead poisoning in grey-headed fruit bats (Pteropus poliocephalus)", "multifocal-poliomyelomalacia", "spinal poliomalacia", "Polio and high-sulfate diets", "atypical porcine enterovirus encephalomyelitis: possible interraction between enteroviruses and arsenicals", "polioencephalomalacia and photosensitization associated with kochia scoparia consumption in range cattle", "bovine polioencephalomalacia." Viral or aseptic meningitis, Guillaine Barre Syndrome (GBS), Chinese paralytic syndrome, chronic fatigue syndrome, epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, ME, post-polio syndrome, acute flaccid paralysis (Jim West, Health and Research Publications, http://www.geocities.com/harpub/).
2002 Figures from the US Centers for Disease Control and Prevention showed there were 1,920 confirmed cases of polio reported by laboratories in 2002, up from 483 the previous year.
2004 (February) West Africa polio campaign is boycotted by Nigerian states.
A mass poliomyelitis vaccination campaign got under way to immunise 63 million children across west Africa but was boycotted by four predominantly Muslim states in Nigeria, where leaders claim the oral vaccine causes sterility and spreads AIDS BMJ (328:485 2004). The west African campaign was intended as a final push to stamp out the disease in the region and is part of the World Health Organization's 15 year drive to halt transmission of the poliomyelitis virus across the world by 2005. According to Dr Haruna Kaita, the head of the medical team that conducted the test in India, the vaccines contain "undeclared contaminants that can cause malfunctioning of the testes and cause infertility in women." The team also found "some toxic substances."
"Polio controversy started long ago," said Dr Kaita. "If you find one batch defective, you should condemn all batches. What these people [proponents of the vaccine] are saying is unethical, illegal, and criminal, and they know that these things are contaminated and they have the potential to cause human hazards. They should be banned rather than cause diseases in innocent children."
2006 (April) Associated press releases article claiming that Bangladesh will vaccinate about 18 million children aged 5 and under to combat polio, which recently re-emerged after authorities believed it had been eradicated five years ago, the country's health minister said Saturday. Bangladesh carried out extensive vaccination programs in 1995-2004, with the last polio case reported in August 2000, according to the government and WHO.
2006 (Sept 1) Polio reported on the rise in Nigeria Lagos, Nigeria despite near-universal vaccination. Nigerian authorities on Friday reported a sharp rise in the number of polio cases in Africa's most populous country over recent months, despite a government immunization drive.
"A total of 784 cases of the disease were registered in 17 states at the end of July, the National Programme on Immunisation said. In June the figures were 501 cases in 15 states, compared to 244 cases in 18 states for the same period in 2005, it said in a statement."
"From June 29 to July 3, Nigerian health officials in collaboration with United Nations health agencies launched an ambitious five-day Polio Plus immunization campaign of 10-million children in northern Nigeria aimed at eradicating the deadly disease from the country by the end of 2006."
2006 (December) Despite the 2004-5 west African polio eradication campaign intended as a final push to stamp out the disease in the region and is part of the World Health Organization's 15 year drive to halt transmission of the poliomyelitis virus across the world by 2005, the CDC, and WHO report that Nigeria now leads the world in new polio cases http://www.who.int/vaccines/immunization_monitoring/en/diseases/poliomy….
-Country: Nigeria
-Year: 2006
-AFP cases (acute flaccid paralysis) reported: 4937
-Non-polio AFP rate:6.7%
-AFP rate with adequate specimens: 88
-Total confirmed polio cases: 1044
-Wild-virus confirmed polio cases: 1043
-Polio cases attributed to vaccine: 9
Andrew, HIV science as a religion? That's so last year. Don't you guys ever come up with new material?
Oh, and I don't have time to read through everything you have on there at the moment, but Simon Flexner isn't the author of the Flexner report (for those unfamiliar, a document which recommended sweeping changes in American medical education, which at the time was sorely lagging behind that in Europe--Flexner suggested actual degrees and rigorous scientific training for MDs, so one can imagine why homeopaths didn't like it). Anyway, Simon's brother Abraham was the one who wrote the report, just FYI.
"Today, various other forms of the word "polio" are still used to describe the effects of poisoning, though usually with regard to paralysis in animals. A search of Medline ("polio" and "poison") finds about 45 contemporary articles where poisoning causality is attributed to polio. The terminology found was: "polioencephalomalacia", "poliomyelomalacia", "polyradiculoneuritis", "neurological picture similar to that of poliomyelitis", "polioencephalomyelomalacia", "lumbal poliomyelomalacia", "cerebrocortical necrosis (polioencephalomalacia)", "Lead poisoning in grey-headed fruit bats (Pteropus poliocephalus)", "multifocal-poliomyelomalacia", "spinal poliomalacia", "Polio and high-sulfate diets", "atypical porcine enterovirus encephalomyelitis: possible interraction between enteroviruses and arsenicals", "polioencephalomalacia and photosensitization associated with kochia scoparia consumption in range cattle", "bovine polioencephalomalacia." Viral or aseptic meningitis, Guillaine Barre Syndrome (GBS), Chinese paralytic syndrome, chronic fatigue syndrome, epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, ME, post-polio syndrome, acute flaccid paralysis (Jim West, Health and Research Publications, http://www.geocities.com/harpub/).
Isn't it a good idea to actually read what you cite? Actually if you cite Jim West it is probably better to not read it if you want to keep your grey matter intact.
Poliomyelitus (like influenza) was named before its cause was known.
Polio is derived from ancient greek for the color grey and hence grey matter in this case.
West's pubmedding resulted in this "Lead poisoning in grey-headed fruit bats (Pteropus poliocephalus)". Pteropus poliocephalus means literally grey-headed bat. The paper has nothing to do with poliomyelitis.
The rest of West's "science" is equally stupid.
There is no small irony in Maniotis accusing others of blindly following the "church of HIV" whilst credulously copying and pasting rubbish from pseudoscientific anti-vaccination websites.
So Dr Maniotis, it is apparent you do not believe polio virus exists. You do not believe HIV exists.
Perhaps you could save a bit of time and just list in alphabetical order all the other viruses you think do not exist, so we can all see exactly where you stand. (Or you could just cut and paste to someone like Lanka if you prefer). You seem to be quite the cut and paste expert; its a pity your comprehension of the material is so poor.
Dear Tara,
Sorry I posted twice somehow-remove one of them if you can.
Thanks for the info about the Flexner report. I was not aware that it was his brother that wrote it (I guess it figures though), and I haven't read it-only seen it referred to numerous times. But I have been reading a fascinating book about the series of "polio" epidemics beginning in 1890's and culminating in Vermont in various years leading up to The Great Epidemic in 1916. In this book, Poliomyelitis in Vermont, a series of maps appears where every case is shown geographically around the state by a red dot, with the author trying to piece together how it is spread, why only typically 1 person in a family gets it, why it is rural instead of cosmopolitan because one would expect it to spread along travel routes more frequently, why some farm animals appear to get it, what the occupations were of the heads of households that contained a polio victim, what their nationality was, what measures were taken by public health authorities each summer to quell the incidence, why it appears to occur in late summer months, how many cases recover, etc. There are many books written about the Great New York Epidemic of 1916, and what is most fascinating is the chronicle Called Dirt and Germs, The Great Epidemic of 1916. It is the story of how the public health officials tried to track, characterize, and isolate victims exhibiting the disease. Apparently spinal taps using mercury injections reached an all time high in the history of medicine during that year (folks like Flexner and the Medical Churchmen of that time were of course great advocates and practitioners of injecting mercury into peoples spinal fluid). Of course, polio, thought to be a disease of dirt and germs was first pinned on immigrants, the poor, and then when that hypothesis failed to materialize because public health officials and doctors learned that the poor ghettos in the broncs suffered far less polio that the burbs, the syndrome was then pinned on houseflies that would fly from the poor area and attack your baby (complete with big posters of enormous flies landing on infants, and then of course several decades latter, the DDT poisoning crusades were implemented to fight the disease, and did apparently affect both poor and rich (the first victim in Phily was a rich playboy, and FDR wasn't a ghetto child). Historically, the syndrome has mostly affected middle to upper middle class folks more than the poorest burrows where immigrants (thought to be the harbingers of the illness, and who were the subjects of mass public health campaigns to sequester them by pain of fines or forced detention).
The first decades of the 20th century also was a glorious golden time for vaccinations, after Rockafeller purged the Encyclpedia Britannica of all the vaccine damage and repeals of the last century gained by the Brits-it truly was a golden time when mass vaccinations were put into into place for other "diseases" such as small pox, and pertussis, and several others.
But what I don't understand is how any compassionate person could possibly advocate the continued testing and experimentation of vaccines on millions of children in light of the readily available evidence and statements by our own doctors and government institutions such as the CDC:
"1972 Jonas Salk, inventor of the IPV, testified before a Senate subcommittee that nearly all polio outbreaks since 1961 were caused by the oral polio vaccine."
"1992 America's Centers for Disease Control (CDC) in Atlanta admits in that the polio live-virus vaccine had become the main cause of polio in the United States. Specifically, the CDC asserted that, from 1973 to 1983, 87% of all (non-imported) cases of polio resulted directly from vaccine administration. Even more amazingly, it was asserted that every non-imported case of polio in the United States from 1980 to 1989 was vaccine-induced (Strebel, P. M., et al., Epidemiology of Poliomyelitis in the U.S. One Decade after the Last Reported Case of Indigenous Wild Virus Associated Disease, Clinical Infectious Diseases, CDC, February 1992, pp. 568-579)."
And despite near universal vaccination in countries like Nigeria, the highest rates of flaccid paralysis are seen today as reported on Christmas of this year.
I guess, despite what leaders in the field have said and warned about, apparently you people "know" what causes AIDS, polio, cancer, and just about everything else. Godlike in your knowledege would not be an understatement.
As for your statement:
"Oh, and I don't have time to read through everything you have on there at the moment, but Simon Flexner isn't the author of the Flexner report (for those unfamiliar, a document which recommended sweeping changes in American medical education, which at the time was sorely lagging behind that in Europe--Flexner suggested actual degrees and rigorous scientific training for MDs, so one can imagine why homeopaths didn't like it)..."
I can only say that I'm incredulous that you are thumbing your nose at "homeopaths" since you are a vaccine advocate and an advocate of the Jennerian myth, that vaccinations protect populations. For the sake of Christ, the practice of inoculation and vaccination were and are the mainstays of homeopathic "science!" Perhaps this is where the problem is amongst us?
From classical times, medical treatments have been predicated on either a rationalist or empiricist philosophy. Rationalists, as a group, tend to regard and approach disease as a localized entity and attack "it" directly by attempting to reduce or reverse its cause or primary symptoms. Radiation, mainstream chemotherapy, and targeted immune therapy are principal examples of a rationalist approach. Antiretroviral therapy (ARV) or HAART (Highly Active Anti Retroviral Therapy) are also examples of the rationalist approach, which employs the "law of contraries," to target a supposed exogenous and biologically unique virus in the case of "HIV," a supposed variant "of a known cancer virus," that is thought to be now responsible for 46 (47 if you now want to include amoxicillin adverse reactions, heart disease, birth defects of infants borne of women on ARV's) different syndromes that were previously known before "HIV" was announced by government proclamation as being the sole cause of "AIDS."
Empiricists tend to regard and approach disease as an imbalance in the living organism, which they attempt to restore by aiding the body in re-establishing its lost balance in ways that increase "resistance," or which non-specifically alert the organism via a "danger signal." Microbial immune therapy, antiangiogenesis therapy, and hyperthermic therapy are examples of an empirical approach. AIDSVAX, the GP120-based "HIV" vaccine is also an example of an empiricist approach, as it employs "the law of similars, to provide the organism with a similar substance (and not target the hypothesized cause directly), to alert the organism to subdue the exogenous invader, which is "HIV." Also, reconstitution of the immune system through nutrition therapy would be considered a form of empiricist therapeutics for immune suppressed individuals.
According to the "law of similars" and a basic understanding of physiology, cells and organisms are known to "push back" against a physical or chemical assault. Normally, the organism is in health at homeostatic balance, until illness results. Empirically, it has therefore been hypothesized, that when a similar disease-causing agent (like an active or inactivated virus, or its components) or a chemical is given to a patient that can produce the same disease symptoms in healthy people, the organism's own natural defenses are more likely to be strenuously evoked, and the illness overcome. Vaccines, cancer immunotherapies, hyperthermic therapies, histamine (not antihistimine) therapy for asthma, are all examples of using "the law of similars" in clinical practice.
"The law of contraries," that is principally touted by allopathic medicine (except of course for vaccinations which derives from the homeopathic idea of the "law of similars"), derives from the notions of Ehrich, Koch, and Virchow. Following "the law of contraries," it is believed that one can specifically target the molecular basis of a disease-causing agent or entity, much like dyes bind to fabrics, as this idea was borne out of the German dye development era of the 1800's during Virchow's, Erhlich's, and Koch's era. Anti-retrovirals and antibiotics, glucocorticosteroids, aspirin, mastectomies, heart surgery for clogged arteries, antihistamines, are a good examples of "the law of contraries" in clinical practice. Cut out the primary syndrome-associated symptom: heart disease: clean out or remove clogged arteries; bacterial infections-kill the bacteria' asthma-too much mucus in the airway-give whopping doses of steroids to suppress the natural immune response; cancer of the breast; chop it off.
Both approaches are "scientific", depending of course on how an experiment or trial is conducted (whether it is terminated prematurely as most, if not all of the FDA AZT and other antiretroviral trials have been for "compassionate reasons"), or, it may be considered a scientific approach if there are consistent results generated in a human patient, such as testing "HIV positive," "HIV positive," and "HIV positive." In science, a finding that repeats 2 times might be a fluke, while 3 points define a straight line, and constitute a minimum requirement to establish 'consistency,' or even 'a trend.' Rationalists also perform their medical experiments on an " average" or idealized patient harboring some "average" symptoms of "a disease," to the extent that even adverse or idiosyncratic reactions to medications such as amoxicillin are believed to fall into stereotypic responses, while empiricists perform their medical experiments in an attempt to restore the apparent imbalance manifested by person-specific, individualized symptoms that may appear different in each patient.
I have never seen two cancer patients die of the same disease. Have you?
Cheers,
Andy
So hard to follow the discussion with Mr. Troll and his sheets of quotes and his gallon jug of paste. But I want to answer Kevin, I want to thank you for being so gracious with me and not giving me the vitriol I deserve like you said.
I read Overdosed America by John Abramson last night. We can agree on something else, Kevin, its a very good book. Thing I like about it, is how Abramson is so common sense. I wrote yesterday of course there are problems with medicine and no one denies it. Abramson talks about some of them. I think he goes too far sometimes like that whole idea of America being so low on all the scales despite high health care spending. That's fallacy. You can't compare Japan or Sweden to USA. Japan, Sweden have very low immigrant populations homogeneous societies very little race problems poverty etc. etc. The USA is alot more diverse and that's very good but there are alot of injustices here and including in health statistics.
Mainly Abramson has some good ideas though. I'm trying to understand why you agree with him, Kevin. You sad that
I'm not saying that ALL doctors are ignorant shills...just the majority ;-)
I know your joking but Abramson doesn't say that even he even dedicates his book to all the health care professionals who are out there helping people. He doesn't call anyone a shill or anything he's against a system and incentives that can corrupt.
Abramson has alot of good things to say and he's fair.
From the book "Commercial funding does not necessarily impugn the conclusions of the study group."
Finally Kevin I wonder what you thought about this quote.
"The mortality rate from AIDS in the developed countries has gone way down as new drugs have been developed that control HIV infection."
Thats on page 43 from Dr. Abramson Harvard physician himself.
Andy not only apparently belongs to the "if you can't dazzle 'em with data, baffle 'em with bullshit" school of debate/discussion but he could be its poster boy. Congratulations Andy!
Yeah I wonder what he'll post next. Maybe something on window-tinting? Hermaphrodite frogs? A list of articles on joint pain? But maybe he covered all that already I really can't read Abramson AND Maniotis in one night.
"Fast forward to 2007. The average life span of an American is now 77. An improvement of 3 decades. The evidence speaks for itself." -- Raven
There is a difference between mere life extension and the quality of the life that is extended. Having read over your posts here, Raven, you seem to be even more of a simpleton than Dear Adele, and your jingoistic insolence is revolting:
"The life span of the average American in 1900, when modern medicine was young, was 47. About the same as trash heaps like Somalia and Afghanistan." -- Raven
Trash heaps, eh? Well, it's nice to know that you're not interested in playing the role of the enlightened and sensitive globalist. Of course, you're probably too stupid to achieve real deceit. However, since you're obviously a self-centered heap of trash yourself, I won't mince words. Modern medical advancements, i.e. treatments developed in the most recent twenty years or so, are not responsible for the increased longevity that privileged citizens of the world now take for granted. Clean water, adequate food supply, and basic treatments for once deadly infectious agents are responsible for the bulk of that improvement, and the most important of those advancements were made in developed nations long ago. Of course, you, Raven, seem to need to believe that poor nations are simply trash heaps, but anyone capable of understanding the dynamic factors involved knows that there are many other factors involved and that the modern medical establishment works hard to indoctrinate ignorant lackeys, such as yourself, because they realize that focusing of providing less-developed nations with clean drinking water and adequate nutrition would surely spoil the ruse that all those poor "trash heaps" really need is more expensive anti-virals.
"Well we haven't hit bottom in idiocy but we are way past sanity here." -- Raven
You were saying....
Previously, I wrote...If you weren't such a toady, Robster, perhaps you could connect the dots..., which you obviously found mildly offensive; however, allow me to demonstrate the veracity of my accusation using your latest response.
Since you claim to be such a masterful logician, Robster FCD, let's examine the logical connections inherent to your position, as provided by your own stated claims:
Statement #1...
"Of course, proper prevention would cut into the need for quite as many drugs, just one of the benefits of prevention.
Statement #2...
"The root is that people choose to live unhealthful lifestyles, and the system doesn't work to change that."
_________________________________
Your conclusion (statement #3)...
"It isn't the drugs or the pharma profits that are the root problem."
Your conclusion does not logically follow from the supporting claims you have made. In fact, your reply was an exemplary lesson in arguing around contradictions to save an unjustified false belief. Thank you for providing such a great example. As such, my accusation is valid. You harp on and on about prevention, which, incidentally, I agree is the key to improving health care, but you refuse to accept the logical conclusion that pharmaceutical companies play a major role in keeping modern medicine from achieving such improvements in preventative medicine, primarily because it would be financially disastrous for them. And that is the "broken promise of modern medicine" and no amount of denial will change that logical fact.
Kevin
So not only does Dr Maniotis think viruses like polio and HIV do not exist, but he is a believer in homeopathy.
HIV denial, germ theory denial and science denial all wrapped up in one package.... lovely!
Kevin,
You imply that improvement in longevity is due to several factors, but still deny the role of modern medicine in recent advancements in developed countries. Life expectancy is still rising - it didn't grind to a halt in the 1950s.
I'm glad you accept the role of treatments for infections, but don't forget vaccines. (Dr Maniotis, you reading this?)
However, to what do you ascribe the 7 or 8 year improvement in life expectancy that we have seen in the USA over the last 50 years?
http://en.wikipedia.org/wiki/Image:Life_expectancy_1950-2005.png
People in developed countries have had access to clean water and good nutrition over this period, I am sure you will agree. So why are they living longer in recent decades, if not because of better orthodox medical care? Any ideas?
Kevin, do you care to comment on Dr. Abramson's antivirals view or is he just another pharma shill to you?
Kevin. I found the toady line to be funny coming from you. Now to that hard to understand quote...
The problems with medicine are too little prevention and too much stress on late stage treatment from medicare and HMOs, which itself acts as a feedback loop against prevention. The structure of the system needs a complete reworking. [Your conclusion (statement #3)] -->It isn't the drugs or the pharma profits that are the root problem. [Statement #2] -> The root is that people choose to live unhealthful lifestyles, and the system doesn't work to change that. [Statement #1] -->Of course, proper prevention would cut into the need for quite as many drugs, just one of the benefits of prevention.
Since I admittedly wasn't as clear as I would like, especially when you cherry pick the middle and end of the paragraph and put the sentences in reverse order...
What drives the system? Money.
Where does the money come from? Health insurance programs including medicare/medicaid and HMOs.
What does insurance value most, based on what they pay the most for compared to the actual costs of service? Drugs and surgery, not office visits and prevention based counseling (which hardly breaks even).
Since money drives the system, if we weight the reimbursement programs towards prevention, we will see an eventual cut the need for as many drugs and surgery.
Personally I would like to see the HMO middle men cut out entirely, and replace it with a single payer system supporting healthy living.
Since we are doing book recommendations, I would suggest Farley and Cohen's Prescription for a Healthy Nation, 2005. Excellent overview of public health, even though they shy away from the political issues.
To DT. I don't necessarily believe in homeopathy. It was Chris Noble that knighted me a homeopath-ologist-for which I thanked him, and posted my new title on my office door to intrigue my co-workers. I think it could be a new field.
If you read about the theoretical basis of homeopathy, and vaccines, you will find that they are one and the same. I'm not a fan of either homeopathy or allopathy-as neither one have made much of a dent in cancer, acquired immune difficiency diseases, or any other major human health issue. I was simply asking Tara why she thumbed her nose at homeopathic theory when she appears to be a vaccine advocate and Jennerian groupie when in fact the basis of both innoculation and vaccination is "the law of similars" as I described above, which is rooted in homoeopathic thinking.
You ask what viruses I believe in and don't believe in so that you can dismiss every piece of information I have presented to you learned people who know how EJ died.
However, I would like to emphasize that it isn't about what I believe in...its about what evidence there is to link a virus to a disease in some consistent manner that makes sense. Even an infant who shakes a rattle, and then sound is made, can believe that the shaking of the rattle causes the sound. Put the virus in pure form into an animal (or human by accident) and show that they will become ill, and that it has a pathogenic mechanism.
For instance, when Tommy got chicken pox, my mommy took me, and all the other mommies took their children down to Tommy's house to get infected. We all got infected. I got little pox on my nose. I would bet it was filled with the virus that has been shown to be associated with that type of lesion, in just about everyone who has acquired the syndrome. I believe the scientific case of chickenpox has been established.
If you read the history of vaccination literature, you will find that smallpox was much the same in terms of chicken pox in areas of the middle east. People have documented how people "purchased the pox" and actually paid out money depending if one acquired the innoculum from 4 pox on somebody's face, or 20 pox. They would then make the lancet scars on the arm, and rub the dried pox powder onto the wound and get a mild form of the syndrome. There is evidence, therefore, that "small pox" of that era was different than some of the more devistating epidemics that wiped out 50% of some cultures. Do I believe that both of these were the small pox virus? I don't know exactly what to believe. Do you?
Do I believe that West Nile virus was isolated from a Black woman in the Nile delta in 1938 before electron microscopes even were working, because of course, as a virus, it ultimately has to come from black people doing something "animal-like." Instead, I tend to defer to Tracy MacNamara's work on "WNV" cross reacting on ELIZA's with SLE (St. Louis Encephalis), which I grew up with and which was always associated with a predictable number of summer cases of encephalitis. Therefore, I'm not a big fan of the toxic pesticide industry coming by my house this summer and spraying their deadly toxic neurotoxins into all our trees so that it makes our pasta taste bad, as they did a few years ago. I don't think its good for the children to push these toxins into the environment. We even threatened them a few years ago to no avail. They doubled their speed when all us parents got out on the street to block their trucks, they came by right at dinnertime, and sprayed their shit into our open windows (that were open because it was a hot July evening).
Do I believe in hepatitis C virus? Don't know. I've never seen one (and neither has anyone else), and even if I did, I've never seen a virus cause a disease like cancer 40 years after it is supposedly acquired-same with HBV or HPV, or HTLV-I abd HTLV-II (first thought to cause increased cancer rates in those cohorts studied living 170 miles from Hiroshima). Viruses cause cancer? So do atom bombs dropped on civilian populations. Sorry to be so impious.
To Tara,
RE:
"However, even medical science doesn't say that all people who are HIV+ will develop AIDS. We know of groups of people who have been HIV+ for years, yet are apparently just fine (even without antiretroviral drugs). These are known as "long-term nonprogressors," and are a group that's actively being studied to see just how they're holding the virus in check--what is it about them that keeps them OK, whereas other people succumb in just a few years if they're not treated? Again, where AIDS deniers sees a group like this and goes, "aha!! These people aren't dying of AIDS, therefore HIV doesn't cause AIDS!", infectious disease epidemiologists, virologists, and immunologists see this as an expected outcome that we see with every other pathogen, and an opportunity to better understand the host/virus interaction."
"Similarly, there are people who are repeatedly exposed to the virus, but never seroconvert."
Really?
I hope everyone had a chance to read the vile racism of the denialist and see who these people really are.
as a virus, it ultimately has to come from black people doing something "animal-like."
Since no one in the medical community I have EVER heard of EVER said ANYTHING like that, not even anything close to it, why would anyone write such a beyond offensive ugly thing? Well there's the old strawman but I think its more than that. It's like denialists are so full of hatred and bitterness and have these nasty thoughts and ideas and can't express them so they pretend someone else, an enemy of theres, is saying them. That way they get to say what they really think and at the same time blame it on someone else they don't like. It's sick. Really, really sick when a guy lets something like that sentence stand beside his name. A shame to himself and his family and his institution.
Andy said:
Do I believe that West Nile virus was isolated from a Black woman in the Nile delta in 1938 before electron microscopes even were working, because of course, as a virus, it ultimately has to come from black people doing something "animal-like."
Adele said:
I hope everyone had a chance to read the vile racism of the denialist and see who these people really are. As a virus, it ultimately has to come from black people doing something "animal-like."
Since no one in the medical community I have EVER heard of EVER said ANYTHING like that, not even anything close to it, why would anyone write such a beyond offensive ugly thing? Well there's the old strawman but I think its more than that. It's like denialists are so full of hatred and bitterness and have these nasty thoughts and ideas and can't express them so they pretend someone else, an enemy of theres, is saying them. That way they get to say what they really think and at the same time blame it on someone else they don't like. It's sick. Really, really sick when a guy lets something like that sentence stand beside his name. A shame to himself and his family and his institution.
Dear Adele,
before you quickly jump to conclusions and shout to the world that Andy is a dirty racist, perhaps you might consider that you have misinterpreted his intended meaning, which was sarcasm. It is surprising that you would make such a great error in interpretation.
Of course, Andy is surely no racist. However, Andy surely is attributing the rascism to you, Adele, and others like you who believe that West Nile, like HIV, MUST have orginated in black people. The racist part comes in where your theories of West Nile or HIV for example attribute various specific characteristics to black people which then results in further spread of the microbe (such as an overactive sex life or sexual contact with animals).
Perhaps Adele should read a few articles from the recent science literature concerning the origin of HIV. They are all perfect examples of racism in action.
Better yet, take a look in your own back yard, here on this BLOG
A Quote from Aetiology; a discussion of how HIV originated in african monkeys and "jumped species" to africans via the sexual route.
I wonder if there is reason to suppose that "butchering or consumption of bush meat" led to interspecies transmission (of HIV ) rather than the obvious route of sexual contact. "Obvious?" Sexual contact with animals is something you consider more ordinary than hunting and eating them? Man... I suppose we don't want to know details about your lifestyle, do we?
I rest my case.
"Kevin. I found the toady line to be funny coming from you." -- Robster, FCD
Oh, Robster, you are most certainly more "toady" than I am. Are you familiar with the following etymology of that word:
...originally referring to the assistant of a charlatan, who ate a toad (believed to be poisonous) to enable his master to display his skill in expelling the poison (1629).
How appropriate for the circus that is HIV/AIDS. After all, you and the other toadies on this blog are the ones bending over backwards, embracing contradictions, all in the service of the easily-identified charlatans who represent HIV/AIDS. Your devotion to their cause knows no bounds for you readily abandon your integrity and extol their collective expertise in beating-back a harmless retrovirus, while ignoring convincing counter-evidence almost completely--a very religious gesture, indeed. And now for the best part: guided by the charlatans' collective expertise, a significant portion of our society, mostly the under-privileged, have been convinced that the ritualistic swallowing of innumerable "poisonous toads" is actually good for them, despite devastatingly-apparent serious side effects. Curiously, the now huge pool of patients swallowing these "toads", or medicines, just so happens to have came about concurrent to astronomical increases in personal wealth for the modern-day charlatans, who, of course, provide these dangerous "medicines". In your world this fact of their massive wealth accumulation is totally unrelated, right?
I think it's pretty clear who is more "toady", Robster, FCD.
_________________________
"Since I admittedly wasn't as clear as I would like, especially when you cherry pick the middle and end of the paragraph and put the sentences in reverse order..." -- Robster
What would I hope to gain by cherry-picking your responses when any reader can simply scroll-up to see the full text? I wasn't cherry-picking; I was pointing out the relevant claims you made. The logical conclusion from your comment was clear, even if you don't seem to understand the implication of your own argument. That tends to be the case when one is arguing from the deficient position. Delusion becomes a necessity. For example, it's much more difficult to ever say what you "really" mean. In addition, my re-arranging of your statements, which were provided verbatim, was equally appropriate. After all, a conclusion is sometimes given before all of the premises are revealed, particularly when given in paragraph form. I was merely arranging your claims in a simple syllogism. Once again, I can't help that you don't seem to understand your own argument.
______________________
You're talking out of both ends, Robster, so as to avoid the most logical conclusion from the statements you've made. Let me explain further:
Statement #1:
"Of course, proper prevention would cut into the need for quite as many drugs, just one of the benefits of prevention.
Statement #2...
"The root problem (see conclusion) is assisted by the fact that people are encouraged to live unhealthful lifestyles through the use of unscrupulous corporate advertising which promotes unhealthful products, such as fast-food and chemically-drenched health and beauty products (among others), and such a system will never work to change that situation because the profits are their primary concern, regardless of industry."
_________________________________
MY conclusion (statement #3)...
"Therefore, it is the ever-increasing dependence on drugs as a substitute for comprehensive care, and the HUGE profits that those drugs yield that are the root problem of our health care system."
See how much more logical my argument is? It's really very simple. All one has to do is ask the logical question of "why" our current system doesn't seem to want to change our collective unhealthy lifestyles. The answer is clear: our health care system cares far more about profits than improving health, and the evidence is apparent at every level. So, you are either a deluded fool or a dishonest toady, and I suspect that both apply.
Kevin
Racist you say!
I believe the term used was "NATIVE," and although the ref I remember was 1938 it was actually 1940. So sorry to get the date wrong. But by 1940, I'm sure you infection people agree that there had been plenty of time to do sucrose density gradients for viral isolation along with EM and pathogenicity studies (making healthy animals develop the disease from the sucrose density isolate that was photographed as being a relatively pure viral isolate), just like with "HIV."
Smithburn KC, Hughes TP, Burke AW, Paul JH. A neurotropic virus isolated from the blood of a NATIVE of Uganda. Am J Trop Med Hyg 1940: 20:471-92.
Indeed, my comment wasn't sarcasm-my comments tried to convey the disgust regarding YOUR continuing vile racist policies of "HIV," in context and with respect to your "risk groups," with respect to the proposed circumcision of every African male living on the entire African continent (who are "waiting in line just eager to get circumcised as the New York Times and other propagandistic outlets released before Bailey even published his data), with respect to smearing microbicides on the genitals of the entire African continent (as Moore and others have proposed by virtue of their "HAIL Mary experiments" that have only unfortunately led to the discontinuation of at least two CDC-publicized microbicide trials, because their microbicides increased the rate of "HIV" infection in the genitally-smeared Africans, with respect to "Hep B" and Australian aboriginals, and, as I posted to earn the term "racist," "West Nile Virus" being isolated from a Native Ugandan.
E.G.
"The "cryptic argument," that every person on the planet must be vaccinated because the hepatitis B "virus" can hide in cells in "chronic carriers" for decades without causing clinically detectable disease, and then mysteriously, decades later, "cause" hepatocellular carcinoma, ignores the fact that seropositivity for the hepatitis B antigens may not have any-thing to do with serum hepatitis. In the vast majority of seropositive individuals without liver disease, the presence of the HBV markers may represent non-specific markers of immunological stress, or merely represent a normal genetic polymorphism, as was originally thought by Baruch Blumberg (who discovered the Au antigen, HbsAg, in the blood of a black Australian aboriginal, and of course was awarded the Nobel Prize for finding that virus in a Black person, that he shared with NIH's former Neurobiology Program director, D. Carlton Gajdusek--the discoverer of the so-called "slow virus" prion diseases-who as the head of the NIH's Neurobiology Program, and who rescued the failing virus-cancer hypothesis (not as skillfully as Gallo did however with HTLV-III), before he plead guilty of course to multiple counts of pedophilia and child sexual abuse for his habit of shipping over some of the subjects he studied in New Guinea to his home in Maryland.
Washington Free Press, #66, 2003]
http://www.wafreepress.org/66/crimeOfBeingPoor.htm
"Sex Crimes"
"The past decade has seen the demonization of sex criminals. Sex offenders must register with police and face a host of other restrictions. But unlike crimes committed mostly by the poor, sex crimes still allow for extremely lenient sentences of probation and suspended sentences, with judges and prosecutors deciding who gets these light sentences. It never hurts to be wealthy when convicted of a sex crime. With the exception of drunk driving, no other crime cuts across class lines more frequently than pedophilia. Yet what spurs judicial and prosecutorial outrage when committed by the poor, provokes little more than yawns when committed by the wealthy and well heeled. Daniel Gajdusek won the Nobel Prize in medicine in 1976 for his research in slow viruses that attack the body, such as mad cow disease and AIDS. In 1997 Gajdusek, then 73, pleaded guilty in Maryland to two counts of child sex abuse for molesting a 16-year-old boy he had brought to the US from the Pacific Islands, where he had conducted most of his research for decades. Gajdusek was sentenced to 30 years in jail but then had all but 18 months of the sentence suspended by circuit court judge Jim Dwyer."
All told, starting in the 1960s, Gajdusek brought 56 children, mostly boys, from the Pacific Islands to his Maryland home, ostensibly to educate them. At least five boys claimed that Gajdusek molested them. Gajdusek served little less than a year in jail. But his lenient treatment didn't stop there. Within hours of being released from jail in 1998 Gajdusek left for France, where prosecutors agreed to let him serve his five-year probation unsupervised. Gajdusek's lawyer said he would continue his "scientific work" there. Presumably poor pedophiles that don't have Nobel prizes would have had to serve their probation sentences in the US, and register as sex offenders with the attendant hassles that that entails. That Gajdusek used his "work" as a ruse to perpetrate his sexual abuse of children for almost four decades was not mentioned by the court or prosecutors who frequently raise the topic in other contexts."
Its not that I don't believe that that child sexual abusers aren't worthy of deep respect and Nobel prizes for their science that postulates things like "slow viruses" and such. Its just that they, like famous athletes, besides their enormous contributions to science, serve as role models for young and in earnest lab techs and other scientists (like me when I was a lab tech back in the 1970's and perhaps others like that impressionable Adele writing on this blog today). In this context, and as an impressionable young aspiring scientist myself, I even met Gajdusek in a famous lab I was a tech in, when he was invited by my boss to give a lecture on his work. When he came, I gazed at him in admiration and awe, as an example of what an anthropologist could accomplish in this life!
For their discoveries, the doctors (Blumberg and Gajdusek) were jointly given The Nobel Prize in Physiology or Medicine in 1976 "for their discoveries concerning new mechanisms for the origin and dissemination of infectious diseases," because the infectious agents and mechanisms of disease causation they postulated, were believed not to conform to the standards of accepted pathogen isolation, the idea of distinctive genetic (nucleic acid) identity, the timing of infection to demonstrable cell pathology or morbidity, or to the classic proofs of pathogenicity worked out by Koch and others after Koch. For instance, D. Carlton Gajdusek championed the idea that "infectious proteins" devoid of nucleic acids were at the basis of slow, debilitating neurodegenerative disorders (e.g., kuru, CJD, Mad Cow, scrapie in sheep)--syndromes that are characterized by extremely long latency periods after initial "infection," and destruction of the brain tissue years or decades after "infection." Although the concept of slow viruses, and pathogens devoid of nucleic acids were vigorously challenged and rejected by many in the scientific establishment during the 1980's because the idea challenged the established biochemical chain of events worked out for other infectious agents, and because these syndromes appeared to be both infectious and run in families, Stanley Pruisner believed Gajducek's hypotheses to be plausible, and found that the hypothesized disease-causing PRP protein was present in both diseased and healthy hamsters (for which another Nobel Prize was awarded). (It really pays to study "virsues" don't it)?
Blumberg termed the rare "hepatitis B" antigen, Au, for Australian antigen, because the Au antigen was first found in the blood of a healthy black, Australian aboriginal man, but he also detected it in the blood samples of Micronesians, Vietnamese, Taiwanese, Native Americans, and patients with Down syndrome, leukemia and transfusion patients. Blumberg acknowledged, however, that the vast majority of people, who test positive for HbsAg or HbeAg, never become sick, develop hepatitis, or cancer of any kind.
For instance, as the first to identify the hepatitis B antigen in their survey of genetic polymorphisms in blood samples, Blumberg and Alter reported that leukemia patients (not liver cancer patients), patients with Down syndrome, hemophiliacs, and blood transfusion recipients tested positive more than the general population for the hepatitis B antigen, yet rarely developed liver hepatitis [Blumberg BS. Hepatitis B virus, the vaccine, and the control of primary cancer of the liver. PNAS, 1997; 94:7121-5.], suggesting there is no specificity or pathogenicity with respect to Au marker and the appearance of the rare hepatitis B syndrome.
What is most puzzling perhaps, is that Blumberg's major focus at first was not directed toward studying liver hepatitis, but inherited genetic (blood) polymorphisms in the tradition of Boyd and others. Are we to assume that because "hepatitis B virus" is thought now to be transmitted through sex and dirty needles and perinatal transmission, or transfusions, that black men who are Australian aborigines all share these risks or risk behaviors? Or does the HPsAg antigen represent a simple and relatively rare (in the West-not so rare in Asia or Australia or Africa) blood polymorphism because most people never become sick, develop hepatitis, or cancer of any kind?
Nor in the context of hepatitis B and cancer, is it clear why Blumberg's hypotheses regarding HBsAG antigen suggested to him that (Blumberg B. PNAS, Vol. 94 pp 7121 -7125, 1997, page 7123 top):
"i) Individuals with Au have an increased susceptibility to leukemia (NOT HEPATOCELLULAR CARCINOMA as is continuously touted by The WHO and the PHS), and this susceptibility is inherited."
Similar to "HIV-AIDS" "science," we see here that hepatitis B is currently proposed to be sexually transmitted, be transmitted through blood or blood products, and it causes a cancer, hepatocellular carcinoma, according to the CDC, the WHO, and other Public health agencies. Unfortunately, if you read Blumberg himself, this "virus" was associated with leukemia, not hepatocellular carcinoma. From Baruch Blumberg, PNAS, Vol. 94 pp 7121 -7125, 1997):
"ii) Leukemia causes Au (HbsAg)" (again not hepatocellular carcinoma);
"iii) Au is related to "the virus" that has been postulated to be the cause of leukemia.
Again, why not "hepatocellular carcinoma?" Do viruses cause leukemia? Read (try to read) Gallo on this one.
Why did Blumberg think "family studies" of carriers (of HbsAg) "were consistent with a genetic hypothesis of inherited polymorphism," yet allowed the idea to be advanced that hepatitis B was transmitted as an infectious agent? How could an inherited trait be infectious? This question, stimulated a lot of controversy and dissent during the 1960's and 1970's, and similar arguments were made regarding the prion diseases postulated by Carlton Gadjucek.
Why did Blumberg believe that HbsAg was an infectious agent linked to leukemia when he was fully aware that "certain individuals were susceptible both to the development of Au-positivity and leukemia" (not hepatocellular carcinoma) and that "children with Down syndrome have a rate of HBsAg of approximately 30% compared to other patients housed in mental institutions whose rate of HbsAg was approximately 5%? Does trisomy have an infectious basis also? Are Down people more promiscuous than other institutionalized persons? Do they share needles? Consume blood products? Eat feces, as suggested by a gifted virologist friend of mine (who confused Hep A with the imagined pathogenesis of Hep B).
Blumberg in his PNAS paper goes on to tell us about his collaborative work with Bayer and Werner in their Philadelphia laboratory who identified particles with the "appearance" of a virus in the serum of individuals with Au (HbsAg antigen) on page 7123, (paragraph 3-4 at the bottom of the first column). Why does Blumberg then emphasize that these particles were subsequently shown to "not contain any nucleic acid" or even "core proteins," and tell us that they were "neither infectious or pathogenic?"
Also, why does Blumberg tell us about how I. Millman and V. Coyne in his lab were able to "localize Au" in the liver cells of patients with hepatitis, and yet elaborate as to why it was it so "difficult to confirm" they were able to sustain the growth of "the virus" in liver cells obtained from patients with liver disease associated with Au? A related question is, why don't chimps show any liver pathogenicity, cellular damage, or develop anything resembling hepatitis in modern studies when they are infected with hepatitis B (Guidotti et al., Viral clearance without destruction of infected cells during acute HBV infection, Science 1999 Apr 30;284(5415):825-9)?
Also regarding racism, Dr. John Moore of Weil Medical College, one of the featured speakers in the 2006 International Toronto AIDS Conference is an enigmatic character. In a talk he gave at the conference about his work, which involves inseminating rhesus macaques up to 5 times after smearing a spermicide cream in their vaginas to prevent "SIV," he claimed that these "HAIL MARY" experiments hold great promise and could solve the "AIDS apocalypse in Africa and elsewhere. He claimed that multiple inseminations are necessary in order to model the frequent sexual activity that goes on in these 3rd World Nations. Not being Catholic, I didn't quite understand at first what was meant by the term "HAIL MARY experiments." To rigorously prove his "SIV-fighting" spermicide worked, I gathered that HAIL-MARYING HIS monkeys and inseminating them 4-5 times represented the fact that his spermicide "absolves" the monkeys of contracting "SIV," as one would if a Catholic perhaps were "absolved of sin" after saying "HAIL MARY" numerous times as penance?
Although "SIV" has always been a better model of "HIV" than "HIV," a critic might suggest Moore try Human "HIV," perhaps with dogs, cows, goats, sheep, or non-infected monkeys, chimps, and humans that have naturally occurring "HIV" sequences (Horwitz MS, Boyce-Jacino MT, Faras AJ. Novel human endogenous sequences related to human immunodeficiency virus type 1. J Virol. Apr;66(4):2170-9, 1992). Although none of these animals acquire AIDS from "HIV," neither do his monkeys since he is inseminating them with "SIV."
Regarding one campaign funded by The Gates foundation, AIDS denialists claimed that spermicide doesn't actually reduce any risk of transmission but actually increased the rate of infection. This runs contrary to what is known about how safe sex practices, including condoms and spermicide, can be completely effective in quelling AIDS in backward 3rd World countries (remember the A,B,C,'s cited above-Abstanence, Being Faithful, and Condoms)? Although it is difficult to believe that AIDS denialism has even affected such organizations as the CDC and WHO, the evidence is overwhelming that this is the case, as in the following article (Maggie Fox. Spermicide worsens HIV risk, study finds. Reuters 12 July 2000):
"South Africa -- Researchers hoping to find a way for women to protect
themselves from AIDS have said they were dismayed to find that a product they thought may prevent infection actually increased the risk.
The product, a spermicide called nonoxynol-9, did not protect prostitutes in Benin, Ivory Coast, Thailand and South Africa from infection with HIV, a
team of U.N.-sponsored researchers said.
"We were dismayed to find out that the group using the N-9 gel had a higher rate of HIV infection than the group using a placebo,'' Dr Joseph Perriens, who heads the UNAIDS microbicide effort, told an AIDS conference Wednesday.
They tested nearly 1,000 women and found 59 of those who used the spermicide became infected with HIV, compared to 41 of those who used a dummy gel.
"We were extremely disappointed,'' Lut van Damme, a researcher at the
Institute of Tropical Medicine in Antwerp who led the study, told a news
conference.
She said researchers may be forced to suspend other trials involving the
product, marketed under the trade name Advantage S by U.S.-based Columbia Laboratories Inc.
"The long-term safety of nonoxynol-9 as a family planning method may have to be re-evaluated,'' she said.
Activists and researchers have been clamoring for the development of a
microbicide -- a gel or cream sometimes described as an "invisible condom'' -- that women and men could use to protect themselves not only from HIV, but from other sexually transmitted diseases such as syphilis and gonorrhea.
"I think this may be the end of nonoxynol-9 as a potential microbicide,''
Van Damme said, although she said the trials did show that women -- in this case prostitutes at high risk of HIV infection -- would use a microbicide if one was available.
CDC Expresses Concern
The Centers for Disease Control and Prevention (CDC) said it was concerned by the findings because some groups advise people to use nonoxynol-9 to protect themselves from HIV if they cannot use a condom.
"I think it's pretty clear we have to tell men who have sex with men not to
use it,'' Dr. Lynn Paxton, a microbicides expert at the CDC, said in an
interview.
"I think they are most at risk and I know they are using it.'' She said it
was less clear whether women who use nonoxynol-9 as a contraceptive -- women who are not at risk of getting HIV -- should avoid it.
"One possible reason for the findings was that the women who used the
spermicide had more lesions than the women who did not," Van Damme said.
"If you use nonoxynol-9 (to protect from HIV), you are probably wasting your money. You may possibly be wasting your life,'' Perriens said. But, he
added: "There is nothing in this trial to suggest you should stop using it
as a spermicide.''
UNAIDS said it was pressing for the development of other products.
"We know that there are more products to come,'' Perriens said. "This
shouldn't be the end of the field... One of the things holding up
development, increasingly, is a lack of private sector interest in this area.''
The Bill and Melinda Gates Foundation said it would try to help with a $25 million grant for microbicide research."
Fortunately, the AIDS denialists at the CDC are no longer hampering work or being pessimistic about this important area of spermicide development as they have in the past. And a week or so ago, Bill and Melinda Gates said during their keynote addresses at the 16th International AIDS Conference opening ceremony in Toronto that:
"A total of 16 microbicides -- a gel or cream used to block infection -- are currently being evaluated. Of those, five are in major advanced studies. Drug trials into oral prevention drugs are also underway."
At the conference, Melinda Gates further encouraged researchers and politicians alike to move past the stigma of HIV/AIDS:
"Stigma is so cruel," she said. "It's also irrational. Stigma makes it easier for political leaders to stand in the way of saving lives."
The couple last week announced that their foundation would contribute $500 million over five years to fight HIV-AIDS, and met with Bill Clinton, the former U.S. president, to present their priorities for ending the epidemic.
Last but not least, and regarding racism:
December 14, 2006 New York Times editorial article entitled, "Rare Good News About AIDS," came as a shock:
"The announcement yesterday about the results in two African studies of male circumcision may be the most important development in AIDS research since the debut of antiretroviral drugs more than a decade ago. The National Institutes of Health halted studies in Uganda and Kenya when it became overwhelmingly clear that circumcision significantly reduces men's chances of catching H.I.V."
Cheers,
Andy
Kevin, you suggested a book for me to read and I read it. I liked it and praised it. I asked you one little question about it. But you won't answer. I don't understand.
Although "SIV" has always been a better model of "HIV" than "HIV," a critic might suggest Moore try Human "HIV," perhaps with dogs, cows, goats, sheep, or non-infected monkeys, chimps, and humans that have naturally occurring "HIV" sequences (Horwitz MS, Boyce-Jacino MT, Faras AJ. Novel human endogenous sequences related to human immunodeficiency virus type 1. J Virol. Apr;66(4):2170-9, 1992). Although none of these animals acquire AIDS from "HIV," neither do his monkeys since he is inseminating them with "SIV."
I'll call your bluff on this one. The endogenous sequences in the Horwitz paper are only about 30 bp and even then they only have a sequence similarity of about 70%.
Compare this with SHIV that are largely HIV.
You can't have it both ways. You can't claim that HIV is endogenous because of the sequence similarity between HIV-vau and a 30 bp region of the human genome and then complain about SIV not being HIV.
A related question is, why don't chimps show any liver pathogenicity, cellular damage, or develop anything resembling hepatitis in modern studies when they are infected with hepatitis B (Guidotti et al., Viral clearance without destruction of infected cells during acute HBV infection, Science 1999 Apr 30;284(5415):825-9)?
According to Duesberg chimpanzees are susceptible to all human infectious diseases with zero exceptions.
If you read about the theoretical basis of homeopathy, and vaccines, you will find that they are one and the same. I'm not a fan of either homeopathy or allopathy-as neither one have made much of a dent in cancer, acquired immune difficiency diseases, or any other major human health issue. I was simply asking Tara why she thumbed her nose at homeopathic theory when she appears to be a vaccine advocate and Jennerian groupie when in fact the basis of both innoculation and vaccination is "the law of similars" as I described above, which is rooted in homoeopathic thinking.
The only people that seriously talk about homeopathy and allopathy are quacks.
Vaccination has nothing to do with homeopathy. Vaccination induces antibodies that can be observed and measured. Homeopathy has absolutely no basis in science. If vaccinations were based on homeopathic principles you would expect homeopaths to be for them. They aren't. If anything they encourage "homeopathic vaccinations" that are so diluted that they don't actually contain any active ingredient and don't provide any protection against anything.
Again, the irony in someone on the one hand claiming that there is no evidence for the existence of HIV and on the other hand taking homeopathy at all seriously is mindboggling.
Andrew,
Are you really so helpless when trying to understand an essay?
Blumberg's paper (Free Full Text Available Here--http://www.pnas.org/cgi/content/full/94/14/7121) is a Perspective Article providing the historical context for the discovery of Hepatitis B Virus (HBV) as an example of how enormous but completely unexpected clinical benefits can be produced by basic research.
The three hypotheses you quoted were Blumberg's initial hypotheses regarding the significance of Au, the "Australia Antigen" eventually shown to be the surface antigen of HBV. As he describes in the paper, when they tested these hypotheses by experiment, they instead found the unexpected association between Au and hepatitis. He vividly describes a key patient who clued them in to the connection:
He then describes the discovery of the virus, the production of the vaccine, and the impact the vaccine is having on the epidemiology of hepatitis and hepatocellular carcinoma. He even goes on to address your question about the connection with leukemia:
He tells a fascinating history of the evolution of scientific ideas--how they change in response to experimental results and conceptual advances. A quality that the pseudoscientific mumbo jumbo you spout noticeably lacks.
The product, a spermicide called nonoxynol-9, did not protect prostitutes in Benin, Ivory Coast, Thailand and South Africa from infection with HIV, a team of U.N.-sponsored researchers said.
Aren't Denialists using the argument that prostitutes don't get HIV and therefore HIV is not sexually transmitted?
Andrew, with every post you are looking more and more disconnected with reality.
Regarding homeopathy, you clearly have no idea about its underlying principles (or should I say the lack of them). Homeopathy proponents like to blur the (biologically vast) distinction between vaccination and homeopathy, because it lends them a degree of scientific credibility ("Its just like vaccination you know, using exactly the same principles"). Complete hogwash.
Vaccination relies on the administration of sufficient quantities of antigenic material to provoke a measurable and predictable immune response in the host. The antigen itself is a modified version of the pathogenic organism, in that it has been altered to lose its virulence (A process that may not always be fully successful as in the case of oral polio for example). [BTW, how do you square up your observation that Sabin vaccine can cause paralytic polio when you also think the polio virus does not exist?].
In vaccines the antigen is measurable, and in fact is usually given at a dose several orders of magnitude higher than would ever be encountered naturally. This is totally at odds with the homeopaths law of dilution/infinitessimals, where the compound administered is usually a lactose tablet which has had magic water dropped on it, water which does not contain a single molecule of the original nosode whatsoever, but is somehow meant to have preserved a memory of that one specific substance (but bizzarely not a memory of the thousands of other substances that the water may have previously come into contact with).
This magical memory can allegedly be transmitted from one tablet to another just by bringing them in close proximity (but apparently any distance will do since this property can even be transferred via the internet).
Vaccines induce a specific measurable response in the host, homeopathy does not and cannot. You imply that the scientific principles of vaccination support a "law of similars" in the sense that they are used in homeopathy, which they are clearly not. Equating the two just shows you are what we would call on this side of the pond "integrity-challenged".
OTOH, perhaps you really are someone who would willingly take a homeopathic malaria vaccine before a trip to Africa, relying on your scientific certainty that it would "fill the malaria-shaped holes in your energy"?
Robster, you asked: "Does anybody remember the name of the AIDS patient who bought into the denialist lies, and later died from an OI? The denialists said that he had started abusing illegal drugs causing his death, instead of the OI. I think it would be a worthwhile read for observers."
If you just want to know of denialists who have died from AIDS, there are plenty. Some have had near-death recantations, including guys like Pasquarelli who decided to take the offer of HAART, even though it proved too late for him (and he still managed to maintain his semblance of denial to the end). For others it also came too late, including one chap called Jack Levine who used to be active on the virusmyth site. Some, like Winston Zulu, have discovered their error in time.
However, I think you mean Raphael Lombardo. His story is a particularly unedifying episode in the annals of AIDS denial.
http://www.virusmyth.net/aids/data/pdazt.htm
As you can see from Raphael's frank letter to Duesberg (about half way through the virusmyth link), he never did drugs. But he bought into the denialist lie after his correspondence with Duesberg and thought he would live forever. When he did die of AIDS, Duesberg tried to imply it was because Lombardo had lied about taking drugs, and blamed them for his death, rather than AIDS.
Just to follow up on Lombardo, here is stuff Chris Noble archived about the case.
Here is what Duesberg said about Lombardo's frank exposition of his (drug free) gay lifestyle, once Duesberg found out he had died:
Yup, sure Duesberg, imply he lied about drugs.
You will see that Duesberg also blames Huw Christie's death on drugs, not HIV
Sickening stuff really.
Yes it is very strange Andy says vaccination is based on homeopathy, but he also says commandos with big guns come to your house and inject gram quantities of pathogens and adjuvants into your little cherubs. Gram quantities and homeopathy? Homeopathy's supposed to work without a single molecule of the original substance.
On drugs and AIDS, Tara said it with goalposts. Denialists say poppers gives you AIDS, but there are cases without poppers. So then they say it's any drug of abuse. And if somebody isn't a drug user, then they're lying. Or they took prescription drugs. Alcohol, maybe? Until the entire world except for maybe a few cult members living in a camp in Nevada should be suffering from AIDS. Denialists accept this kind of thinking and blame scientists for being to lazy!
Yes of course. Drug abuse explains the cases of HIV+ newborns, pediatric AIDS patients. Who have a short lifespan without HAART. Everyone knows there are hordes of 1 year olds roaming the streets of the world, buying drugs and shooting up.
This thread has shown just how intellectually bankrupt HIV denial is. There is no idea so kooky that someone won't fervently believe in it. I read one site that claims that the USA is extensively tunneled with hundreds of miles of underground complexes. Space aliens live down there. Several species in fact. The latest news is that everyone is mad at the "Greys". Apparently the Greys have been acting up again and are in violation of several treaties.
How odd. What sentient creature would come hundreds of light years to live in a tunnel complex under North America? And why?
I think what drives a lot of this HIV denial is just routine old fear. No one wants to hear that they have an incurable virus that will kill them sooner or later in an unpleasant slow way. Understandable to some extent.
It's not quite the case today which makes denial destructively pointless. HAART extends lifespan by an average of 13 years in the US. Optimal treatment would be more like 20 years. This is to the point where many patients end up dying of other diseases first. And the treatments keep getting better. Who knows what will be available 20 years from now?
In Denmark they estimate survival on treatment to be as long as 35 years. So of course patients will be dying of other diseases. Denialists twist this fact around and claim that patients are dying of the toxic effects of the medications. Whatever it is due to, you can be sure the meds are to blame. Even old age will be labelled as HAART toxicity soon.
To be fair, HAART does increase the risk from other disorders such as liver and cardiovascular events. But the rise in these is tiny in comparison to the lives gained/saved by the treatment. The denialists just spout garbage like "Liver deaths have doubled! - Shock, Horror! Evil toxic drugs to blame!"
The facts are that the drugs are only partly to blame (hepatitis being the main factor). If mortality from liver probs/hepatitis rises in patients on HAART from 5 to 6 deaths per annum but AIDS mortality is almost halved from 45 deaths to 24 deaths per annum, then you have the apparent paradox where "Liver deaths have doubled!" from 10% to 20% of all deaths! So denialists can deviously state they are telling the truth, but it is only their perverted version of it, I'm afraid.
Raven said: Yes of course. Drug abuse explains the cases of HIV+ newborns, pediatric AIDS patients. Who have a short lifespan without HAART. Everyone knows there are hordes of 1 year olds roaming the streets of the world, buying drugs and shooting up.
Dear Raven, if there is no connection between maternal drug use and pediatric AIDS, please provide a reference in the medical literature to any newborn pediatric AIDS study in which the mothers ARE NOT I.V.DRUG USERS In fact, they all are IV drug users.
Regarding the other disparaging comments above by the obvious paid shills for Big Pharma, ad hominem attacks on people in absentia is fairly typical for AIDS apologists, since they have nothing else to offer. Under normal circumstances a few references in the medical literature would be sufficient to make a point...however, there are none that can be provided, except for pointing to government web sites that proclaim all scientists believe HIV is the cause of AIDS because if they dont believe, then the NIH funding gets cut off. Lately their funding is getting cut off anyway and the infighting has been vicious. (i.e the fiasco in HIV Vaccine funding).
Regarding the administration of toxic anti-HIV drugs to pregnant mothers and their newborns. This is a criminal act whether they are HIV true positive, or HIV false positive. Those responsible will be held accountable at some day in the future.
RAVEN said: I think what drives a lot of this HIV denial is just routine old fear. No one wants to hear that they have an incurable virus that will kill them sooner or later in an unpleasant slow way. Understandable to some extent.
Raven is correct about the element of fear. However, the fear factor comes from AIDS INC from the old television ads which constantly drum the refrain, HIV is the cause of AIDS and all HIV positives will surely die, and the government and the medical system will protect you with their medical reseach and medical science.
The reality is that there are plenty of examples of HIV positives who live healthy lives without drugs. To live such a HIV positive life is difficult with the constant fear mongering bombardment from the media that death from AIDS is around the corner. The stories of HIV positives who refuse toxic drugs and live long healthy lives abound on the internet.
The reality is that the toxic HIV drugs are useless at removing HIV. It is impossible to remove a nucleotide sequence from the human genome with toxic drugs, and that is what HIV is, a nucleotide sequence in the human genome. However, these drugs are very successful at delivering toxicity to the rest of the human body with liver failure, and hideous lipodystrophy of the face which looks like phantom of the opera.
Raven mentions bancruptcy, but again Raven misplaces the true object of the preposition. It is the HIV causes AIDS hypothesis that has bancrupted the national treasury, and taxpayers are asking the lab for results for all their hard earned money. The labs have no results for them, only hollow slogans. 20 years and no vaccine. 20 years and the new drugs are hailed as miraculous because they dont kill off the patients at the same horrendous rate as the older AZT. 20 years and no mechanism of disease. That is what is called bancruptcy.
FMAAP posted if there is no connection between maternal drug use and pediatric AIDS, please provide a reference in the medical literature to any newborn pediatric AIDS study in which the mothers ARE NOT I.V.DRUG USERS In fact, they all are IV drug users.
In fact there is a connection between maternal drug use and pediatric AIDS because the incidence of HIV seropositivity is higher in drug using women than in non drug users. But HIV negative drug users do not have HIV positive babies and not all HIV positive babies are born to drug using mothers.
Google "hiv newborn Yoon" for an example of a study in which 25% of HIV positive babies were born to non drug using mothers.
I see the reality deniers are now outright lying. Maintaining a delusional belief system must be hard work. Here is one such study. In Argentina, the main way that women become infected with the HIV virus is through sex. Well duh, HIV is commonly a sexually transmitted disease. Some of the women's consorts are IV drug users. Not surprising either, IV drug users are a known high risk group for blood borne infections such as HIV. Some are not however.
So is IV drug use something that can be acquired? And then become hereditary? And then kill babies quickly? Sort of lacking a mechanism or agent here aren't we? Not really, HIV can be acquired a number of ways, it can be vertically transmitted from mothers to newborns, and it causes AIDS in them.
1: Int J Infect Dis. 2002 Mar;6(1):9-16.Links
Clinical and epidemiologic aspects of human immunodeficiency virus-1-infected children in Buenos Aires, Argentina.Fallo AA, DobrzanskiNisiewicz W, Sordelli N, Cattaneo MA, Scott G, López EL.
AIDS Reference Center, Division of Pediatric Infectious Disease Hospital de Niños Dr. Ricardo Gutiérrez, Buenos Aires, Argentina.
BACKGROUND: Argentina has the sixth largest number of cumulative pediatric cases of acquired immunodeficiency syndrome (AIDS) in the Americas; therefore, this study was designed to characterize human immunodeficiency virus-1 (HIV-1) infection in children in Buenos Aires, Argentina. MATERIALS AND METHODS: Medical records of 389 children at risk and infected with HIV-1, an urban population followed by the AIDS Reference Center at the Hospital de Niños "Dr. Ricardo Gutiérrez" of Buenos Aires, from February 1990 to June 1997, were retrospectively reviewed. Mother-infant pairs were analyzed according to clinical and epidemiologic patterns. RESULTS: Perinatal transmission occurred in 94.9% of the 389 cases classified as seroreverter (n=104, 26.7%), exposed (n=64, 16.4%), asymptomatic (n=13, 3.4%), and symptomatic patients (n=208, 53.5%); 132 patients met the Centers for Disease Control and Prevention (CDC) criteria for AIDS.
************************************
The main maternal risk factor was sexual transmission 58.9% (73.4% of their sexual partners were injection drug users [IDU]).
**************************************************
Among the AIDS patients, the most common AIDS-defining condition and death-related disease were severe bacterial infection and Pneumocystis carinii pneumonia, respectively. Death occurred in 51 of 221 HIV-infected children. Low CD4 was related to death (P < 0.001). Mortality was estimated for two periods: January 1990 to December 1995 (G1) and January 1996 to May 1997 (G2). In G1, 37 of 127 (29.1%) died compared with 14 of 154 (9.1%) in G2 (P=0.001). The median age of death was 10 months for G1 and 29 months for G2 (P=0.01). The 3-year survival rate was 72% for G1 and 87% for G2 (log rank P=0.06). CONCLUSIONS: Intravenous drug use is the leading risk factor among parents of children exposed to HIV. Infant mortality was related to age less than 12 months, low CD4 count, severe bacterial infection and P. carinii pneumonia. In this study, P. carinii pneumonia prophylaxis and combined antiretroviral therapy routinely implemented since 1996 has demonstrated a trend toward increased survival rates (P=0.06) and a lower mortality rate (P=0.001).
Google "hiv newborn Yoon" for an example of a study in which 25% of HIV positive babies were born to non drug using mothers.
You can lead a mule to knowledge but you can't make it drink.
It is entirely unreasonable of you to expect that a Denialist would actively seek knowledge that might refute his deeply held beliefs. I'm sure he'll just go back and read a bit more Duesberg.
Sickening stuff really.
The way they treated Jack Levine was sickening too.
While Jack was healthy his Denialist friends gave him support and understanding. Jack followed the standard advice. Don't take recreational drugs. Don't take ARV. Eat well etc. Nevertheless, he still progressed to AIDS with a number of opportuinsitic infections that are rare in the general population. He began to doubt the advice he had received from his friends and supporters.
What happened when he expressed his doubts about HIV "dissidence". His former friends disowned him. One of them said he had never been a true "dissident". Obviously true HIV "dissidents" don't get AIDS. Some of the more paranoid "dissidents" accused him of being a pharma-shill plant. Apparently the pharmaceutical companies are so evil that they hire plants to pretend to be HIV "dissidents" for several years and then pretend to die from AIDS. Others invented fanciful explanations to explain away the fact that Jack took the "dissident" advice, didn't take ARVs and still came down with AIDS.
Meanwhile Jack was dying from AIDS and his previous support groiup had abandoned him. Sickening.
I've read on another website that HIV deniers seem to come and go.
No one is too sure why. But the betting is, 1 of 2 things happen.
1. They get sick and decide to go on HAART.
2. They get sick and decide to forgo HAART and die.
The second option is not at all uncommon, especially in Africa where HIV is prevalent and knowledge and HAART is not.
Hey 40 mules,
Here's a ref for you from a multicenter prospective study conducted in the USA:
Abrams, E J et al. (2003). Maternal health factors and early pediatric antiretroviral therapy influence the rate of perinatal HIV-1 disease progression in children. AIDS:Volume 17(6)11 April 2003pp 867-877.
In a prospective study of the children of 2656 pregnant and postpartum HIV-infected women they identified 360 children infected with HIV. During the first two years of life, 116 of these children were diagnosed with AIDS and 13 died of HIV-1 related causes prior to an AIDS diagnosis. Of these 129 unfortunate children, 76 (or 31.5%) were born to mothers with no history of IV drug abuse.
Hey 40 mules,
Here's the ref you asked for from a multicenter prospective study conducted in the USA (with my error on the percentage corrected):
Abrams, E J et al. (2003). Maternal health factors and early pediatric antiretroviral therapy influence the rate of perinatal HIV-1 disease progression in children. AIDS:Volume 17(6)11 April 2003pp 867-877.
In a prospective study of 2656 pregnant and postpartum HIV-infected women and their children they identified 360 children infected with HIV. During the first two years of life, of these 360 children, 116 were diagnosed with AIDS and 13 died of HIV-1 related causes prior to an AIDS diagnosis. Of these 129 unfortunate children, 76 (59%) were born to mothers with no history of IV drug abuse. Of the 241 children born to HIV-1 infected mothers who had no history of IV drug abuse, 31.5% developed AIDS or died of HIV-1 related causes within the first two years of life.
If forty mules or his plow manage to read the article that Franklin cites he would also read.
The majority (71.3%) of AIDS diagnoses and deaths occurred in untreated children. Fewer than 6% of children receiving NRTI only, dual NRTI, or PI therapy during the 0-6 month age period met the endpoint compared with 19.7% of children not receiving treatment (Table 4). During the 6-12 and 12-18 month age intervals, respectively, similar proportions of children in the no treatment (15.1%, 8.6%), NRTI only (15.4%, 12.8%), and dual NRTI (13.8%, 9.4%) categories met the endpoint. In comparison, fewer than 4% of children treated with more complex antiretroviral regimens met the endpoint during these age intervals.
I eagerly await the homeopathological explanation for this. The larger the number of different ARVs the better the outcome.
Hey Andy's Defender,
Just like Andrew, you seem a little reading-challenged, too.
Perhaps you should take another look at the first paragraph of the Results Section at the top of Page 61 to find the truth about the study population:
So your claim that this study and all the studies of pediatric HIV/AIDS are done on drug addict mothers is false.
Is it a reading problem? Or maybe you know your position can't win in an intellectually honest atmosphere, so you support it with falsehoods that most readers won't bother to check. Classic pseudoscience--just like Andrew.
Andrew,
You really have a hard time understanding clinical papers, don't you?
This paper compares patients started on HAART therapy in 1995-96 (when HAART first became widely available) to patients starting HAART in'97, '98, '99, 2000, '01, or '02-'03. It asks whether the modifications made to HAART therapy since it was first introduced have altered patient response compared to the earliest forms of HAART. So when they report no "decrease in mortality" within the first year of starting HAART therapy, they have found that HAART as practiced in 2002-03 compared to HAART as practiced in 1995-96 shows the same 1-year mortality. This mortality is much lower than that of the pre-HAART era.
To find a study that asks if HAART confers a decreased mortality compared to the pre-HAART era, you should look up the appropriate papers cited by the authors of the Lancet paper:
14 M Egger, B Hirschel and P Francioli et al., Impact of new antiretroviral combination therapies in HIV infected patients in Switzerland: prospective multicentre study, BMJ 315 (1997), pp. 1194-1199.
20 RS Hogg, B Yip and C Kully et al., Improved survival among HIV-infected patients after initiation of triple-drug antiretroviral regimens, CMAJ 160 (1999), pp. 659-665.
33 A Mocroft, S Vella and TL Benfield et al., Changing patterns of mortality across Europe in patients infected with HIV-1, Lancet 352 (1998), pp. 1725-1730.
Look, ref 33 is a Lancet paper. You seem to like that journal. Why not read it and get back to us. Here's a sneak preview to whet your appetite:
Sounds like those computer modellers at the NIH just might be on to something!
Forty assumes ALL women giving birth to HIV+ babies are intraveinous drug users. We just saw that isn't true, so Forty is wrong.
Forty also assumes ALL drug users in these studies continue using during pregnancy. Sometimes true sometimes not true. The mothers are sorted by risk factors for infection and if someone was or is a injecting drug user they are listed that way. It doesn't mean they still are! Some stopped drug use before they got pregnant and some when they found out they were pregnant. For alot of these babies they didn't get exposed to drugs in utero but they still got HIV. So there goes Forty's drug use HIV theory for those kids.
Doesn't really matter though because drug use doesn't give anyone HIV or AIDS. Like above no babies get HIV or AIDS when they have drug-using moms without HIV.
Dear Raven,
regarding your reference which was supposedly cited to show that pediatric AIDS studies can be conducted in a population sample consisting of non-drug using white suburban housewife moms:
According to the report you cite, 73.4% of the dads admitted on a questionairre that they are IV drug users. How many of the moms are IV drug users? It doesn't say. Let's ask a hypothetical question. If you had a room full of 20 male IV dug users accompanied by their pregnant sex partners, how many of the females in the room on average would you think might be IV drug users as well? Many of them.
Also notice in this paper, like all the others, the greatest mortality among the babies is in the first 6 months, which is expected in babies born from drug addicted mothers. The authors cites a TREND toward improved survival over time which, in their opinion , they attribute to treatment. Rather than a refutation, your citation is actually supportive of the fact that mothers of AIDS babies are mostly black, minority group, inner city, poverty stricken drug users. Note the letters IDU means injection drug user.
Raven's citation 1: Int J Infect Dis. 2002 Mar;6(1):9-16. Clinical and epidemiologic aspects of human immunodeficiency virus-1-infected children in Buenos Aires, Argentina.Fallo AA, Dobrzanski Nisiewicz W, Sordelli N, Cattaneo MA, Scott G, López EL. AIDS Reference Center, Division of Pediatric Infectious Disease Hospital de Niños Dr. Ricardo Gutiérrez, Buenos Aires, Argentina.
The main maternal risk factor was sexual transmission 58.9% (73.4% of their sexual partners were injection drug users [IDU]).
CONCLUSIONS: Intravenous drug use is the leading risk factor among parents of children exposed to HIV. Infant mortality was related to age less than 12 months, low CD4 count, severe bacterial infection and P. carinii pneumonia. In this study, P. carinii pneumonia prophylaxis and combined antiretroviral therapy routinely implemented since 1996 has demonstrated a trend toward increased survival rates (P=0.06) and a lower mortality rate (P=0.001).
Dear Franklin,
Thanks for citing the following article from Harlem Hospital Center and Columbia University which is intended as a refutation in which you intend to show that HIV positive babies come from drug free mothers.
This study was conducted in inner city hospitals, and 40% of HIV positive babies are born to mothers who freely admit they are IV drug users:
Abrams, E J et al. (2003). Maternal health factors and early pediatric antiretroviral therapy influence the rate of perinatal HIV-1 disease progression in children. AIDS:Volume 17(6)11 April 2003pp 867-877. Setting: Urban medical centers in four cities in the USA. In a prospective study of the children of 2656 pregnant and postpartum HIV-infected women they identified 360 children infected with HIV. During the first two years of life, 116 of these children were diagnosed with AIDS and 13 died of HIV-1 related causes prior to an AIDS diagnosis. Of these 129 unfortunate children, 76 (or 31.5%) were born to mothers with no history of IV drug abuse.
Actually look at Table 2, you will see that of the 341 HIV babies, 100 of the mothers freely admitted to IV drug use. 241 did not. Think about it, if you were an IV drug user, which is not a socially acceptable thing, would you freely admit to it?
If you disagree with this, then perhaps you could give me an estimate of how many IV drug users on average on a standard medical questionaire will put a check in the box for YES I am an IV drug user and how many will choose not to disclose this information by placing a check in the NO box?
Also, how many cocaine, oxycontin or methadone addicts would deny being IV drug users even though they are chemically addicted? After all, these drugs are not taken IV, yet they result in drug addiction for the mother and fetus. Bottome line, again this study was conducted in INNER CITY hospitals on poor black drug users. Where are the studies on white suburban non-drug using moms? There aren't any.
In addition, giving AZT or protease inhibitors to the mothers or the babies doesnt help them to cope with the effects of drug addiction/withdrawal. AZT and anti-HIV drugs cause neurodevelopment problems in the fetus on top of the street drug issues. Administration of these toxic drugs to pregnant inner city mothers is a huge medical experiment which should be halted. HIV is a nucleotide sequence in the human genome which cannot be eradicated by administration of toxic drugs. You can be certain that in the future, those responsible for conducting these hideous experiments will be held accountable.
For more information see: www.livingwithouthivdrugs DOT com
I notice Forty that you didn't bother commenting on Yoon. Probably because in that study mothers were actually tested for drug use.
"Kevin, you suggested a book for me to read and I read it. I liked it and praised it. I asked you one little question about it. But you won't answer. I don't understand." -- Adele
Dear Adele,
You claim to have read the book I recommended and for that, you want accolades? Yet, not surprisingly, you've failed to demonstrate any understanding of the central theme of the book, which leads me to believe that perhaps you didn't actually "read" the book. Instead, your only comment is a decidedly cherry-picked comment about the apparent efficacy of HIV medicines. If our mutual pal, Robster, is still following the discussion, you've provided him, and all of us, with a proper lesson in the art of "cherry-picking" -- that very dishonest analytical method that Robster, and others here, like to bandy about whenever a dissident exposes HIV's significant shortcomings. Of course, having established that Robster is quite a "toady" fellow in my previous post, I suspect that he'll fail to learn from the cherry-picking lesson you've so graciously provided.
Now, before I answer your dubious question regarding the apparent efficacy of HIV medicines, readers should be made aware of the central theme of the book that you supposedly mastered in a few hours. Incidentally, I tend to read slowly so as to give thought to what I'm reading, while I'm reading it. You should try that method, Adele. I realize that this assumes one is capable of significant comprehension, which you Adele have consistently failed to demonstrate. Now, let's continue examining the central theme. Even a cursory look at the chapter titles from the book in question -- Overdosed America -- provides insight into the central theme of the book:
Chapter 2: Spinning the Evidence -- Even the Most Respected Medical Journals Are Not Immune
Curiously, you fail to offer any quotes from this section, Adele. Why? It's one of the most important chapters in the book. Dishonest posters such as Dale, DT and the ever-ignoble Chris Noble would most certainly benefit from the information in this section.
Chapter 4: The Myth of Excellence
Now, this was a brilliant chapter and on topic since many of the less-enlightened posters on this blog (Hello, Raven) want to claim that health care in this country is marked by excellence. Alas, you fail to offer up any insight here, Adele. Why?
Let's do one more...
Chapter 7: The Commerical Takeover of Medical Knowledge
A superb chapter! Our mutual friend, Robster, could really benefit from reading this section, but being an established toady for Big Pharma, that is unlikely. Pity. Perhaps you Adele -- having mastered this work -- would like to provide, Robster, with a succinct summary of this very illuminating chapter?
___________________
Now, I haven't forgotten how much you like to be reminded of my own health history, Adele, but it is quite relevant to the current discussion. Besides, we may new readers. Either way, I do expect a typical response from you since you seem to understand that the implications of my "story" are unflattering to the HIV explanation of AIDS. Nevertheless, it bears repeating that, two short years ago, I was extremely sick with numerous AIDS-defining OIs, all in the absence of HIV! Of course, now that I've regained my health, I realize that I am far better equipped to "connect the dots" than most, but the information is now available for anyone to digest, even if their situation is less inspiring than acute survival!
Of course, I employed mostly alternative treatments, which are frequently disparaged by members of the peanut gallery here; however, I did not completely shun modern medicine. After much research, I realized that my compromised immune system had been caused by the antibiotics that my numerous doctors were giving me, indiscriminately, for recurring bacterial infections. My AIDS, and I suspect the AIDS that is attributed to HIV, was the result of a severe and long-standing fungal infection, so I took powerful anti-fungals at extremely high doses for a total of 16 weeks. That's what it took to see progress. Amazingly, my health improved impressively by combining this treatment with numerous alternative measures designed primarily to help me detox from the years of antibiotic abuse -- the therapy that my doctors wanted to continue even after it was apparent that my problems were almost entirely fungal-related. Thankfully, I found an enlightened DO who understands the big picture.
In summary, had I tested HIV positive, I'm sure that I would have been given HAART, and it very well may have improved my condition since it appears to be quite effective at resolving mutiple infections, including fungal infections. However, that was not an option for me since I was test-negative. Of course, testing the efficacy of HAART on HIV-negative AIDS cases will never happen because any clinical improvements would undermine the causal connection between HIV and AIDS; thus, in the long run, drug companies would lose all those healthy HIV-positive patients who are scared into taking HAART based on the test result, alone.
I would love to discuss this issue with Dr. Abramson, the author of Overdosed America. Of course, I would point out that the efficacy of HAART is most likely best utilized as a short-term treatment for the most severe cases of AIDS, whether positive or negative. In addition, I would note that most AIDS patients will test positive since they are most likely suffering from numerous infections that will trigger a positive response, due to the cross-reactivity of the tests. In that respect, I consider myself quite lucky -- never testing positive, in spite of numerous recurrent infections.
Did you get all of that, Adele? Perhaps, you should practice your comprehension skills and read it, again -- preferably before you offer up one of your typical juvenile responses.
Reading over all of the examples here from the likes of Noble, Dale and DT is truly dispiriting. Such ignorant toadies with such a limited understanding of the realities of AIDS....
Kevin
Kevin,
By your own admission, your story has nothing to do with AIDS. You were not HIV positive but had a medical problem that was, in the end, treated and resolved using conventional medicine. End of story.
Still, I wonder why you believe that if HAART were efficacious in treating conditions other than HIV infection, it wouldn't it be used for this purpose. After all, if Big Pharma is as greedy as you seem to think, there are far more HIV negative individuals (and therefore potential customers) in the Western world than there are HIV positive individuals. Why would they deliberately restrict their potential market?
Sorry, Kevin. I spent the Father's day weekend with my family, and didn't pay much attention to the net. Congrats on looking up the etymology of "toady." It still doesn't change your dishonest tactics in misquoting me.
But please, you say that I am a toady for ignoring convincing counter-evidence almost completely--a very religious gesture, indeed.
What convincing counter-evidence? You have none. And when offered evidence that HIV causes AIDS, you ignore it. Are you aware of the psychological concept of projection?
-----------------
40 mules, nice cherry picking of a comment from an old thread. The comment you quote out of context, without formatting, was a response to someone making a comment that had strong racist overtones. Said offensive commenter did not return.
-----------------
DT, Chris, thanks for finding the accounts of how the denialist camp throws their own under the bus when they have the audacity to die from AIDS OIs.
Well, Dale, perhaps you should work on your reading comprehension skills, too. Maybe you and Adele could form a study group.
You wrote:
Still, I wonder why you believe that if HAART were efficacious in treating conditions other than HIV infection, it wouldn't it be used for this purpose...Why would they deliberately restrict their potential market?
I wrote:
Of course, testing the efficacy of HAART on HIV-negative AIDS cases will never happen because any clinical improvements would undermine the causal connection between HIV and AIDS; thus, in the long run, drug companies would lose all those healthy HIV-positive patients who are scared into taking HAART based on the test result, alone.
In order to improve your understanding of the situation, Dale, you are going to have to abandon your Group Think mentality, if just for a moment. To continue the ruse that these drugs are necessary to combat a rapidly, mutating virus is paramount to maintaining ANY significant patient population for these drugs, and you know the reason why, even if you can't bring yourself to say it. These drugs are extremely cyto-toxic, and they really should only be used as a short-term stopgap, followed by appropriate adjunctive therapies; nevertheless, they are not appropriate for treating even serious infections, no matter their efficacy, unless all other means have been exhausted. After all, such high-levels of efficacy are not achieved without significant health costs, and the general public will probably be far less tolerant of lipodystrophy and live failure, et al, than has been the frightened and vulnerable gay community, especially when other drugs are potentially effective at treating the individual ailments that are now erroneously known as HIV/AIDS.
You were not HIV positive but had a medical problem that was, in the end, treated and resolved using conventional medicine. End of story. -- Dale
Once again, you need rise above the dogma, Dale, if you ever hope to gain any real understanding. Just like a Christian Fundie, you begin with God, (HIV in this case), and then you proceed to massage the data to fit your crumbling belief system. You would certainly like to believe that my being test-negative is "end of story", but others might find it curious that I had PCP, esophageal candidiasis, and recurrent pnuemonia...and that's just for starters. Those are AIDS-defining illnesses, are they not? If I was in Africa, I would have been shunned for having "slim" disease, no doubt, since I lost over 60 lbs in less than year. My conventional doctors tested me for HIV numerous times. In fact, that's about all those worthless hacks (university-affiliated, no less) could think to do, which isn't surprising, for I now understand just how endemic the Group Think is within the medical community and how doctors receive most of their "continuing education" from drug company representatives. After finding the competent D.O., I had to take diflucan at 500 MG for 16 weeks. If you know anything about that medication, then you know that that is far from a "conventional" dosage, as you so flippantly suggest. Treatment at lower doses consistently failed to resolve my acute problems and my health continued its rapid decline. The alternative methods and an altered diet were equally essential as the 500 mg of Diflucan.
It should be noted that I am not implying that this condition will ever be easy to treat, but with comprehensive care, it can be overcome. Of course, it also helps not to cause the problem in the first place, whether doctor or drug addict, or both. The fact remains that current treatment protocols, namely HAART, do not prolong life, and there are many studies demonstrating that very fact. Granted, patients improve initially, but they still die, with the major change being liver failure has now replaced PCP as the defining death knoll. Your forthcoming denial won't change that fact, either, Dale.
You're losing this argument and for good reason. I've lived through this horror, close to the bone, as they say, and your deluded spin is so very obvious to any else who has endured such poor treatment while in the care of our "excellent" health care system.
Kevin
ps
Adele, I eagerly await your chapter summaries...after all, you said you really enjoyed the book. Besides, Dale is an even bigger bore than you.
Kevin, the reason for clinical trials is to overcome the biases inherent in drawing any conclusion from a sample size of one. In fact, as has been pointed out to you many times by many individuals, clinical trials demonstrate that HAART is effective, although not 100% so.
In the case of any chronic disease for which there is no cure, individuals often become progressively more ill before they die. As they are ill, they are likely on medication. That is true for AIDS patients, for cardiac patients for diabetics, etc. etc. Some of them die. Not because the medication killed them but because the medication failed to save them. No medication saves everyone but the studies show that AIDS patients with access to the best treatments (including but not restricted to HAART) have a longer life expectancy than those who don't.
As far as HAART. If HAART resolved symptoms in non-AIDS patients that would not restrict Big Pharma's HIV patient market in the slightest - it would just open up the market to the far larger market of non-AIDS patients.
Finally, regarding the relevance of your personal medical history to AIDS - you just don't seem to get it. Nobody. Any. Time. Ever. Has said that you must be HIV positive in order to be immunosuppressed. So based on your symptoms you were likely immunosuppressed. But you didn't have AIDS.
Hey Chris, Adele, DT, Raven, Tara, Kevin, 40 mules and a plow, and anyone else posting here I may have missed, I got paid a few days ago, and was thinking that if all of you help me, we could put together a package of about 500 condoms for these people who need to eat food. Shouldn't set us back that much if we all pitch in.
"And with poverty afflicting nearly 50 per cent population, the great majority of people who need to use condoms have to choose between spending money on it or buying food. Government supplies through dispensers at social places remain the only viable source. Prevention is still central to the government strategy for containing sexually transmitted infections and HIV/Aids. And condoms are a big part of that strategy."
Makokha's Memos: a Worrying Break in Condom Supply
The Nation (Nairobi)
COLUMN
16 June 2007
Posted to the web 16 June 2007
By Kwamchetsi Makokha
Nairobi
Kenya is in the grip of a condom crisis because of procurement irregularities. A Ministry of Health survey of distribution across the country shows that this year's stock levels at just under 30 million for males against an annual requirement of 132 million. Female condom stocks stand at 85,180 against an annual requirement of 1 million.
According to the US Aid's Kenya: Final Country Report released in March, some 300 million condoms bought with World Bank funding were expected to run out mid-last year. Although the Government secured some Sh240 million to buy 120 million more condoms that would give an 18-month reprieve, the delivery has not been made because of pitched battles over the supply tender. Twice in recent times has the Government asked the United Nations Population Fund (UNFPA) to provide emergency supplies to stock dispensers around the country.
UNFPA is giving 25 million male condoms and 197,000 for females. Although the Global Fund for Aids, malaria and TB does not usually buy condoms, the crisis in Kenya forced it to pledge 30 million male condoms. The shortage has caused a sharp decline in supplies to outlets right up to the location level.
A Ministry of Health distribution survey done in Nyanza, Nairobi, Coast and Western provinces shows a sharp decline in the supplies over the years. Between August and December 2004, more than 50 million were distributed in the areas studied -- partly because the sheaths were available and there was money for distribution.
The figures for February to June 2006 are half that. By July 31, last year, the areas surveyed were receiving a total of 13 million condoms -- a 68 per cent decline in supplies. Supplies have been cut back as areas that are not using as many condoms as they receive are ordered to return unused stocks for redistribution.
Supplying condoms is big business. The sheer volume of the orders guarantees bidders who win the supply tender a handsome profit - even if their margins are as low as 50 cents a piece.
Since condoms are manufactured to internationally accepted standards, people who bid for the supply tender often have the same qualifications.
The tendering battles are bruising and could go to the highest levels of government. Picking one and not the other usually sets off a chain of complaints and appeals that inordinately delays delivery.
A ministry official who cannot be named for this story, said buying condoms in bulk introduces a financial dimension to the exercise that can delay procurement for months - even years.
The only way to avoid the battles, he suggested, was to reduce the volumes bought so that procurement covered three or six months rather than three years. Thanks to the thriving commercial spirit in Kenya, many people can buy male condoms at anywhere between Sh10 and Sh350 for a pack of three. There are, however, places in this country, where social marketing has not caught on.
And with poverty afflicting nearly 50 per cent population, the great majority of people who need to use condoms have to choose between spending money on it or buying food. Government supplies through dispensers at social places remain the only viable source. Prevention is still central to the government strategy for containing sexually transmitted infections and HIV/Aids. And condoms are a big part of that strategy.
The Total War on Aids initiative has budgeted $12 million (Sh804 million) for condom purchases over the next three years.
Since the introduction of female condoms in Kenya a few years ago, there has been no proper research on the demand for their use and attitude towards them.
If we all buy them about 500 condoms, and perhaps a few bottles of water, it won't cut back the promising work now ongoing with the "HIV" vaccines, despite the criticisms from the AIDS vacine denialists that have compromised the progress of the "HIV" vaccine program? E.G.
"HIV" vaccine denialism advanced by Donald Francis, David Baltimore, Richard D. Klausner, Julie Louise Gerberding, Robert Gallo, Barre-Sinoussi and others have compromised the "HIV" Vaccine Program:
It was announced in Science that former head of the CDC, Donald Francis, and his company VAXGEN failed in their attempts to produce a new effective AIDSVAX, or "HIV" vaccine. How does Donald Francis know it was a failure! Has he followed every recipient of the vaccine? If not, his pessimism is a form of dangerous and extreme AIDS denialism, to claim that the vaccine was a failure!
In some "HIV" vaccine trials, in addition, it has been claimed that: "HIV" vaccines may appear to help black women more frequently than white women, but the data so far obtained are not statistically significant.(Sort of reminiscent of the Veterans Affairs Trial conducted by Hamilton-The Veterans Affairs Cooperative Study Group reported that, "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians" (JD Hamilton et. al. and the Veterans Affairs Cooperative Study Group. A controlled trial of early versus late treatment with zidovudine in symptomatic human immunodifficiency virus infection. New England Journal of Medicine, 326: 437-434, 1992).
Therefore, isn't it is irresponsible AIDS denialism for Dr. Francis and the other investigators to ignore their "gut?" If those who monitor "HIV" vaccine trials feel that the vaccine helps some black women regardless of what the statistics obtained in the study concluded, then why on earth should Dr. Francis deny and the other investigators deny that AIDSVAX and other "HIV" vaccines did no good, just because there was no "statistical significance?" If this idea that the AIDVAX "HIV" vaccine trial failed is not challenged (a trial that was a true bargain at 120 million), it could deny hope to millions, and compromise the salaries of many hard working "HIV/AIDS" researchers, merely because the numbers are not quite where they should be yet.
Such pessimism (and AIDS denialism) by Francis and others will also serve to erode confidence of the public in the National Vaccine Program. In this regard, I suppose it is of no surprise to "HIV=AIDS" believers, therefore, to find none other than Gallo himself, in the pages of Science, after the so-called failure of the 120 million dollar AIDSVAX program was announced, suggesting that:
"A sound Rationale (is) needed for Phase III HIV vaccine trials (Gallo and others, Science, Vol 303 16 January, 2004)."
If a virus and its associated antigens have been isolated in pure form (A), and when it or some of its components are injected in an inactive form into an antibody-generating immune competent host, an antibody against the virus or components should be produced against the virus or its components (and impurities such as cell membranes). This is the basis for, and reason why, the monoclonal (or polyclonal) antibody industry exists. This process is at the basis of vaccination and the immune response. If "HIV" (A) or some of "its components" ("GP120") is introduced into an immunocompetent host, that subject's immune system (B) will produce antibodies that will neutralize A, so that future exposure will prevent intact virus particles, antigens or components of (A) from destroying or replicating in the immune system (B). Gallo and his colleagues throw all logic and the history of immunology to the winds when he said in this Science article, "A sound rationale is needed for Phase III trials." Are not the principles of antigen and antibody interactions at work for "HIV" as they are in rest of the antigenic universe? This is a more subtle form of AIDS denialism. The logical flaw? Gallo's statement arises from the AIDS denialist idea that the isolated "HIV" antigens are not "immunogenic enough." Try telling that to the millions of "HIV-positives" walking around the planet, that "HIV" isn't immunogenic! This is pure AIDS denialism, and a refutation of the "law of similars" upon which the principle of vaccination is homeopathically based (instead of targeting pathogens directly according to the law of contraries touted by allopathic medicine (AZT, penicillin, etc., directly attack pathogens).
Also, in this Science article, the AIDSVAX trials were criticized by Gallo and his co-authors because they were from the beginning, a colossal waste of time, money, but most of all, as Gallo warns in the last sentence of the letter to Science, the trials are potentially damaging for the credibility (and future funding) of the HIV=AIDS paradigm:
"The decision about whether or not to proceed with mounting a phase III HIV-1 vaccine trial needs to take into account the likelihood of success and the consequences of failure, the value of what can realistically be learned, the human and financial costs involved. As a whole, the scientific community must do a better job of bringing truly promising vaccine candidates to this stage of development and beyond." (Gallo and others, Science, Vol 303 16 January, 2004).
This negative attitude, certainly missed by the mainstream press who should have exposed Gallo's statement as nothing more than an extreme form of AIDS denialism, is a form of denialism that is consistent with the conclusions that AIDS denialists at the AIDS Vaccine Program, SAIC, National Cancer Institute-Frederick Cancer Research and Development Center, Maryland advanced in a published paper, which stated that PHA (phytohemagglutinin) and IL2 (interleukin-2) stimulated healthy {non-infected} cells produce "viral like particles" and HIV 'specific' proteins only when stimulated with PHA and IL-2," and therefore an antigen would be impossible to isolate in pure form in order to evoke immunity, as discussed earlier. Maybe there is a conspiracy amongst these AIDS denialists?
Despite this subtle kind of AIDS denialism becoming entrenched in our National Vaccine Program and by Gallo and his colleagues in the pages of Science due to a lack of vigilance on the part of "HIV=AIDS" supportive editors (who should be reprimanded for letting this slip by), other AIDS denialists have also betrayed their AIDS denialism by advocating that we proceed with worthless "HIV" vaccines that have shown no benefits or which have not been adequately tested for safety, and in many cases, have generated no antigenicity in the vaccinated. These denialists argue that untested "HIV" vaccine programs and strategies should be aggressively promoted and foisted on the general public (not only on black women). For example, in the journal Science, Volume 300, Number 5628, Issue of 27 Jun 2003, pp. 2036-2039, we hear an AIDS-denialist chorus, including, Richard D. Klausner, Anthony S. Fauci, Lawrence Corey, Gary J. Nabel, Helene Gayle, Seth Berkley, Barton F. Haynes, David Baltimore, Chris Collins, R. Gordon Douglas, Jose Esparza, Donald P. Francis, N. K. Ganguly, Julie Louise Gerberding, Margaret I. Johnston, Michel D. Kazatchkine, Andrew J. McMichael, Malegapuru W. Makgoba, Giuseppe Pantaleo, Peter Piot, Yiming Shao, Edmund Tramont, Harold Varmus, Judith N. Wasserheit, singing loudly and vociferously about global vaccine campaigns and strategies for controlling "HIV" and "AIDS." This is irresponsible at best and criminal at its worst. It also may even more strongly suggest that a co- conspiracy of AIDS denialism may exist, like terrorist cells, in which multiple investigators have teamed up to undermine the simple logic of A leads to B leads to C.
I think if we could send about 500 condoms to these hungry folks, that it will make a significant impact on not only the AIDS pandemic, but it will impress many of these AIDS denialists who say the "HIV" vaccine won't work, or will work, or whatever it is these denialists will claim from time to time.
Even Barre-Sinoussi (one of Montagnier's original group) has "come out of the closet," so to speak, with her AIDS denialism. At the Toronto International AIDS conference, she said at the conference:
"It is not clear if therapeutic vaccines might be useful, since 15 trials to date have not demonstrated definitive evidence of improved outcomes."
This is clear AIDS denialism, because, sometimes it takes more than 15 times to isolate just the right antigen from a pathogen to make it evoke humoral, mucosal, or cellular immunity, stimulate a T-cell or two, or prevent disease, as the experience of Pasteur, his 2 assistants, and his 3 vaccines suggested in his anthrax demonstration.
Perhaps this is a job for Homeland Security-to root out these medical terrorists! Or at least serve as a reason to form a "HIV" Truth Commission for HIV=AIDS denialsim and AIDS denialists, as Dr. Wainberg suggested.
But how can we get everybody to take their shots after we send the 500 condoms? Perhaps the best strategies to use are those employed during other recent vaccine campaigns. For instance, if more physicians (especially pediatricians), and pharmaceutical company workers, and vaccine scientists were to inject themselves and their loved ones on T.V., so that everybody can watch (offer their own children as examples of the vaccine's safety in pre-scheduled demonstrations), then wouldn't it stand to reason that the medically ignorant would also line their children up in the vaccination line also to get jabbed? A good idea, perhaps, but the phenomenon of physician non-compliance to vaccination has been known since the early 1980's (From Thomas Levy, MD, FACC):
"Even among the physicians who are the biggest purveyors and promoters of vaccination, it would appear that when the needle is turned around, the inoculation mania subsides. In a study published in the Journal of the American Medical Association, 90% of obstetricians and about 70% of pediatricians refused to take the rubella vaccine. The possibility of "unforeseen vaccine reactions" seemed to have their concern ("Rubella Vaccine and Susceptible Hospital Employees: Poor Physician Participation," Journal of the American Medical Association, (February 20, 1981). Apparently, what's good for the goose is not always what's good for the gander. If these vaccines were truly all they were purported to be, these good doctors should have been pushing each other aside to be first in line to get stuck."
Fortunately, the Bush Administration has recently taken steps to insure that medical disasters do not impede the enormous progress which the vaccinologists are making in protecting the public with "HIV" vaccines that may require too much time to demonstrate efficacy and safety, especially with all of these terrorists running around stealing our anthrax from Dugway Proving Ground, and perhaps other maximum security installations (In a way, it is a good thing that now Don Francis's company is supported through the military, by taxpayer money to make a 857 million dollar anthrax vaccine following the divestment following his unfortunate announcement (and denialism-see above) of the failure of the 120 million dollar AIDSVAX "failed" trial). For example, a "Biodefense and Pandemic and Vaccine and Drug Development Act of 2005" was passed this year in order to alleviate the industrial-medical establishment from impediments such as claims for vaccine or drug damage. As a new directive, the bill amends the Public Health Service Act to enhance biodefense and pandemic preparedness activities, and for other purposes. The bill releases makers and health providers from the following impediments:
"A manufacturer, distributor, or administrator of a security countermeasure, or a qualifed pandemic and epidemic product, described subsection [b,1,A] or a health care provider shall be immune from suit or liability caused by or arising out of: the design, development, clinical testing and investigation,manufacture, labeling, distribution, sale, purchase, donation, dispensing, prescribing, administration, or use of a security countermeasure, or a qualified pandemic and epidemic product
[....]"
"[I]n general, no cause of action shall exist against a person [company] described in subsection a for claims for loss of property, personal injury, or death arising out , reasonably relating to, or resulting from: the design, development, clinical testing and investigation, manufacture, labeling, distribution, sale, purchase, donation, dispensing, prescribing, administration, or use ...in defense against, or in response to, or recovery from an actual or potential public health emergency.."
What is being described here is a total freedom at last to use untested vaccines, pharma products, drugs, or "security countermeasures" carte blanche, because of this Burr-Frist-Bush-Eli Lilly-Big pharma bill. And there is nothing AIDS denialists can do about it because it is in the interests of National Security!
Kevin,
Dyspepsia much? The difference between Dr. Abramson's book and your interpretation of it is, he is firm but positive and constructive. He gives the problems but doesn't say everyone is a shill and a hack and dull etc. He says alot of good things about doctors. He says there are good people and a system with some bad parts. Seems you can't say a good thing about anyone or anything unless it's a book whose message you exaggerate.
Ah, Forty comes back with the LIE defense. If someone has an HIV baby and says she never took drugs she's LYING. I would say she could've been injected by aliens too. But I will leave that line for Andrew. (Does he get paid for writing this stuff?)
Dear 40 mules,
Talk about moving the goalposts! Let me see if I understand your argument.
This was your request:
You made this request because, in your words:
We have provided a prospective study of HIV-infected women in which 59% of children who developed AIDS or died of complications of HIV-1 infection by two years of age were born to mothers with no history of IV drug abuse.
You dismiss this study because you assume that ALL of the women in the study who report no history of IV drug abuse are LYING. You make this assumption because IV Drug abuse is not a socially acceptable thing and therefore they are unwilling to freely admit to it.
Well, the mother of Eliza Jane is in the same boat, isn't she? Our only assurance that she has never abused IV drugs can only be based on her word--just like the women in the study. Eliza Jane developed AIDS despite her mother being a self-reported non-abuser of IV drugs, just like 59% of the unfortunate children in the study.
And EJ's mom deliberately refused to inform the hospital physicians about her daughter's perinatal exposure to HIV, so we know that, even with her daughter's life at stake, she is quite willing to withhold important medical information when it might be considered socially unacceptable.
If we can't take the women in the study at their word, I don't see how we, as objective scientists, can take the word of EJ's mom.
But I will leave that line for Andrew. (Does he get paid for writing this stuff?)
If he does get paid, it must be by the word. I see no other explanation for what he posts.
Is that all you got, Adele? I'm a meanie?
How about responding to the detailed Chapter headings that I listed?
Surely you have favorites of your own, you know, since you enjoyed the book so much?
_____________
The reason I identify you and other posters on this blog as hacks, etc is because that is exactly what you are, and at least, I back up my personal attacks with supporting facts; whereas, all the hacks on this blog always revert to personal attacks IN LIEU of actually addressing the salient facts of the matter. Perhaps, now is a good time to remind everyone of your intial post in the Wikipedia">Dr. Margulis thread from some months back. If I recall you jumped right in with the name-calling and otherwise maligning the character of world-class scientist...all the while without providing so much of an ounce of independent thought.
You, along with all the other regulars on this blog are some of the most intolerant people I've ever encountered -- a real goon squad. Losers, the lot of you ... automatons ...so many adjectives come to mind, but I have only so much time. After all, I'm not here because I enjoy engaging you or Dale or any of the others. I'm here because I almost died as a result of the poor-quality medicine and the corrupt science that corporations have normalized in our society, and this is my way of trying to make sure that others don't have to learn the same hard lessons, the same hard way. My apologies if you find it upsetting that someone is capable of exposing your superficialities, so easily.
Perhaps you should contact one of your sciency friends in Big Pharma about developing a new drug for "thickening one's skin".
Kevin
The correct Dr. Margulis link...
Kevin
Might I suggest that this blog-war be taken to its own web-space. If one is experiencing difficulty locating this space, one may try: forums.wecantgetalongontheinternet.net
I'm having problems taking sides here because I see no inherent value in any winning outcome to this argument. This is a niche site, and the primary product of "winning" (it shouldn't be win/lose anyway, and either case is unlikely with the way things have been going here) the discussion is personal satisfaction.
Furthermore:
1) You could be spending your time studying these things.
2) With the current characters involved in this discussion, one will find themselves in a logic loop similar to the one involved in a theism vs atheism argument (hint: there have been too many beliefs used in this discussion).
3) One will never gain enough headway in any discussion if it is being related personally i.e.: John "Can you present the evidence?" Bob "Yes: your a fag!"
Dear Franklin,
Because Christine, who, according to a book she wrote has tested inconclusive, positive, inconclusive, positive, negative, and positive, and has in effect never tested positive twice in a row, when would you have proposed that her children forcfully be removed from her custody by the state, tested, and then, if positive, or even if one of her children tested as she had but in different order, lets say for argument purposes, Eliza Jane had tested indeterminate/positive,positive,negative, indeterminate, or whatever, when should she have been given those "life-saving meds?" After her slightly high 10,800 T-cell count came down to a more respectable AIDS-defining level of say, 1,500 cells/ul? Or should Eliza Jane have been forced to be tested:
1. Between Christine's first indeterminate and first "positive" test?
2. After Christine's second "positive" test?
3. Between Christine's first negative test and before the second positive test?
4. After the last of the six tests?
Timing is important here, and no child should ever be spared from a good drugging, or from having their "HIV status" known to the government. To bad the mandatory laws were not yet in place, which force everyone to be tested at routine doctor's office visits. (I can't imaging for the life of me how Abbott Labs and all the other 31 test kit makers can ever even hope to be ready to test everybody-its a lot of work to make that many test kits, and even the over-worked and underpaid pharma workers that make them can't be expected to get that many out all at once!
Cheers,
andy
"Internet's Defender" says I'm having problems taking sides here because I see no inherent value in any winning outcome to this argument.
ID the "inherent value" is people's lives and health. Study after study for the past 25 years says HIV causes AIDS, antiviral drugs improve health and save lives and reduce transmission. People who know the facts need to respond to educated people like Andrew who say they're experts when they're not and either know they're lying or are ill. And also to other people like Kevin who is also educated but not in science and has deluded himself into thinking his own illnesses made him an AIDS patient.
That's my perspective. The scientists here are correcting lies as they see them. The denialists think they're doing the same thing. Probably all think they're doing the right thing. Why should this discussion get shut down?
Also, we're learning here. I'm probably the least educated person on this thread and I haven't read some of the papers Franklin and DT and Dale and Chris and Raven gave up there. I know more because I learn from them. Maybe Andrew and Kevin and Forty don't read those papers but maybe they'll remember something from the titles or how people described them.
Kevin, be honest, you call us hacks because we disagree with you. Your suspicion of profit and medical science (based on your sample size of one, ignoring the fact that medical science saved your life) is not evidence against HIV causing AIDS.
---------------
Andrew, when you willfully misrepresent other's words as denialism when it is really just a discussion of details, you are resorting to the tactics of creationists arguing against evolution.
Too bad Robin Scovill and Christine live in Southern California. They'd been perfect for the Padian serodiscordant couple study if they had only lived in Northern California. For instance, it was publicised that Robin had to HIV test in order to keep their son out of the clutches of DCFS, and as expected, he tested negative. Do you see where I am going with this, assuming he had 12 years of what people do in private with his "HIV/AIDS"-diseased wife.
Elisa Jane was a beautiful, beautiful little child, with the smoothest skin, gem-filled eyes, and inquisitive soul. You should have heard her talk about a bug that once got caught in their car's windshild.
Two pictures of Eliza Jane can be seen at:
http://www.justiceforej.com/
At her funeral, Christine and Robin had put together a pictoral of her life from the time of her birth. The "gallery" had some 200-300 photos of the child doing different things. In none of the images does the infant or child appear ill. She just had too many lymphocytes, and was gaining weight (and size) steadily throughout the pictoral history. To accuse this family of ever having shown their children anything but love and complete engagement, to those who knew them, would be the greatest and saddest chapter in our civilization's history.
To Adele,
You bet I will at least remember the titles. Kind of like a "slow" child, and repetition is really the best way for me to go.
EG ICL AIDS is simply AIDS without any "HIV" in it.
Some children die of too many absolute lymphoctes.
Old drugs developed for cancer are good for the immune system.
Dogs, sheep, goats, chimps, macaques, and humans test positive for "HIV," but only humans die in 13 years (with the current miraculous drug cocktails.
Damn virus mutates every 60 seconds, but in doing so, only mutates genes that do not interrupt its deadly sting, and of course, mutation is why people don't respond to AZT (see my blog above by TAG's Harringon).
I suppose that Eliza Jane could have at least lived at least to age 16 if only...if only....she would have been put on HAART, if what you state above, that HAART has extended life an average of 13 years (or in Norway to 35 years some one of you said?). So show me the study that says 35 years on HAART is safe and effective, and should have been aggressively promoted in the case of the daughter of an inconsistently testing mother, who can't infect her husband, and who has never been ill herself.
I concede, you are right, and I will remember all you have discussed.
Cheers,
Andy
Dogs, sheep, goats, chimps, macaques, and humans test positive for "HIV," but only humans die in 13 years
Ignorant, lying or deliberately misleading. Only humans, chimps and macaques test positive for HIV and for the latter two species there is no evidence of infection outside of the laboratory.
...based on your sample size of one, ignoring the fact that medical science saved your life... -- Robster
You don't read well, either, apparently. As I've noted numerous times, I know of many others with similar health histories to my own. Thank you, internet. How do you think I found the doctor who helped me. After all, I had to travel 400 miles, out of state to get the care that I needed. Conventional medicine nearly killed me! My primary care physician gave me more antibiotics during my final visit to that moron, which is of course the very worst thing one can give to someone with severe candidiasis.
Incidentally, the doctor who finally knew what he was doing -- namely he knew how to treat severe candidiasis -- well, he no longer accepts any insurance because he realizes just how much it compromises care options, completely to the detriment of his patients. None of the numerous HMO doctors that I saw would prescribe the diflucan, at the dosage I needed. Their hands were either tied by the HMOs or they were too arrogant to consider my situation properly and prescribe the medication "off-label".
You make statements that show a serious lack of comprehension, Robster and then you wonder why someone calls you a hack.
I've never stated that all modern medicine is to be avoided. Unlike you, I've been very pointed in discussing the limits of modern medicine, both the good and the bad. Something you are too much of a boot-licker to understand. Regardless, I'm certainly not the only HIV-negative Aids case, and I surely won't be the last as long as drugs and more drugs are the only treatment option.
Your sense of denial is evident, Robster and absolutely unbelievable.
Kevin
...and was gaining weight (and size) steadily throughout..
Technically correct. She wasn't shrinking but from birth she steadily dropped in weight percentiles from the 30th percentile to below 3. There was a jump in weight between her last weighing and when she ended up in hospital however this was hardly healthy growth as it consisted of extravascular fluid being retained.
I don't doubt that Christine loved her child and did what she thought was best for Eliza-Jane. That doesn't change the evidence that indicates that Eliza-Jane died from PCP and AIDS.
Numerous people have pointed out to you that AIDS is characterised by the depletion of a specific subset of lymphocytes. Numerous people have given you specific papers that demonstrate that PCP, low CD4+ counts and high total lymphocyute counts are not inconsistent. It's hard to understand whether you are simply incapable of understanding this or whether you just pretend to be stupid/delusional.
PS. Before you cherry pick Barre-Sinoussi you could learn the difference between preventive and therapeutic vaccines. They aren't the same thing.
Kevin, If you are trying to tick me off, you need to try a lot harder, especially since I don't care what you think about me. I don't wonder why you call me a hack (I disagree with you, that seems to be reason enough, let alone pointing out when you are wrong).
Conventional medicine didn't nearly kill you. The disease organisms were what was killing you. A doc who wasn't up on his differential diagnosis certainly didn't help, but you found a doc that was. That one gave you the conventional medical treatment that you admit saved you. Your statement that you had HIV free AIDS is a violation of the clinical definition of AIDS. Having any of the OIs associated with AIDS does not mean you have AIDS.
Beyond that, does your having met others like you via the net increase your sample size to anything significant compared to HIV/AIDS studies? Or does it demonstrate that a rare immune suppression disorder can initially be mistaken for a more common syndrome?
I'm no fan of HMOs. Do you think I want a bunch of bean counters making medical decisions? No thanks. I want a single payer system, and one that makes prevention profitable instead of a loss leader.
What I don't want is magic, woo, alternative medicine or denialism (such as HIV/AIDS denialism, germ theory denialism or antivax nuttery) passed off as legitimate medicine. If that makes me a hack in your eyes, so be it.
Andrew,
Thanks for the concession. I think you should make it your new mantra. Repeat it in front of the mirror 10 times every morning before shaving.
What's most impressive to me is that when your blatant misrepresentations of the scientific literature are explicitly pointed out, your response is to retreat into a paranoid fantasy world where I'm asking for a child to be forcibly removed from her parents.
You're getting so incoherent you can't even keep straight the difference between a lymphocyte and a T-cell:
Her total lymphocyte count (TLC) was 10,800--, as pointed out on June 9 by Richard Jefferys, that means her T-cell count had to be lower (unless she completely lacked B cells, and NK cells).
Furthermore, as has been pointed out previously EJ's TLC was not measured under circumstances that in any way approximate those of the outpatient studies you cite. According to the coroner's report (p. 21) the blood specimen was obtained at 2:40 AM--only 3 hours before her death from untreated Pneumocystis pneumonia--and after EJ had already required CPR on three separate occasions after collapsing pulseless at home at 12:03 AM. The possibility that her blood profile might be altered by the extremely severe infection of her lungs and the heroic measures taken to try and save her life should occur even to you.
There is only one reason why EJ's CD4 T-cell level wasn't determined while she was alive--her parents refused to even consider checking it. It is the height of hypocrisy for you to complain that the coroner hasn't produced all of the standard tests used to work up an HIV infection, given that the girl's parents and pediatrician had 3 ½ years to get the testing done and refused. The coroner's job is to determine the cause and manner of death. He did that. Now that EJ is dead, the coroner can't make up for the inadequate health care provided by her parents and the Quacks they sought out to be EJ's doctors.
The following reports explain why only 40% of drug users will self report on a medical history form. One of the reasons for this is that in many jurisdictions, this Intra Uterine Drug Exposure is reported to state or local authorities and may result in the mother's losing custody of her baby. Again as I have stated previously, all pediatric AIDS studies take place with inner city hospitals on poor, mostly black IV drug users, and hard drug users.
So far, none of the (as Kevin says) hacks, here, have been able to provide a citation to a single study in the medical literature of white suburban nondrug user mothers with AIDS babies to refute my statement. The syndrome called pediatric AIDS, is in fact, maternal/fetal drug use, addiction/withdrawal. The administration of cytotoxic drugs to this group is a medical experiment which should be halted and those responsible held accountable.
Clinical Chemistry. 1997;43:235-242
http://www.clinchem.org/cgi/content/full/43/1/235
Detection of intrauterine illicit drug exposure by newborn drug testing Tai C. Kwong and Rita M. Ryan
Intrauterine cocaine exposure has also been associated with an increased risk of prematurity, small for gestational age status, microcephaly, congenital anomalies including cardiac and genitourinary abnormalities, necrotizing enterocolitis, and central nervous system stroke or hemorrhage. Infants born to mothers using amphetamines have many of the same problems as cocaine-exposed infants, including increased rates of maternal abruption, prematurity, and decreased growth parameters such as low birth weight. In addition to an increased risk of prematurity and being small for gestational age, striking withdrawal symptoms often requiring treatment are frequently observed in infants after in utero opioid exposure. Symptoms include irritability, hypertonia, wakefulness, jitteriness, diarrhea, increased hiccups, yawning and sneezing, and excessive sucking and seizures, with onset of withdrawal earlier in heroin-exposed babies compared with methadone-exposed infants. Some intrauterine cocaine-exposed infants may manifest symptoms of withdrawal including hypertonicity, jitteriness, and seizures. Intrauterine amphetamine-exposed infants may also have similar postnatal symptoms including hypertonia, tremors, poor feeding, and abnormal sleep patterns. Long-term follow-up of IUDE infants suggests that in addition to the potential for difficult social situations, such as increased risk for child abuse and neglect, abnormal neurocognitive and behavioral development may occur, as well as an increased risk of sudden infant death syndrome.
Drug testing is one of the only methods of identification of IUDE . Maternal history of drug use is often unreliable. If identification of IUDE infants is worthwhile, it is inadequate to rely on maternal self-reporting; for example, 24-63% of mothers with positive cocaine tests deny cocaine use.
In addition, in many jurisdictions, a physician caring for a newborn suspected of IUDE is required to investigate and report the findings to the appropriate authorities. A positive maternal history of drug use or the demonstration of drug in maternal urine may not constitute sufficient evidence to indicate a report to child protective services. Definitive documentation of the presence of drug in the baby may be required.
The documentation of the presence of an illicit drug in a newborn can be challenged by the mother or the family. Moreover, in many jurisdictions, reporting of the finding to state or local authorities is mandatory and, although infrequent, may result in the mother's losing custody of her baby.
Int J Gynaecol Obstet. 1991 May;35(1):51-4 Peripartum cocaine use: estimating risk of adverse pregnancy outcome.Cohen HR, Green JR, Crombleholme WR.
http://www.ncbi.nlm.nih.gov/sites/entrez?cmd=retrieve&db=pubmed&list_ui…
Pregnancy outcome of 83 patients with a positive urine toxicology screen for cocaine in the third trimester were reviewed. The outcomes of pregnancies complicated by cocaine abuse were compared to those of matched controls selected from our general obstetric population. We observed a statistically significant increase in the incidence of premature separation of the placenta, low birthweight infants, preterm deliveries, and the incidence of fetal distress requiring cesarean section. On admission, 55% of patients denied recent cocaine use.
Am J Obstet Gynecol. 1990 Sep;163(3):797-801
http://www.ncbi.nlm.nih.gov/sites/entrez?cmd=retrieve&db=pubmed&list_ui…
Prevalence of use of cocaine and other substances in an obstetric population.
Matera C, Warren WB, Moomjy M, Fink DJ, Fox HE.
Increasing use of cocaine among pregnant women has been reported. This study was conducted to determine the prevalence of positive urine toxicologic screens for cocaine and other substances of patients admitted to the Sloane Hospital for Women. Urine samples were obtained from 509 women admitted to the delivery suite. The overall prevalence of cocaine was 10% (n = 51). Cocaine use was 10 times more prevalent in the clinic population (14%) than in the private population, (1.4%). In addition, women whose urine samples were positive for cocaine were more likely to have no prenatal care, previous induced abortions, to be human immunodeficiency virus-positive, and admitted previous use of cigarettes, alcohol, cocaine, and other drugs. Amphetamines were detected in 13% (n = 65) of patients. However, the screens did not distinguish between metabolites of amphetamines and other drugs such as cold medications. The medical history alone predicted only 37% (n = 19) of the cocaine-positive screens and none of the amphetamine-positive screens.
end quote
Discussion of HAART toxicities which would then be added to the pre-existing problems of drug addiction/withdrawal in the baby. See this site;
http://hivinsite.ucsf.edu/InSite?page=kb-03-02-06
Goalpost moving alert
....please provide a reference in the medical literature to any newborn pediatric AIDS study in which the mothers ARE NOT I.V.DRUG USERS
So far, none of the (as Kevin says) hacks, here, have been able to provide a citation to a single study in the medical literature of white suburban nondrug user mothers with AIDS babies to refute my statement.
Now apparently the mothers have to be white and suburban too. Any more caveats? Should they also be anti-vaccination vegans too?
The administration of cytotoxic drugs to this group is a medical experiment which should be halted and those responsible held accountable.
Are you incapable of reading the articles that have been cited? I'll quote again from one of the studies.
The majority (71.3%) of AIDS diagnoses and deaths occurred in untreated children. Fewer than 6% of children receiving NRTI only, dual NRTI, or PI therapy during the 0-6 month age period met the endpoint compared with 19.7% of children not receiving treatment (Table 4).
Simply compare the outcomes of the babies that received ARV and those that didn't. How can you explain these results? Wouldn't your theory predict a higher mortality in those given ARVs?
Most of the HIV/AIDS establishment as well as some in the gay community, and the pharmaceutical industries that make "AIDS drugs," have increasingly regarded the questions, efforts, empirical, and homeopathic ideas of Christine Maggiore, Robin Scovill, and other "HIV/AIDS" question-askers as a threat to the rationalist, reductionist, and allopathically-focused "HIV/AIDS" practices and public health policies, as well as perhaps, an economic threat to pharmaceutical profits. By law, it is mandated that "HIV/AIDS" is a reportable disease. Those who raise issue with "HIV/AIDS dogma" or public health policies are often regarded and treated as enemies of the medical and scientific community. For instance, "HIV/AIDS" critics have been called "Holocaust deniers," "flat-earthers," "irresponsible," and "criminal." From the beginning of the AIDS era, the AIDS establishment, backed by the federal government and Epidemic Intelligence Service, has attacked those who question any of the accepted AIDS axioms or dogmas with increasing hostility, censorship, and legal consequences. Recently in Maine, Oregon, Massachusetts, and Canada, the children of parents who test "HIV-positive" and who refuse "AIDS medications" for their children, have been taken away by the state. Parents in some instances have faced legal retribution. In New York at Incarnation Children's Center (ICC), an NIH and GlaxoSmithKline-funded trial was conducted in which it is documented that some children who refused to take their medications, or were too young to easily manage were force fed antiretrovirals through G-tubes surgically implanted in their stomach (4, 5). Upon threat of court martial and military prison, since 1990-91, military inductees were forced to be immunized with an ineffective "anthrax" vaccine, and perhaps other experimental vaccines (such as AIDSVAX), that are known to contain dangerous autoimmune syndrome-inducing adjuvants (because the vaccines don't work), during Operation Desert Storm (6). Apparently, during the early 1990's, this experimental program was overseen by Dr. Edmund Tremont, a powerful figure in the AIDS establishment.
The sudden and antibiotic-associated death of child of a mother who had previously questioned "HIV/AIDS dogma" and public health policies regarding "HIV/AIDS" has presented a formidable medical, social, and political conundrum for some in the HIV/AIDS establishment. However, Christine Maggiore is not alone. There are now thousands of scientists including several Nobel Laureates, National Academy members, physicians, scholars, journalists, and people living with "HIV/AIDS" throughout the world, who do not believe that scientific, medical, or epidemiological evidence supports the hypothesis that "HIV causes "AIDS," that "AIDS" is a transmissible syndrome, or that "HIV" is an exogenous retrovirus that has been correctly isolated (see http://aras.ab.ca/rethinkers.htm; http://www.virusmyth.net/aids/statement/).
They believe instead that profound immunosuppression is caused by a myriad of factors and that it is incorrect to group these syndromes under a single disease entity, "HIV/AIDS." The consequences of this view suggest that different treatment strategies are needed for the spectrum of the 46 previously known "AIDS-indicator diseases," rather than the toxic and dangerous pharmaceutical or vaccination approaches currently in place.
In the aftermath of the tragic death of Eliza Jane, and many other high profile cases that were said to have died of "AIDS," the AIDS establishment could have chosen one of two paths to improve Public Health policies regarding "HIV/AIDS patients." 1) Initiate a non-pharmaceutical company backed scientific investigation with an open and critical look at the accuracy of the so-called "HIV tests," the efficacy and safety of the so-called "life saving AIDS medicines (regardless of the fact that not one of their package inserts claims that they are "life saving" or even that they have been tested for safety or efficacy) and begin an investigation as to the scientific credibility, accountability, ethics, and motives of leading AIDS researchers who were accused of fraud and scientific misconduct at the beginning of the AIDS era (7), and investigate AIDS program leaders such as Edmund Tremont, who openly admitted to changing safety reports in Nevirapine drug trials last year because he "knew better" than other AIDS scientists and drug-trial safety officers about "AIDS" (8). Or, 2) the tragedy of Eliza Jane's death could present a golden opportunity for some in the "HIV/AIDS" establishment to even more vigorously attack those who ask questions regarding the current "HIV/AIDS" paradigms, axioms, and policies, by mounting a politically motivated, highly publicized, quasi-religious, and Inquisition-style Salem witch hunt for Christine Maggiore and Robin Scovill, because they have dared to question AIDS dogma, and therefore have threatened, the "HIV=AIDS" establishment.
4. Revision of autopsy findings:
Predictably, and in retaliation for asking questions, or for never consistently testing "HIV-positive," and perhaps at the most vulnerable moment in the lives of any parents, The public health officials were somehow made aware that a reappraisal of Eliza Jane's "indeterminate" autopsy findings by the LA coroner's office was in order, to determine if the parents should be prosecuted, and their other child aged 8, taken away by The State to be "HIV" tested, and perhaps fed antiretrovirals.
The new autopsy analysis was performed by Dr. Chanikarn Changsri of the LA coroner's office, and Dr. Maurice A. Verity, a neuropathology consultant from UCLA who was asked to 'help her' interpret 'the new neuropathology findings'. Also, another LA coroner, Dr. James Ribe, was summoned in to oversee Dr. Changsri's and Dr. Verity's report. Dr. Ribe has been under investigation by the LA Appellate Court, and other legislative bodies, for his seriously flawed and fraudulent autopsy findings in at least 5 well-documented cases that led to child abuse and murder convictions of parents. For example, in 1996, an autopsy report he wrote led to the life time convictions of the Jacobo parents for findings he felt consistent with child sexual abuse and murder, but which after reappraisal, appeared consistent with a inherited vitamin deficiency, which has led to the release of the father but not the mother, who is still in prison for life (Case No 95-09550). Other examples of Ribe's alleged criminal misconduct can be found at http://www.justiceforej.com/ribeflipflops.html.)
Four months after the autopsy and case reassessment was ordered, on September 15, 2005, Dr. Changsri, Dr. Verity, and Dr. Ribe concluded in their autopsy report and press release to the LA times, that Eliza Jane actually died of end-stage AIDS-related Pneumocystis carinii pneumonia (PCP), and that the child suffered from p24-positive brain encephalopathy due to the ravages of "HIV," despite her almost twice normal lymphocyte count of 10,800 lymphocytes/µl.
Trauma, physical abuse, or chemicals known to render the acute symptoms consistent with the 36 hour temporal sequence of Eliza Jane's death were eliminated through scans at VPH hospital, and at autopsy (1,2). On May 16, 2005, blood analysis at VPH showed that her lymphocyte count was high. The analysis showed that she had 10,800 lymphocytes/µl (normal=2000-8000 lymphocytes/µl) (2). Her hemoglobin and hematocrit counts were low (hemoglobin=6.3 g/dl instead of 12-16g/dl, and hematocrit=21% instead of 37-48%, respectively). (2). Her neutrophils were measured at 12% (normal=45-74%) (2). Her monocyte percentage was in the normal range at 8% (normal is 4-10%) and her platelet count (214 k/µl) was in the normal range (130 k/µl -400 k/µl) (2). The revised autopsy revealed that she had pericardial and pleural effusion and ascites attributed to PCP pneumonia, that her lungs, heart, liver, and kidneys were significantly increased over the expected average weight for her age (184%, 131%, 121%, 146% of normal), that her liver was significantly enlarged and the hepatocytes showed micro-and macrovesicular steatosis. that there were non-specific microscopic lesions in the brain consisting of microglia, multinucleated giant cells, and p24 protein staining, and that her bone marrow showed atrophy, as did her thymus and spleen. These findings differed significantly from "no cause of death" detected by the coroners before they had become aware of the mother's viewpoints on "HIV/AIDS."
5. Enter the media:
The new finding of PCP pneumonia and "HIV"-encephalopathy were immediately made available to the LA Times by the coroner's office without the consent of the parents. The findings, in addition, were presented by the LA Times and more recently, by ABC Primetime, to insinuate heretical wrong doing on the part of the parents and pediatricians. In the first of many inflammatory articles that came out coincident with the release of the revised autopsy report of Dr. Changsri, Dr. Verity, and Dr. Ribe, entitled "A mother's denial: a daughter's death," The LA Times went into great detail alluding to how Christine Maggiore barbarously gave birth to her two children at home, refused the Holy Waters of infant vaccines, and unconscionably breast fed her children. It described how one of her three pediatricians defended his daughter, who was a accused of being a Madame involved in prostitution, and worse, how Christine never had the children tested (9), to see if they would test as she had: positive (the first one), indisputably positive (the second one), inconclusive (the third one), positive (forth one), negative (fifth one), and positive (sixth one).
6. Parents and pediatricians under investigation, and threats to remove her other child:
Predictably, and due to the coroner's revised findings and recommendations, the parents were placed under investigation by The Department of Children and Family Services, the LA police department, and the media. The pediatricians are now being investigated by the State Medical Board. To protect the unity of their family, Christine Maggiore and Robin Scovill immediately arranged to have their 8-year old son Charlie "HIV"-tested multiple times by their pediatricians, and presented with consistently negative results. The 8-year old is still living at home with them.
Franklin said: We have provided a prospective study of HIV-infected women in which 59% of children who developed AIDS or died of complications of HIV-1 infection by two years of age were born to mothers with no history of IV drug abuse.
You dismiss this study because you assume that ALL of the women in the study who report no history of IV drug abuse are LYING. You make this assumption because IV Drug abuse is not a socially acceptable thing and therefore they are unwilling to freely admit to it.
I have provided citations to medical studies of drug users which reveal that only 40% of drug users will self report on a medical history form. One of the reasons is that this informatin is reported to authorities and may result in the mother's losing custody of her baby. Notice how a typical AIDS apologist, franklin, twists this information into the defensive statement that these women are being unfairly accused of LYING. Of course they are lying, in order to maintain custody of their baby. I would have no hesitation in LYING in the same situation.
Not only are these women lying, if they could, they would stay away from the inner city hospital and medical system which is harmful to them and their babies. Administering toxic drugs to a mother and unborn baby is sheer folly and a crime which must be halted.
Regarding the miraculous saving of drug addicted babies lives with toxic drugs, this is a delusion created by the twisted logic demonstrated in a few of above replies. In fact, there are no sanely carried out clinical trials comparing toxic drugs to placebo in maternal or pediatric AIDS, and any statement that these drugs are lifesaving or miraculous is essentially another LIE. The nevirapine trial is an example of the type of lying and corruption that take place in these types of drug studies. Ask Dr. Jonathon Fishbein, the NIH whistleblower about it. In fact, HIV negative babies born from drug addicted mothers have a high mortality in the first 6 months and then do quite well from 6 months on, which is the same profile for babies of drug user mothers who test HIV positive.
Kevin is absolutely correct in his statement about corruption in medical research, the current state of conventional medicine, and his estimation of this blog.
It should be obvious to the lurkers by now that there has been a deafening silence here in the inability to cite a single pediatric AIDS study in which the mothers were not mostly black, poor inner city hard drug and IV drug users. The only reply above is to joke about it, which tells the lurkers that the argument has been lost.
The HIV causes AIDS hypothesis is under serious re-examination by taxpayers who want an accounting of the billions wasted on this project. It's time to stop the phoney medical studies on poor inner city black drug users and all the other self serving wasted HIV/AIDs science projects, and divert the hard earned taxpayers dollars to real projects elsewhere.
For more information see
www.reviewingaids DOT com
www.livingwithouthivdrugs DOT com
Hey Forty Mules,
I think your almost getting the point when you say:
The unfairness arises not from your skepticism that a woman with an HIV-infected child might lie about IV drug abuse, but from your applying this standard only to women who seek care at "inner city hospitals" and not to EJ's mom, even though--as the girl was dying--she lied to health care workers about EJ's perinatal exposure to HIV. If a child acquiring HIV from her mom equals IV drug abuse in your world view, it should mean the same thing whether the mom is Black, White, or Hispanic.
Sounds like racism to me:
Poor Black and Hispanic women report never using IV drugs--they must be lying.
Rich white suburbanite reports never using IV drugs--she must be telling the truth.
I guess when logic fails you, you are willing to stoop to the lowest forms of argument--even racism-- just to stay in the debate.
How do you explain the case of Ariel Glaser, a child who died of AIDS despite having a rich white mom who didn't use drugs?
Forty Mules, do you realise you are accusing Christine Maggiore of being a drug user and lying about this and her other circumstances to keep custody of her surviving child?
Forty, Dale asked you to look at Yoon J.J. et al a few days ago. I'll assume you haven't so here is a quote from the abstract
In addition, maternal drug usage was evaluated using maternal history and toxicological screening of maternal blood and urine and newborn blood, urine and meconium
That "toxocological screening" of blood part is the same thing you see in alot of papers on this topic where it's called "phlebotomy".
Forty assumes every single mother with an HIV + baby except white suburbanites is a drug user. Every single one who doesn't admit it is lying. Forty people can lie all day long but their blood can't.
How do you explain these with drugs?
1. Some HIV + babies are NOT born to drug using moms and this is confirmed by blood tests not just questions.
2. Almost all babies of drug using moms are NOT HIV positive and don't get AIDS.
3. The one thing always there in pediatric AIDS is HIV in the mother and that's with or without drugs.
Kevin,
Did you give an interview recently? I heard a guy on the radio a few days ago talking about how antibiotics gave him severe candidiasis and how he had "AIDS without HIV" and how doctors have failed. Just wondering. Interesting interview though.
Hopefully he'll correct me if I'm wrong, but I think Kevin also has a website called "NotAIDS" (if it's not Kevin's, it certainly promotes similar views about fungal overgrowth being the cause of AIDS).
Also, Kevin wrote:
Conventional medicine nearly killed me! My primary care physician gave me more antibiotics during my final visit to that moron, which is of course the very worst thing one can give to someone with severe candidiasis.
Are you sure this was entirely the doctor's fault? Back in 2004, you wrote the following about your fondness for antibiotics:
http://groups.google.com/group/alt.med.allergy/browse_thread/thread/8df…
"Just wanted to say that I am very excited (and grateful) for the opportunity to try a more natural approach to treating my chronic sinusitus. I am currently experiencing my second sinus infection in 6 weeks and taking another course of antibiotics.
A little more history...
My infections generally respond well to antibiotics, meaning I feel much, much better after 3 days or so. By the end of two weeks of treatment with antibiotics, I usually feel as though I am totally clear. This is a new response, only achieved since I had surgery almost one yr ago today (jan 03). Before the surgery, antibiotics helped with acute symptoms but I never felt fully well. I would get an infection every 3 months, like clockwork. I felt great after the surgery and only had my first infection 6 months later. Now, I am beginning to experience the chronic symptoms again (i.e. never feeling fully recovered).
I am quite educated on the subject but I haven't heard of using H2O2 as a treatment. generally, I tell any doctor I see what works and what doesn't for my particular situation; they basically do whatever I suggest re: antibiotics and other treatments. (I did see a doc recently who wasn't familiar with my history, who tried to tell me that antibiotics would do nothing for me. After much arguing, I cut a deal explaining that I would return in two weeks and educate him on just how necessary antibiotics were for acute exacerbations of my chronic condition. I plan to call him tomorrow). I am halfway thru a Biaxin regimen and feel almost well, but I know it is only temporary. Currently, I cannot even go out to a bar that is at all smoky without developing a sinus infection a few days later. I will begin the H2O2 irrigation tonight and keep you posted.
Thanks for such a thorough explanation of the procedure.
Regards
Kevin"
Hopefully he'll correct me if I'm wrong, but I think Kevin also has a website called "NotAIDS" (if it's not Kevin's, it certainly promotes similar views about fungal overgrowth being the cause of AIDS).
Not my website. Once again, you've proven to be quite the presumptuous cretin, Mr. Jeffreys. I don't maintain any "personal" website. I don't have the time nor the inclination.
_____________________________
Now, "the post from the past" that you quote here is indeed mine. However, it is not inconsistent with what I have posted here. My views have certainly changed, but that is exactly what I've stated numerous times. Thank you for providing an example that illustrates just how my views have changed. Consider:
My infections generally respond well to antibiotics. (I've never denied that antibiotics were sometimes useful for me. However, the results were always temporary. They would help with the acute bacterial-related symptoms, but I was unaware, at that point, that they were making my underlying ill health worse because they were exacerbating my fungal problems-- which were soon to get much worse.) This is a new response, only achieved since I had surgery almost one yr ago today (jan 03) (The surgery was indeed helpful, but the effects were also temporary). Before the surgery, antibiotics helped with acute symptoms but I never felt fully well. I would get an infection every 3 months, like clockwork. I felt great after the surgery and only had my first infection 6 months later. Now, I am beginning to experience the chronic symptoms again (i.e. never feeling fully recovered). (I haven't taken an antibiotic in almost 2 years. Yet, I can now say that I feel fully recovered)
As this post indicates, I was actually very uneducated as to what was really wrong with me. Once again, I had no idea of the role that frequent antibiotic use was playing in my poor health.
Continuing:
I am quite educated on the subject but I haven't heard of using H2O2 as a treatment. (Again, I guess I wasn't quite as well-educated on the matter as I thought. Incidentally, the peroxide treatments were helpful but too painful to endure) generally, I tell any doctor I see what works and what doesn't for my particular situation; they basically do whatever I suggest re: antibiotics and other treatments. (So sad but so true...my opinion here has changed little, for even though I still had almost full-faith in modern medicine at this point, I realized early on that most of my physicians were not equipped to help me. I just didn't understand the "why". Regardless, my overall health was not improving. I thought I needed the antibiotics, and apparently, so did they) (I did see a doc recently who wasn't familiar with my history, who tried to tell me that antibiotics would do nothing for me. After much arguing, I cut a deal explaining that I would return in two weeks and educate him on just how necessary antibiotics were for acute exacerbations of my chronic condition. I plan to call him tomorrow). (I wish I would have listened to this doctor, he was fairly intelligent but he moved shortly thereafter. I would like to know just how much he knew about what would work but he moved before I learned of the fungal connection to my health problems)
____________________________________
Your attempt to malign my credibility has failed; however, such an attempt is indeed splendid detective work for it is very revealing about your character, Mr Jeffreys. You have consistently proven to be a smarmy and unctuous fellow, whose intentions are ignoble. I have posted on this blog numerous times that I have only recently realized how dysfunctional our health care system is-- recently being the last few years, as this "post from the past" corraborates. In January of 2004, it's safe to say that I had a fair amount of faith in the system; however, my health declined rapidly that Spring which is when I was diagnosed with my first AIDS-defining condition, esophageal candidiasis, which is why I never posted a corrected analysis on that site. By the Spring of 2004, I was suddenly too sick to focus on anything but survival. If anything, this "post from the past" offers further proof of the truth of my story, including my history of frequent antibiotic use and the incompetency of my caregivers.
_____________________________
And now for the best part ... as I've also posted on this blog at least one other time, my discovery of the following Mayo Clinic study was the eye-opening experience that changed everything (in addition, to my struggles with esophageal candidiasis):
Mayo Clinic Study Implicates Fungus As Cause Of Chronic Sinusitis
Since you've proven to be quite the detective, Mr. Jeffreys, why don't do some follow-up research on this Mayo Clinic study and report back to all on this blog. If you do, you'll discover that two subsequent studies have confirmed the findings of this initial study (from 1999!), namely that over 96% of chronic sufferers overwhelmingly respond to anti-fungal treatment; yet, the treatment standards for this condition have not changed. Why is that, Mr. Jeffreys? Perhaps, you and your pal Robster would both like to answer that question for the gallery.... For me, that was last straw. I quickly realized just how severely corrupted medical science had become and just how lucky I was to be in a position to figure it all out before I died.
Thank you, Mr. Jeffreys.
Thank you for bringing this further evidence to everyone's attention. The proof is indisputable. I am extremely healthy now and that change is due solely to overcoming my severe fungal problems, aka AIDS. After enduring the candidiasis, PCP, histioplasmosis, and a host of other OIs, anyone who knows me can attest to the marked turn around in my health; Such a change is not coincidental. One added bonus of good health is that my mental acumen has increased ten-fold, so I have plenty of energy to combat insidious people like you, Richard Jeffreys. So keep searching...my intentions are just, and I stand by any and all comments that I have made because they were all made in good faith. Can you say the same?
Lastly, I will continue to participate in these discussions, so that perhaps others will not have to suffer through the unpleasant trial and error medical processes that I, thankfully, survived.
Kevin
Ps
No, Adele, I have never given an interview, radio or otherwise, regarding my views on antibiotic use and it's relationship to candidiasis.
Kevin,
The Mayo Clinic paper is very interesting but life changing? The findings are compromised by this:
Interestingly, the control group of normal, healthy volunteers was 100% culture positive for fungi.
96% of chronic sinusitis people had positive fungal cultures but 100% of healthy controls had positive cultures. They found an avg 2.7 organisms per person in the sick group and 2.3/person in the healthy ones. It's not a significant difference because there were just 14 healthy people and 210 who were sick.
So everyone has fungus and gets exposed to fungus. That's what the study says. The rest you can agree with or not but fungus itself obviously isn't the culprit. Something has to cause an immune breakdown for the fungus to cause problems. In AIDS its the presence of HIV. Sometimes its immunosuppressive drugs. In Kevin's case, we don't know, maybe too many antibiotics.
Some MDs Dibbern and Dreskin wrote in to the Mayo journal in Jan 2000 and said this,
The authors have done an excellent job to raise awareness of this syndrome and encourage careful handling of nasal secretions and pathologic specimens for fungal isolation. However, we doubt that such a high percentage of chronic rhinosinusitis (CRS) cases, 93% of 101 consecutive surgical cases as reported in this series, are caused by this disorder. Importantly, the authors note that 100% of 14 normal volunteers had fungal culture-positive nasal washings, as did 96% of 210 patients with CRS, limiting the importance of this finding. Thus, fungal colonization per se adds little positive predictive value for AFS.
Dibbern and Dreskin say Morpeth JF, Rugg NT, Dolen WK, Bent JP, Kuhn FA. Fungal sinusitis: an update. Ann Allergy Asthma Immunol. 1996;76:128-139 gives the guidelines for diagnosing fungus involvment. 1996 I think was even before 1999.
What about the two follow-ups with 96% results?
I guess Ponikau et al J. Allergy Clin. Immunol. 2002 Dec;110(6):862-6. is one. They see 75% although Kevin said 96% patients with improvement in symptoms. Amazing but there's no control. A Dr. Ferguson write in next May and asks Antifungal nasal washes for chronic rhinosinusitis: what's therapeutic-the wash or the antifungal?
I couldn't find the other one, maybe Kevin can send it.
But I did find these,
Kennedy DW et al Laryngoscope. 2005 Oct;115(10):1793-9. "Treatment of chronic rhinosinusitis with high-dose oral terbinafine: a double blind, placebo-controlled study."
Conclusion: the antifungal didn't help the patients
Weschta M et al Arch. Otolaryngol. Head Neck Surg. 2006 Jul;132(7):743-7. "Effect of nasal antifungal therapy on nasal cell activation markers in chronic rhinosinusitis."
Conclusion: Amphotericin B (what Kevin's people used) didn't help anyone.
Helbling A et al J Laryngol Otol. 2006 Dec;120(12):1023-5. Epub 2006 Sep 11. "Amphotericin B nasal spray has no effect on nasal polyps."
Conclusion: didn't help.
Ebbens FA J. Allergy Clin. Immunol. 2006 Nov;118(5):1149-56. "Amphotericin B nasal lavages: not a solution for patients with chronic rhinosinusitis."
Conclusion: obvious. I'll just say this was a placebo controlled study and there wasn't a difference between placebo and antifungal.
Kevin, I don't say fungus isn't important it obviously is and I'm not saying the Mayo clinic study is really bad either. I'm just saying you are taking one little piece of information and turning it into your life. Like the HIV positive person keeping everything under control with HAART and then some idiot tells them the drugs are toxic and they stop. I'm glad you're healthy. But why use your misunderstanding of medicine to convince others to stop getting treatment?
One more paper, this one's from Andy's favorite journal,
Eby GA Med. Hypotheses. 2006;66(4):851-4. Epub 2006 Jan 10.
"Strong humming for one hour daily to terminate chronic rhinosinusitis in four days."
Hmmm.
Hmmmmmm.Hmmm.Hmmm.
Kevin,
Administering toxic drugs to a mother and unborn baby is sheer folly and a crime which must be halted.
Everything is toxic, depending on the dose. Giving pregnant mothers any drug, by your logic, would be a crime. In the case of in utero transmission of HIV, antiretrovirals can prevent the kid from getting HIV. HAART leads to extended lifespans for AIDS patients, so some toxicity wins out against the effects of the syndrome.
The proof is indisputable. I am extremely healthy now and that change is due solely to overcoming my severe fungal problems, aka AIDS.
Having an OI associated with AIDS does not mean you have AIDS, and not all AIDS OIs are fungal.
...namely that over 96% of chronic sufferers overwhelmingly respond to anti-fungal treatment; yet, the treatment standards for this condition have not changed.
If what you are saying is accurate and has been replicated by other researchers, standards need to change. Someone should write up a CME on the subject and get it out there. But that is just one hack's opinion. :)
Today, Kevin wrote:
In January of 2004, it's safe to say that I had a fair amount of faith in the system
In January 2004, Kevin wrote:
I tell any doctor I see what works and what doesn't for my particular situation; they basically do whatever I suggest re: antibiotics and other treatments
and
I did see a doc recently who wasn't familiar with my history, who tried to tell me that antibiotics would do nothing for me. After much arguing, I cut a deal explaining that I would return in two weeks and educate him on just how necessary antibiotics were for acute exacerbations of my chronic condition. I plan to call him tomorrow
You had the same excessive certainty then (about your need for antibiotics) as you do now (about your fungal infections somehow being AIDS). You were wrong then, and you're wrong now.
I wish I would have listened to this doctor
Yeah, right.
Kevin wrote,
why don't do some follow-up research on this Mayo Clinic study and report back to all on this blog.
I'm not Mr. Jefferys but I did what Kevin wanted.
If you do, you'll discover that two subsequent studies have confirmed the findings of this initial study (from 1999!), namely that over 96% of chronic sufferers overwhelmingly respond to anti-fungal treatment
In fact I found that Kevin was wrong on all points again. 96% of CRS patients had positive fungal cultures but 100% of healthy volunteers did too. The study Kevin cites didn't involve antifungal treatments. So there was nothing treatment related for follow up studies to confirm.
I found a treatment study by the same group and I cited it unlike Kevin. 75% of patients had some improvement in symptoms, not 96%. The study was uncontrolled. Critique of study asked if lavage itself was responsible not the antifungal.
I just found Kevin's second study Richetti A et al, J Laryngol Otol. 2002 Apr;116(4):261-3. "Effect of anti-fungal nasal lavage with amphotericin B on nasal polyposis." Study was also uncontrolled. Nasal polyps eliminated in 39% of patients, not 96%. The authors speculate the lavage ITSELF might have done this, not the antifungal. In both studies the lavage may have done everything! Why do people bother doing useless studies like this?
Contrast with at least three double blind placebo control studies saying there's no effect of amphotericin B above saline solution. Other antifungals were tried in other studies with similar result.
Two uncontrolled studies versus three controlled studies.
I would say we still don't know the role of fungus in CRS. But antifungals aren't a cureall for it. Fungus is found there in CRS, but it's found in everyone else too. If fungus has a role it's probably not the fungus itself it's how the body reacts to it.
Kevin I don't mind if you call me names. I do want to understand how you pick the weakest papers as the "paradigm shifters" and ignore the more numerous well done studies like they don't exist. And confuse the numbers also what the papers are saying. Have you read these papers? Do you understand that your Mayo clinic paper wasn't about antifungal treatment for example? Anyone on here I'm sure would answer questions for you if you have them.
franklin said:
The unfairness arises not from your skepticism that a woman with an HIV-infected child might lie about IV drug abuse, but from your applying this standard only to women who seek care at "inner city hospitals" and not to EJ's mom, even though--as the girl was dying--she lied to health care workers about EJ's perinatal exposure to HIV. If a child acquiring HIV from her mom equals IV drug abuse in your world view, it should mean the same thing whether the mom is Black, White, or Hispanic. Sounds like racism to me: Poor Black and Hispanic women report never using IV drugs--they must be lying. Rich white suburbanite reports never using IV drugs--she must be telling the truth. I guess when logic fails you, you are willing to stoop to the lowest forms of argument--even racism-- just to stay in the debate.
Dear franklin,
Racial discrimination is treating people differently based on their race. Institutional racism (also known as structural racism, state racism or systemic racism) is racial discrimination by governments, corporations, educational institutions or other large organizations with the power to influence the lives of many individuals.
Institutional Racism is the exclusive victimization of poor black drug user moms by the "medical system", the "inner city hospital" and city and state agencies which have the authority to take custody of the mothers child.
Racial discrimination is the exclusive administration of toxic drugs by inner city hospitals causing harm to poor black drug user moms and their babies, and NOT to white well off suburban non-drug using moms.
Racial discrimination is the exclusive stigmatization of poor black drug user moms by inclusion in the pediatric AIDS medical literature, and the exclusion of the white well off suburban moms from the pediatric AIDs literature.
Where is the requested single reference in the medical literature in which pediatric AIDS is studied and reported in well-off white suburban non-IDU moms. There aren't any. That's because pediatric AIDS is, in fact, pediatric in-utero drug exposure, addiction and withdrawal. Pediatric Aids is in fact a creation of institutional racism. The government of South Africa understands this quite well, and has rejected this form of institutional racism.
franklin said:
How do you explain the case of Ariel Glaser, a child who died of AIDS despite having a rich white mom who didn't use drugs?
Elizabeth Glaser, like Arthur Ashe and Kimberly Bergalis died of AZT poisoning. Did Ariel die from AIDS at the age of 7, or did she die from the Intravenous AZT she received? Please show me a double blind placebo controlled study showing the survival of any human or animal exposed to INTRAVENOUS AZT. It kills all living creatures. Her HIV positive brother Jake is alive and well aged 22. How do you explain that? Her father Michael (Starsky and Hutch) reported he had a natural sexual relationship with his spouse for 13 years (81-94) and is HIV negative. How do you explain that? Regarding EJ's mom: She is alive and well without drugs. How do you explain that? Many of the so called AIDS deaths in the years after 1987 were in fact caused by AZT toxicity.
For more information see:
www.reviewingaids DOT com
www.livingwithouthivdrugs DOT com
Andrew,
Are you using your new mantra? Your latest post seems marginally more coherent, even if still seriously flawed.
But I see you still have no comment about the gross inaccuracies that have been pointed out in your previous posts. So far I've pointed out how you were dead wrong about Blumberg's historical essay on the discovery of the hepatitis B virus and about May et al.'s comparison of patient response to HAART from 1995 to 2003--both papers that you brought up yourself. Other people on this thread have pointed out at least 10 other major errors in your "facts" or "logic". Still no response from you. Well, no response except your concession:
Was that a blanket concession for all the mistakes we have pointed out in your posts, or did you have a specific error(s) in mind?
Still you do continue to lapse into your paranoid fantasy world:
Andy, no one I know views any of these people as a threat to our health care system, economic interests, or scientific enterprise. We just think they are mistaken and providing others with harmful advice.
You're almost right, Andrew. EJ's death did lead to a conundrum, but it's a conundrum for the HIV/AIDS denialists. If HIV does not cause AIDS, then why did EJ die of Pneumocystis pneumonia? Quite the conundrum for the denialists. On the other hand, if HIV causes AIDS and EJ acquired HIV perinatally from her mother, her death from pneumocystis is predictable. No conundrum for mainstream medicine. In fact it's such a big, guilt-inducing conundrum for you and your denialist cohorts that you've had to invent wild conspiracy theories and ridiculous medical scenarios to try and explain her death and autopsy findings.
EJ's death was a tragedy exactly because it was so preventable. I have never experienced the death of a child, but I am sure that EJ's parents have suffered horribly from their loss. I doubt an hour passes without thoughts of her coming to their minds. They made poor choices, taking foolish risks with EJ's health, and eventually those risks caught up with EJ and with her parents. Like any parent who loses a child at such a young age, I'm sure EJ's parents will be haunted by self-doubt and feelings of guilt for the rest of their lives.
But the guilt for EJ's death rests not only with her parents. Their foolish choices were made based on the advice of irresponsible scientists and other charlatans who distort the results of medical research. EJ's mother traces her AIDS denialism to an influential meeting with Peter Duesberg. And other scientists, including you, Andrew Maniotis, serve on the Advisory Board of her AIDS denialist organization. Therefore, much of the responsibility for EJ's death must rest with scientists such as Duesberg and yourself. You call attention to yourself by playing absurd intellectual mind games based on the deliberate distortion of the scientific work of others--and you use these mind games to convince others to forgo prevention and treatment of a fatal illness. And now a little girl is dead. You should be ashamed of yourself.
Forty,
see Ylitalo N et al, Arch Pediatr Adolesc Med. 2006 Aug;160(8):778-87. "Risk factors for opportunistic illnesses in children with human immunodeficiency virus in the era of highly active antiretroviral therapy."
982 of 1701 children in this study are black. 255 are white. Why not 100% black and no white children if your right?
I could go on with more studies but the 255 white children in this study falsify your repulsive notion, AZT is injected into black children in a genocide campaign, or white children are kept out of the literature to avoid stigmaitinzg them.
It's repugnant how you look at the very real injustices suffered by large parts of the African American community and steal and twist and distort them into lies for your own ends.
I agree Anyone that disputes hiv/aids is a loony tune, therefore I propose new postulates called Gallo's postulates.
1. find a partial correlation with a virus that is barely detectable in 1 of every thousand cells, and nuetralized by antibodies.
2. Create a window period so long to buy yourself time.
3. Forget having an animal model, just announce your new microbe to the press if you can, once its on every channel, the debate will end and everyone will beleive it,and call anyone that doesnt a "Holocaust denier"
Im new here, the real cause of many aids/cfs cases and most chronic illnesses is a bacteria called mycoplasma incognitus. DR. shyh ching lo isolated it from sick patients and grew it in culture, every animal he injected it with died. None of the control animals died. He published in a peer reviewed journal.
Go to www.projectdaylily.com to learn more.
You had the same excessive certainty then (about your need for antibiotics) as you do now (about your fungal infections somehow being AIDS). You were wrong then, and you're wrong now.
You're a philistine, Richard Jefferys.
_________________
You, of course, do not comment on the salient points that I addressed. Instead, you once again resort to character assault, carefully avoiding the facts of the matter -- the mark of a true coward. As anyone can see, I admitted I was wrong then, but I was only beginning my journey to renewed health; thus, it's very easy for me to admit my early errors in interpreting "this mess". If I would have had good health care, I would not have been given the opportunity to be so wrong. Regardless, I've carefully explained the situation, which I'm sure is beyond the appreciation of a genuine coward, such as yourself. I've noted that I was convinced, like all of you, that trusting medical professionals was completely safe; however, the good health that I now enjoy did not fall into my lap. I suffered a great deal and was wrong about quite a few things, along the way, but the biggest mistake of all was being so trusting in the face of such obvious corruption. My renewed vigor is proof enough that I am not wrong, this time. As I noted before, it is unmistakable to all who know me, all who saw me go from a 115 lb skeleton to the happy and healthy 175 lb man that I am today.
The slippery attacks of a coward are far more revealing about the one who resorts to such underhanded tactics than they are about the honest man. Nevertheless, I can certainly understand your position: it must be very difficult to defend such an inhumane and destructive ideology in the presence of an honest counter-example. You're lack of integrity is about the only fact you've bothered to demonstrate, Mr. Jefferys.
Kevin
Now here is a research from a real scientist.................its sad that reasearch that folfilled kochs postulates much more than gallo ever did gets ignored, much more evidence than microbes such as hepatitis c, hpv. (an animal model
Researchers at the U. S. Armed Forces Institute of Pathology (AFIP) in Washington, D. C., and the Warren Grant Magnuson Clinical Center at the National Institutes of Health, have found compelling evidence that a previously unrecognized opportunistic infection -- one potentially treatable with antibiotics -- may be a major cause of illness in people with AIDS. Many infections of organs including the brain, spleen, liver, or lymph nodes -- as well as some systemic infections -- might be caused by the newly-discovered organism, called Mycoplasma incognitus. Until now, these infections would be counted among the many which cannot be diagnosed.
While the first report of the organism now known as Mycoplasma incognitus was published over three years ago, most of what is now known was learned later and published last year. And only in the last few weeks has the AIDS research community paid serious attention. Until recently the new organism was mistakenly believed to be a virus, and its discovery seemed to have little immediate relevance to treatment.
Then a series of five articles by Shyh-Ching Lo and others in the American Journal of Tropical Medicine and Hygiene, between February and November 1989, showed:
(1) The new organism is a mycoplasma -- which is potentially treatable. Mycoplasma, a form of life between bacteria and viruses in complexity, was discovered about 100 years ago. Some species are known to cause human diseases.
The published articles only hint that the new organism might be treatable with antibiotics. But scientists at AFIP tested 15 common antibiotics against the Mycoplasma incognitus in the laboratory. A detailed report is being prepared for publication, but because of the public-health importance of the information, AFIP released a list of the drugs and their effective concentrations in a separate document. Doxycycline, tetracycline, clindamycin, lincomycin, and ciprofloxacin were found to be effective against Mycoplasma incognitus. But erythromycin, the antibiotic most commonly used to treat mycoplasma infections, was not effective -- and penicillin, streptomycin, gentamicin, and others also had no effect.
(2) Mycoplasma incognitus was found in the thymus, liver, spleen, lymph node, or brain of 22 of 34 persons who had died of AIDS. The patients who were selected for this autopsy study had all had evidence of organ failures.
(3) In a separate study with different patients, the mycoplasma was found in seven of ten persons with AIDS. Also, a much earlier study had found Mycoplasma incognitus in blood lymphocytes of 12 of 23 living persons with AIDS -- but in none of 22 healthy blood donors used as controls.
(4) The mycoplasma was also found in six HIV-negative patients (with no sign of AIDS) from different parts of the world, who had died in one to seven weeks of an undiagnosed infection.
No one knows how the organism spreads, but evidently it is not by casual contact, as family members of infected persons have not become infected themselves.
(5) Four monkeys were injected with Mycoplasma incognitus; all died in seven to nine months. The organism was found in the spleens of all the monkeys, and in some other organs as well. It was not found in a fifth monkey tested as a control.
(6) Extensive evidence from electron-microscope examinations, from specially designed PCR tests to look for the DNA of Mycoplasma incognitus, and from immunologic tests, showed that the organism was concentrated in lesions in affected organs. Mycoplasma incognitus is unusual in that it often infects and kills tissue without causing an inflammatory reaction, suggesting that it disables or evades part of the immune system.
The publication of this evidence, much of it in November 1989, led to a meeting between Dr. Anthony Fauci, director of NIAID (the National Institute of Allergy and Infectious Diseases) and other AIDS experts, with Dr. Lo and his colleagues at AFIP. The meeting, on December 14, 1989 in San Antonio, was chaired by Dr. Joel B. Baseman, chairman of the Department of Microbiology at the University of Texas Health Sciences Center in San Antonio, an expert on mycoplasma. An article in THE WASHINGTON POST (January 5) quoted Dr. Baseman as saying that Lo's mycoplasma "might be a significant agent for many infectious diseases, not just AIDS. There is enough information to say that this agent is real." The same article quoted Dr. Fauci as saying that Mycoplasma incognitus "may be an important opportunistic infection ...If it's real, it could have an important impact on how doctors look at AIDS patients with unexplained problems."
References
Altman LK. Unusual microbe, once dismissed, is now taken more seriously. THE NEW YORK TIMES, January 16, 1990, page B6.
Booth, W; Specter, M. Microbe may play role in AIDS, other diseases. THE WASHINGTON POST, January 5, 1990, page A3.
Lo SC; Dawson MS; Wong DM; Newton PB 3d; Sonoda MA; Engler WF; Wang RY; Shih JW; Alter JH; Wear DJ. Identification of Mycoplasma incognitus infection in patients with AIDS: an immunohistochemical, in situ hybridization and ultrastructural study. AMERICAN JOURNAL OF TROPICAL MEDICINE AND HYGIENE, November 1989, volume 41, number 5, pages 601- 616.
Lo SC; Shih JW; Newton PB 3d; Wong DM; Hayes MM; Benish JR; Wear DJ; Wang RY. Virus-like infectious agent (VLIA) is a novel pathogenic mycoplasma: Mycoplasma incognitus. AMERICAN JOURNAL OF TROPICAL MEDICINE AND HYGIENE, November 1989, volume 41, number 5, pages 586-600.
Lo SC; Dawson MS; Newton PB 3rd; Sonoda MA; Shih JW; Engler WF; Wang RY; Wear DJ. Association of the virus-like infectious agent originally reported in patients with AIDS with acute fatal disease in previously healthy non-AIDS patients. AMERICAN JOURNAL OF TROPICAL MEDICINE AND HYGIENE, September 1989, volume 41, number 3, pages 364-376.
Lo SC; Wang RY; Newton PB 3d; Yang NY; Sonoda MA; Shih JW. Fatal infection of silvered leaf monkeys with a virus-like infectious agent (VLIA) derived from a patient with AIDS. AMERICAN JOURNAL OF TROPICAL MEDICINE AND HYGIENE, April 1989, volume 40, number 4, pages 399-409.
Lo SC; Shih JW; Yang NY; Ou CY; Wang RY. A novel virus-like infectious agent in patients with AIDS. AMERICAN JOURNAL OF TROPICAL MEDICINE AND HYGIENE, February 1989, volume 40, number 2, pages 213-226.
In fact I found that Kevin was wrong on all points again. 96% of CRS patients had positive fungal cultures but 100% of healthy volunteers did too. The study Kevin cites didn't involve antifungal treatments. So there was nothing treatment related for follow up studies to confirm.
You're a buffoon, Adele, that's what I don't have time for you. There are numerous studies demonstrating that virtually all chronic sinus problems (CRS) have a significant fungal component. What is not understood, by modern researchers, but is well understood by many alternative medicine practitioners, is the very obvious reason that some people have an immune response, while others do not. The answer: those who show a hyper-immune response to fungi in the sinuses undoubtedly have significant systemic fungal infections. It's not rocket science and when patients are treated for the systemic problem with or without a topical antifungal in a nasal wash, the symptoms almost immediately resolve. Irrigation improves long-term resolution, but oral diflucan does the trick, alone, if provided for long enough at high enough dosages. I've lived it and so have many others. Regardless, here's another link that contains links to far better sources than the meager ones from which Adele has been cherry-picking:
Fungal Sinusitis is much more common than previously thought.
A quote, from the link, just for you Adele:
Fungal cultures were positive in 202 of 210 CRS patients (96%) and the diagnosis of allergic fungal sinusitis (AFS) was made in 94 of 101 consecutive surgical cases (93%).
96%...93%...whatever, it still proves that you're a dim-witted bloward.
Yet, in the face of all this evidence, standard treatment by virtually all American physicians is still antibiotics! I guess the fact that no new drugs will need to be develop plays some role in that, or perhaps the medical establishment realizes they're on a slippery slope since so many modern pharmaceuticals can lead to fungal overgrowth in the human body. Either way, as is usually the case, the Europeans have been far quicker to change treatment protocols after reviewing such convincing data. After all, the evidence is truly overwhelming.
____________________________________
I see that I've upset all of the apple-polishers on this blog...looks like you've been polishing rotten apples.
Kevin
Well, Franklin, I see I touched some nerves. You probably wouldn't believe me if I told you that I didn't post that last tome above that begins:
"Most of the HIV/AIDS establishment as well as some in the gay community, and the pharmaceutical industries that make "AIDS drugs," have increasingly regarded the questions, efforts, empirical, and homeopathic ideas of Christine Maggiore, Robin Scovill, and other "HIV/AIDS" question-askers as a threat to the rationalist, reductionist, and allopathically-focused "HIV/AIDS" practices and public health policies, as well as perhaps, an economic threat to pharmaceutical profits."
Although it is attributed to me, and I did write it, I wrote it about 2 years ago when asked to study the case of Eliza Jane.
It wasn't posted anywhere, and I only emailed it to a small number of people by the request of the parents. I had intended publishing it, but didn't at their request. For the life of me (note how some of the info is dated before other events have come to light) I cannot figure out who posted it? Please ask your webmaster to check where it came from for me, will ya?
At any rate, my concession above is meant as a good will gesture, that indeed I am reading all that is put before me. It has taken me a few days but I have read the following posted by Adele:
Palumbo, P.E., et al., Predictive value of quantitative plasma HIV RNA and CD4+ lymphocyte count in HIV-infected infants and children. Jama, 1998. 279(10): p. 756-61.
75. Church, J.A., HIV disease in children. The many ways it differs from the disease in adults. Postgrad Med, 2000. 107(4): p. 163-6, 169-71, 175-6 passim.
76. CDC, 1994 Revised Classification System for Human Immunodeficiency Virus Infection in Children Less Than 13 Years of Age, 1994, CDC.
77. Urschel, S., et al., Withdrawal of Pneumocystis jirovecii prophylaxis in HIV-infected children under highly active antiretroviral therapy. Aids, 2005. 19(18): p. 2103-8.
78. Thea, D.M., et al., Benefit of primary prophylaxis before 18 months of age in reducing the incidence of Pneumocystis carinii pneumonia and early death in a cohort of 112 human immunodeficiency virus-infected infants. New York City Perinatal HIV Transmission Collaborative Study Group. Pediatrics, 1996. 97(1): p. 59-64.
With a complete willingness to be proven wrong about my views (science is self-correcting and inexorable in this regard), during the past several days, I looked at these articles, and many more related links on Medline that these articles are associated with, and my initial question still stands because nowhere in any of these studies does it say that HAART-naive persons die of PCP with absolute lymphocytes counts of 10,800/ul. In fact, the articles themselves are mostly studying the effects of HAART on "viral load" and CD4 lymphocyte counts-and as one might image, low counts are always associated with poor survival, and in one case I found, PCP prophylaxis is advised to be discontinued when the CD4 count is higher than 400, because it is unnessessary as persons with higher counts do not suffer from PCP, unless of course they are on HAART. Absolute counts reflect similar if not identical trends according to all the available studies that have compared the two (CD4 and absolute).
But according to your logic, PCP can occur in people whose lungs sound clear to 3 physicians stethoscopes preceding their death, and whose "autopsy" slides show little if any infiltrate, and who harbored 10,800 total T-cells hours before their death from PCP? A heart that is enlarged 150% of normal is an AIDS-defining illness (I guess "HIV" has learned to replicate in dividing cardiac muscle cells? Children who gain weight are suffering from failure to thrive of AIDS wasting? The WHO guidelines I posted above on ALL CASES of beta-lactam delayed reactions (not pre-sensitized only) have no meaning for you, AIDS being a disease of too many lymphocytes rather than too few lymphocytes doesn't bother you people? A mother who never tests the same on 6 "HIV" tests is "HIV-positive," and who can't transmit it to her partner after 12 years (pretty strange to have a long-term-non-progressor and a CCR5 mutant man in the same family don't you think? What would be the odds of that happening. Rare as unicorns I would think?
Interesting ideas? Concessions perhaps, from you? Maybe next time there is a similar threat to the AIDS establishment, Ribe or whomever can pick better slides to go with the T-cell count (or at least erect a plausible story) before trying a family for child neglect in the LA Times?
The responsibility for the death rests with more than just with "scientists" like me and Duesberg: all of us, like Wainberg says, belong in jail for asking questions about T-cells, etc. E.G.
Dr. Luc Montagnier, Virologist, discoverer of "LAV", Institute Pasteur Paris:
"There are too many shortcomings in the theory that HIV causes all signs of AIDS. We are seeing people HIV-infected for 9, 10, 12 years or more, and they are still in good shape, their immune system is still good. It is unlikely that these people will come down with AIDS later." (Miami Herald 23 Dec. 1990). From his original paper in Science in 1993, Montagnier wrote that: "....replication and cytopathic effect of LAV (HIV) can only be observed in activated T4 cells. Indeed, LAV infection of resting T4 cells does not lead to viral replication or to expression of viral antigen on the cell surface, while stimulation by lectins or antigens of the same cells results in the production of viral particles, antigenic expression and the cytopathic effect" (Klatzmann & Montagnier, 1986)."
Dr. Etienne de Harven, Dr. Etienne de Harven is emeritus Professor of Pathology, University of Toronto. He worked in electron microscopy (EM) primarily on the ultrastructure of retroviruses throughout his professional career of 25 years at the Sloan Kettering Institute in New York and 13 years at the University of Toronto. In 1956 he was the first to report on the EM of the Friend virus in (mouse) leukemia, and in 1960, to coin the word "budding" to describe steps of virus assembly on cell surfaces.
"Dominated by the media, by special pressure groups and by the interests of several pharmaceutical companies, the AIDS establishment efforts to control the disease lost contact with open-minded, peer-reviewed medical science since the unproven HIV/AIDS hypothesis received 100% of the research funds while all other hypotheses were ignored." (Reappraising AIDS Nov./Dec. 1998).
"The faith in retroviruses as pathogens assumed quasi-religious proportions," de Harven laments. "Since electron microscopy could not demonstrate viruses in the 1.16 bands from human subjects, we forgot about microscopy and started relying on 'markers.' Microscopy is time-consuming and skill-demanding. Who has time for that? Not when research funding was getting difficult and when major pharmaceutical corporations were starting to finance 'crash programs' for speedy answers." Reappraising AIDS Nov./Dec. 1998.
"When retroviruses are legion, molecular markers provide a useful approach to quantification probably better than direct particle counting under the electron microscope (which I always found difficult). But without isolates, the use of markers is methodological nonsense. 'Markers' of what? We know that all of the so-called 'HIV markers' are totally non-specific." Reappraising AIDS Nov./Dec. 1998.
Dr. Alfred Hässig, Emeritus Professor in Immunology at the University of Bern, former Director Swiss Red Cross blood banks: Director of the Swiss Red Cross Transfusion Service, and President of the Board of Trustees of the International Society of Blood Transfusion. With colleagues he formed the Study Group for Nutrition and Immunity. The Swiss research group doesn't believe that HIV causes AIDS. According to Hässig et al. AIDS is a multi-causal disease caused by severe stress.
"The sentence of death accompanying the medical diagnosis of AIDS should be abolished." (Sunday Times (London) 3 April 1994)
"In the virological research, so much money is invested, and the research people want to stay in that area because if you deviate to research in other directions probably other people come in and must be funded." (Meditel 1992).
"Virologist have nothing new to offer. They keep coming up with excuses, they find constant growth and change in the virus structure, it evades, attacks, strange things, but none of them has the courage to explain properly how these things could possibly be so." (Continuum Jan/Feb 1996)
"AZT (anti-viral AIDS medicine) has, in countless cases, brought about the inevitable and slow asphyxiation of the patient's body cells. The doctors wrongly diagnose the fatal consequences of AZT medication as AIDS following a prior HIV infection. Treatment with AZT and allied toxic substances may be equivalent to joining a suicide squad with a time fuse."
"It is the duty of every doctor to preserve life at any cost -- and not death-curse people based on any test so they are so frightened they kill themselves. I am sad to say that these voodoo methods were practiced despite there never being any proof that the detected antibodies are an indication of mortality in all diagnosed people. I consider it medical malpractice to push patients into dying by prophesying an early death. We are medical scientists, not prophets!"
Dr. Heinz Ludwig Sänger, Emeritus Professor of Molecular Biology and Virology, Max-Planck-Institutes for Biochemy, München. Robert Koch Award 1978:
"Up to today there is actually no single scientifically really convincing evidence for the existence of HIV. Not even once such a retrovirus has been isolated and purified by the methods of classical virology." (Letter to Süddeutsche Zeitung 2000).
"The result of my intensive literature research shows that so far not one publication exists, in which is being described that HIV has been isolated, purified, and characterized by the criteria of classical virology." (Forword Mythos AIDS 2000).
"During the past 20 years HIV-AIDS research has shown to a line of critical scientists again and again that the existence of HIV has not been proven without doubt, and that both from a aetiological (causal), and a epidemiological view, it can not be responsible for the immunodeficiency AIDS. In view of the general accepted HIV/AIDS hypothesis this appeared to me so unbelievable that I decided to investigate it myself. After three years of intensive and, above all, critical studies of the relevant original literature, as an experienced virologist and molecular biologist I came to the following surprising conclusion: Up to today there is actually no single scientifically really convincing evidence for the existence of HIV. Not even once such a retrovirus has been isolated and purified by the methods of classical virology." (Letter to Süddeutsche Zeitung Oct. 2000)
Dr. Joseph Sonnabend, New York Physician, founder of the American Foundation for AIDS Research (AmFAR), who latter quit the foundation after he found their statisitics were being used for political purposes by the AIDS establishment:
"The marketing of HIV, through press releases and statements, as a killer virus causing AIDS without the need for any other factors, has so distorted research and treatment that it may have caused thousands of people to suffer and die." (Sunday times (London) 17 May 1992).
Dr. Sam Mhlongo: Head of the Department of Family Medicine and Primary Health Care at the Medical University of South Africa:
"The case for a link between HIV and AIDS is not proven. I would like the "orthodox" scientists to acknowledge that in Africa there are 29 or 30 diseases which may mimic AIDS, which are related to poverty. But they will not accept that because poverty does not make them big money but HIV makes them money. If we dissidents had only one hundredth of the funds that the orthodox view has, the orthodox view would probably be dead in less than a year."
Dr. Kary Mullis, Biochemist, 1993 Nobel Prize for Chemistry:
"If there is evidence that HIV causes AIDS, there should be scientific documents which either singly or collectively demonstrate that fact, at least with a high probability. There is no such document." (Sunday Times (London) 28 nov. 1993).
Dr. Walter Gilbert, Professor in Molecular Biology, 1980 Nobel prize for chemistry:
"I would not be surprised if there were another cause of AIDS and even that HIV is not involved." (Omni June 1993)
"[Duesberg] is absolutely correct in saying that no one has proven that AIDS is caused by the AIDS virus. And he is absolutely correct that the virus cultured in the laboratory may not be the cause of AIDS." (Hippocrates Sept./Oct. 1988)
"The community as a whole doesn't listen patiently to critics who adopt alternative viewpoints. Although the great lesson of history is that knowledge develops through the conflict of viewpoints." (Meditel 1990).
Dr. Albert Sabin, Virologist:
"I think the views of a person like Dr. Duesberg are terribly, terribly important, and we must pay attention to them." (Oakland Tribune 31 Jan. 1988).
(He should know-he and Salk are attributed to spreading SV-40 to more than 300 M folks). Woops!
Dr. Michael Lange: Head of AIDS Programme St. Lukes Hospital, New York:
"What I would strongly support is a more open discussion. We do not know the pathogenesis of this disease. And we were very early forced into a very dogmatic view: namely that somehow HIV kills the T-cells." (Spin April 1991).
Dr. Steven Jonas, Professor of Preventive Medicine, Suny Stony Brook, NY:
"Evidence is rapidly accumulating that the original theory of HIV is not correct." (Sunday Times (London) 3 April 1994)
Dr. Beverly Griffin, Director of the Department of Virology, Royal Postgraduate Medical School, Hammersmith Hospital London:
"It will surely lead to a scientifically healthier society if the burden of proof for HIV as a deadly pathogen is returned to where it belongs - to those who maintain that HIV causes AIDS - and others are allowed to pursue alternative approaches in the battle for eradiction of the disease." (Nature 20 April 1989).
Dr. Henk Loman, Professor of Biophysical Chemistry at the Free University in Amsterdam:
"There are many people with AIDS but without HIV, and a great many people with HIV but without AIDS. These two facets mean that HIV = AIDS is much too simple. Plausible, alternative, testable causes of impairment of the immune system which may ultimately lead to AIDS should become part of regular AIDS research." (Sunday Times (London) 3 April 1994).
Dr. Fabio Franci, Specialist in Preventive Medicine and Infectious Diseases, Trieste, Italy:
"I am not an agnostic; I am well convinced HIV is harmless." (Sunday Times (London) 3 April 1994)
Dr. Paul Rabinow, Professor of Anthropology, University of California at Berkeley:
"In particular I have pursued the situation of haemophiliacs and HIV because it was the arena least charged with moralism. Systematic attempts to be allowed to look at the data or to find rigorous controlled studies have failed." (Sunday Times, London,1994).
Dr. Andrew Herxheimer, Emeritus Professor of Pharmacology, UK Cochrane Centre, Oxford:
"I think zidovudine [AZT] was never really evaluated properly and that its efficacy has never been proved, but it's toxicity certainly is important. And I think it has killed a lot of people. Especially at the high doses. I personally think it not worth using alone or in combination at all." (Continuum Oct. 2000)
Dr. Arthur Gottlieb, Chairperson of the Department of Microbiology and Immunology at the Tulane University School of Medicine:
"The viewpoint has been so firm that HIV is the only cause and will result in disease in every patient, that anyone who challenges that is regarded as 'politically incorrect.' I don't think - as a matter of public policy - we gain by that, because it limits debate and discussion and focuses drug development on attacking the virus rather than attempting to correct the disorder of the immune system, which is central to the disease." (Penthouse April 1994).
Dr. Roger Cunningham, Immunologist, Microbiologist and Director of the Centre for Immunology at the State University of New York at Buffalo:
"Unfortunately, an AIDS 'establishment' seems to have formed that intends to discourage challenges to the dogma on one side and often insists on following discredited ideas on the other." (Sunday Times, London, 3 April 1994).
Dr. Gordon Stewart, Emeritus Professor of Public Health, University of Glasgow:
"AIDS is a behavioural disease. It is multifactorial, brought on by several simultaneous strains on the immune system - drugs, pharmaceutical and recreational, sexually transmitted diseases, multiple viral infections." (Spin June 1992)
"Nobody wants to look at the facts about this disease. It's the most extraordinary thing I've ever seen. I've sent countless letters to medical journals pointing out the epidemiological discrepancies and they simply ignore them. The fact is, this whole heterosexual AIDS thing is a hoax." (Spin June 1992)
"AIDS is a behavioural disease. It is multifactorial, brought on by several simultaneous strains on the immune system - drugs, pharmaceutical and recreational, sexually transmitted diseases, multiple viral infections." (Spin June 1992)
"The hypothesis that HIV is the sole cause of AIDS simply does not fit the clinical and epidemiological facts"
"From both my literature review and my personal experience over most of the AIDS - so called AIDS centers in Africa, I can find absolutely no believable persuasive evidence that Africa is in the midst of a new epidemic of infectious immunodeficiency." (Meditel 1992).
Dr. James Hudson, Professor of Pathology and Medicine, University of British Columbia
"I stopped going to AIDS meetings several years ago -- I could no longer stand the stress of restraining myself from getting up and shouting, 'Rubbish!"
Dr. Manu Kothari: Professor of Anatomy, Seth G.S. Medical College, Mumbai India:
"For all we know, it is not HIV that causes AIDS, but the so-called co-factors such as indiscriminate antibiotic use, recreational drugs, poverty, malnutrition, polluted water and pesticised food. AZT and the like (so-called triple therapy) are rank cytotoxic poisons. To give AZT to pregnant women is a crime against the mother and the baby she is making."
Dr. Frank Buianouckas: Professor of Mathmatics, Bronx New York.
"I am suspect about everything involved in this AIDS epidemic, because if HIV causes anything, it certainly causes fund-raisers. It sells stocks. It supports dances. It sells condoms. And it keeps the AIDS establishment going." (Penthouse Dec. 1995)
Dr. Donald Abrams: Prof. of Medicine, San Francisco General Hospital:
"I have a large population of (HIV + patients) who have chosen not to take any anti-viral drugs. They've watched all of their friends go on the anti-viral bandwagon and die."
.Dr. Manu Kothari: Professor of Anatomy, Seth G.S. Medical College, Mumbai India:
"For all we know, it is not HIV that causes AIDS, but the so-called co-factors such as indiscriminate antibiotic use, recreational drugs, poverty, malnutrition, polluted water and pesticised food. AZT and the like (so-called triple therapy) are rank cytotoxic poisons. To give AZT to pregnant women is a crime against the mother and the baby she is making."
Andy Maniotis. Chief Dish and Bottle Washer, University of Illinois, Chicago:
Profound immunosuppression is caused by a myriad of factors and it is incorrect to group these syndromes under a single disease entity, "HIV/AIDS." The consequences of this view suggest that different treatment strategies are needed for the spectrum of the 46 previously known "AIDS-indicator diseases," rather than the toxic and dangerous pharmaceutical or vaccination approaches currently in place.
Alas!
It should be obvious to the lurkers by now that there has been a deafening silence here in the inability to cite a single pediatric AIDS study in which the mothers were not mostly black, poor inner city hard drug and IV drug users.
You are shifting the goal post further and further.
Now you won't accept a paper where most, but not all, of the mothers are black.
You have been given references where not all mothers of perinatally infected children were black and where not all mothers of perinatally infected children were IV drug users (confirmed by blood tests).
Elizabeth Glaser, like Arthur Ashe and Kimberly Bergalis died of AZT poisoning.
You obviously get all your factoids from reading Duesberg. Duesberg writes in his book that Bergalis was perfectly healthy before she took AZT. This is a complete lie. It doesn't become any less of a lie if fools repeat it.
Bergalis had systemic candidiasis, severe weight loss, PCP and a CD4+ count of less than 50 before she was ever prescribed AZT.
AIDS From A Healer, Scorn From Others
Dr. Walter Gilbert, Professor in Molecular Biology, 1980 Nobel prize for chemistry:"I would not be surprised if there were another cause of AIDS and even that HIV is not involved." (Omni June 1993)
Andrew, why are you quoting Walter Gilbert's comment from 1993 when you are perfectly aware that he no longer holds this view?
How amny of the others that are still alive have changed their views?
People like walter gilbert get so much pressure from aids inc. some partially recant their statements, it doesnt mean they dont beleive it inside.
heres another brilliant scientist that questioned the hiv aids hypothesis, he heads the most sophisticated lab in the history of the world, the armed forces institute of pathology. If we go to war, this is the lab that will have to identify the bio weapons our enemies use.
"There is no good explanation for why and how the virus breaks out of the antibody protection," says Lo. "I'm not saying that HIV plays no role in AIDS -- the data shows a clear correlation with disease. But AIDS is much more complicated than HIV."
"In the spirit of "the openness" of science we salute Peter Duesberg for his challenging and courageous voice speaking out against the present scientific establishment. His extensive experience and knowledge about retroviruses lends merit to his critical evaluation of the possible causative role of HIV in the AIDS disease.
We believe the most healthy and responsible scientific attitude in dealing with AIDS research is to explore all possible avenues. To make any conclusion lightly or prematurely, such as ruling out any possible role of microbes in AIDS, or to commit oneself exclusively to a particular agent and completely rule out any other possible role of a different microbe, may all result in a greater loss of AIDS victims."
Shyh-Ching Lo M.D. PHD
Chief, Division of Geographic Pathology
Col. Douglas J. Wear, MC USA
Chairman
Department of Infectious and Parasitic Disease Pathology
Department of Defense
Armed Forces Institute of pathology
Washington, DC
His mycoplasma hypothesis is was ignored by Aids inc. even though he had an animal model. This bug is fouund at much higher rates in cfs, AIDS, ra and many other chronic illnesses. Thanks to Aids inc it was ignored an now there is an epidemic Of CFS etc.
I suggest you read www.projectdaylily.com to see how this bug was tested on americans and was part of the biological weapons program.
Andrew Maniotis wrote:
Absolute counts reflect similar if not identical trends according to all the available studies that have compared the two (CD4 and absolute).
You'd think I'd be used to it by now, but the magnitude and transparency of the lies continues to surprise me. The correlation between CD4 (count or %) and TLC (or ALC) is weak (the strongest correlation I can find in the literature is r=0.76). The Lancet paper you've cited states the following:
"Analysis of all pairs of measurements within yearly age bands showed that total lymphocyte count and CD4-cell percentage were weakly positively associated, with correlation coefficients ranging from 0â¢08 to 0â¢19."
Perhaps, as a scientist, you could comment on the strength of that association? These are quotes from (and links to) the other studies I could find that looked at the question, they are also not compatible with your claims (each quote is from a different study):
"On bivariate analysis, the absolute CD4+ count correlated positively with total lymphocyte count (r = 0.28 0.48 0.64)... Furthermore, on bivariate analysis total lymphocyte count correlated positively with absolute CD8+ count (r = 0.82 0.88 0.92). In conclusion, although there was a positive correlation between absolute CD4+ count and total lymphocyte count, the clinical significance is questionable as the total lymphocyte count correlated more strongly with the absolute CD8+ count."
"An overall modest correlation was observed between absolute lymphocyte count and CD4 lymphocyte (r = 0.51)"
"For the observations as a group, a correlation (r = 0.704) between CD4+ T-cell count and TLC was demonstrated, but if the patients were divided into three groups according to their CD4+ T-cell count, this correlation weakened considerably. Therefore, although TLC shows a correlation with CD4+ T-cell count, it is not a good predictor of the CD4+ T-cell count in this population and should preferably not be used in the clinical care of HIV/AIDS patients."
"We cannot recommend the use of ALC as a surrogate for CD4+ count in our environment as this study has clearly shown that the correlation between the two is weak."
"Only a weak correlation was observed between TLC and CD4 counts (r=0.41, p=0.05). As a predictor of CD4 count, TLC cut-offs less than 2.0 and less than 1.0 x 10(9)/L were unable to predict these values reliably, but showed that at TLC cut-offs of less than 1.0 x 10(9)/L there was a high chance of CD4 counts being under 200 cells/mm(3)."
"A significant linear correlation was seen between the log10 CD4 count and log10 TLC (Pearson's correlation coefficient = 0.70, p less than 0.001). The finer cut off value for TLC where false positive error rate is minimum and sensitivity maximum was 1500-2000 cells/mm3."
"The correlation between 1534 paired absolute lymphocyte count and CD4 lymphocyte count was found to be high (R = 0.76). When analysed by stage of HIV infection, the correlation increased from R = 0.64 for asymptomatic patients, to R = 0.72 for patients with symptomatic non-AIDS HIV infection and R = 0.73 for AIDS patients. Correlations between absolute lymphocyte count and CD4 per cent were considerably weaker: R = 0.41 all paired counts; R = 0.32 for asymptomatic patients; R = 0.25 for symptomatic non-AIDS patients; R = 0.32 for AIDS patients."
"in this setting, TLC is not a reliable predictor of CD4 cell count in HIV-infected individuals."
"All parameters except TLC predicted survival in univariate Cox models"
Notice also that the correlation is consistently strongest at the lower values, much weaker to non-existent at higher values. This is in line with the Lancet study on prognostic markers finding that: "Above the age of 2 years, mortality risk increased sharply at total lymphocyte counts less than 1500-2000 cells per μL, with little trend at higher values." What they mean is not that there was zero risk at higher values, but that there was little trend toward a difference in risk across the selected higher values looked at in the study (3,000, 4,000 & 6,000). This is because peripheral blood CD4 counts decline but CD8 T cell count increases mask that decline (see close correlation between absolute CD8 T cell counts and TLC reported above). Only in the most advanced stage of disease does the TLC tend to plummet, by this point there is a severe depletion of naive CD8 T cells (which occurs in parallel with naive CD4 T cell loss; the pace of the loss correlates significantly with the levels of CD4 and CD8 T cell activation) and the accumulation of memory CD4 and CD8 T cells that cannot proliferate (and can therefore not maintain the memory T cell compartment by proliferating).
These are the only studies I have found that provide data on total lymphocyte count or white blood cell count at PICU admission. They don't support your claims, either.
J Trop Pediatr. 2007 May 25; [Epub ahead of print]
Children with Human Immunodeficiency Virus Infection Admitted to a Paediatric Intensive Care Unit in South Africa.
Lower total lymphocyte count (p = 0.004) and higher gamma globulin level (p = 0.04) were paradoxically the only findings significantly associated with survival.
Pediatr Emerg Care. 1993 Oct;9(5):265-9.
HIV-infected children in the pediatric emergency department.
Patients with a white blood cell count more than 15,000/mm3 were more likely to be hospitalized (87 vs 62%, P less than 0.01), though the white blood cell count was not helpful in identifying patients with bacteremia or serious infections.
People like walter gilbert get so much pressure from aids inc. some partially recant their statements, it doesnt mean they dont beleive it inside.
Is this the best explanation that cognitive dissonance can give you.
His mycoplasma hypothesis is was ignored by Aids inc. even though he had an animal model. This bug is fouund at much higher rates in cfs, AIDS, ra and many other chronic illnesses. Thanks to Aids inc it was ignored an now there is an epidemic Of CFS etc.
It wasn't ignored. It was investigated and found to be wrong.
Lo's latest paper indicates that not all AIDS patients have mycoplasm.
"In the United States, the organism rarely infects other risk groups of HIV-infected patients, such as intravenous drug users (IVDUs) and hemophiliacs (both less than 1%) [5]. In comparison, 10-15% of HIV-negative and 27-37% of HIV-infected male homosexuals have M. penetrans-specific antibodies."
Mycoplasma penetrans infections and seroconversion in patients with AIDS: identification of major mycoplasmal antigens targeted by host antibody response.
I suggest you read www.projectdaylily.com to see how this bug was tested on americans and was part of the biological weapons program.
No. You've got it wrong. HIV was created as a part of the biological weapons program!
You can't argue with the flowchart
Dear 40 mules,
Thanks for looking up the definitions of racism.
Now apply your definition to your own formulation of the EJ case. I think you will find that it is racist.
Because you claimed that EJ's mother is not a drug addict, you asked for examples of studies of pediatric AIDS in which the mothers were not IV drug abusers. We provided several such studies, including a study in which 76 of the 129 afflicted children were born to women with no history of IV drug abuse. You rejected that study because the mothers were patients at Harlem Hospital Center and Columbia University and therefore you assumed that they were all "poor black drug users." You assumed that the mothers of all 76 children had to be lying when they denied IV drug use because they seek health care at inner citiy hospitals that serve a predominantly minority population. Yet when EJ's mother denies drug use, you assume she is telling the truth because she is white and well-to-do.
Look back at your definition. "Racial discrimination is treating people differently based on their race." I think your logic meets the definition.
Dear 40 mules,
I tried to accommodate your racist attitudes by reminding you about a well-publicized case of a wealthy white woman who became infected with HIV through a blood transfusion and transmitted the virus to both of her children. Her daughter, Ariel Glaser, died of AIDS at age 7. I guess you found this case impossible to reconcile with your theory that pediatric AIDS is entirely due to maternal drug abuse in the inner city. You had no explanation--you only had a question:
The answer is that she died of AIDS. She did not die from intravenous AZT.
Had you read the information hyperlinked to Ariel's name, you would have learned that Ariel died before any anti-retroviral drugs were available for children. Her parents tried desperately to obtain AZT for Ariel, but they were unsuccessful. Ariel never received AZT. Her death could not have been due to AZT or any other anti-retroviral therapy--because she received none. Read about Ariel and about the parents of other HIV-infected children who were forced to helplessly watch their dying children become blind and demented and still could not get approval to have their children treated with AZT in this NY Times article from 1989.
Once again you prove that AIDS denialists have no regard for the facts. You are committed only to advancing a point of view and will simply ignore any and all evidence to the contrary. Ariel's tragic death was pretty much run-of-the-mill for pediatric AIDS cases back in the 1980's. Nowadays, deaths like Ariel's can largely be prevented. Unfortunately for EJ, her parents chose to ignore the lesson of Ariel Glaser.
My point is the only way to get people like walter gilbert to say what they really mean is to quit intimidating them and let them speak freely. As long as we live in a society that treats people who question hiv like holocaust deniers, its no wonder they speak in riddles.
Walter gilbert made one statement in a private email after years of intimdation and you hiv fundamentalists ignore the many public statements he's said in the past against the hiv hypothesis.
As far as Dr. lo's work, it was never debunked, it cant be debunked actually. He found a microbe that caused a fatal disease in every animal he injected it with. None of the control animals died. He could see the mycoplasma damaging the organs with electron microscopy. It was found to be the cause of death in 7 hiv negative people who died of mysterious infections. (all these refrences are posted above)
As far as it not being in every Aids patient, lo's hypothesis was that there were several different causes of AIDS/immune supression and it is ridiculous to blame it all on one particular agent (hiv) or lifestyle(duesberg) a multitude of factors can play a role.
For example if 10 people had a fever, it does not mean the cause of the fever is the same in every patient, with some it could be the flu, for others it could be an allergic reaction. Just because the symptoms are the same, doesnt mean the cause is the same.
Anyways since you are so quick to "debunk" lo's work, where Did gallo have an animal model?, did he actually see the hiv damaging organs with the electron microscope like Lo did with mycoplasma? How does hiv which only infects a small fraction of tcells (1 in 100 or so) how does it cause organ failure which was seen in many AIDS patients that Lo actually examined?
You cant debunk Lo because he folfilled kochs postulates much more than Gallo or the virus hunters that gave us hepatis c ever did.
What about people with gulf war syndrome and chronic fatigue syndrome that test positive for this microbe? dont they have a right to learn of this research? Or because the CDC has officially abandoned them, you people as always must follow thier lead...............
My point is the only way to get people like walter gilbert to say what they really mean is to quit intimidating them and let them speak freely. As long as we live in a society that treats people who question hiv like holocaust deniers, its no wonder they speak in riddles.
Walter gilbert made one statement in a private email after years of intimdation and you hiv fundamentalists ignore the many public statements he's said in the past against the hiv hypothesis.
Some of Gilbert's quotes are from 1988. At this stage it was not totally unresonable to raise some questions. In 2007 it is not.
Gilbert has looked at the evidence that has accumulated since he made those comments and changed his mind. It is called rethinking - something that self-styled "rethinkers" do rarely or never. It takes guts to admit that you were wrong. Gilbert had enough strength.
The weaker option is to slip into delusional thinking and to never admit to being wrong. Duesberg and others fall into this category. Duesberg has invested too much into his Denial. He'll never admit to being wrong.
Walter gilbert just gave a glowing review of bialy's laudatory book on duesberg in 2004 , now why would he do that if doesnt still have doubts?..............thanks for ignoring my points on mycoplasma incognitus, I guess you dont have an answer......................LOL
Walter gilbert just gave a glowing review of bialy's laudatory book on duesberg in 2004 , now why would he do that if doesnt still have doubts?..
What exactly did he write? Or are you just repeating what you read on "dissident" websites.
..thanks for ignoring my points on mycoplasma incognitus, I guess you dont have an answer......................LOL
LOL.
There are several hundred papers published since 1989 that cite Lo's initial papers. Read some of them (there is a tool called the Science Citation Index that can help you find them). The world didn't stop in 1989.
Mycoplasma ignognitus is actually a strain of mycoplasma fermentans that was most likely a contaminant in Lo's tissue cultures.
There is no evidence that mycoplasma fermentans is anything other than an opportunistic infection and a co-factor in AIDS.
Lo himself has published about mycoplasma fermentans and chronic fatigue syndrome.
Absence of antibody to Mycoplasma fermentans in patients with chronic fatigue syndrome.
and Gulf War Syndrome
Lack of serological evidence for Mycoplasma fermentans infection in army Gulf War veterans: a large scale case-control study.
Cooler,
I couldn't find that Gilbert review of Bialy's book. Are you sure he wrote one? Could you give us a link?
Mycoplasma contamination is one of the commonest things in any cell culture lab. Today alot of labs test their stuff routinely for it. Why? Because its everywhere. You can keep your cultures free of most bacteria and fungi if you're careful but Mycoplasma is a insidious little beastie. Finding Mycoplasma in cultured samples from AIDS patients in 1989 is like finding water in samples, it's everywhere. Doesn't mean water causes AIDS. By the way no one called you a holocaust denier. A denier denies something like a historian studies the history of something. If someone calls you a historian it doesn't mean you have to be a Holocaust historian. When someone calls you a denier or denialist, it doesn't mean you're a Holocaust denier.
Kevin, Mr. Jefferys has exposed you as a hypocrite, and I showed yesterday you don't understand or read scientific literature. Doctors didn't force antibiotics on you to kill you, YOU DOCTOR-SHOPPED and INTIMIDATED your doctors until they gave you what you wanted. Your sickness was probably caused by your stubborness. And then you blame corrupt medicine and shill doctors and do a 180 and now you agree with the doctors who didn't want to give you antibiotics back then!
Next you read a press release about how the Mayo Clinic applied for a patent on antifungal treatment for CRS. It said two studies confirmed the drug works. You come on here, confuse or lie all the statistics like 96% efficacy instead of 39% or 75%, don't mention there weren't any controls, and don't mention THREE subsequent responsibly designed controlled studies found there was no effect of antifungals. It was placebo effect or maybe just the lavage itself. AND 100% of healthy people have fungus compared to 96% of people with CRS.
No one here disputes immune response to fungus probably has a role in CRS. I said that twice yesterday I mentioned the paper giving diagnostics for AFS from 1996. But you want to believe fungus is the cause of everything including AIDS just like you wanted to believe you needed lots of antibiotics two years ago. But if your this ignorant in your own area of personal medical experience that you don't even know the literature on it, why should anyone trust you on HIV or AIDS something you never even experienced and you don't know anything about?
You've been exposed as a hypocrite and either a liar or an ignorant person. Calling me names won't change it.
Doctors didn't force antibiotics on you to kill you, YOU DOCTOR-SHOPPED and INTIMIDATED your doctors until they gave you what you wanted.
Oh, the poor, poor doctors that I intimidated ... I hope they've recovered from my evil intimidation. Of course, I wouldn't know about that because I had to leave their care in order to get well, but you don't find anything significant about that fact, right Adele?
Regardless, you are damn right that I "doctor-shopped"! I'm alive today because I had the good sense to question those ignorant bastards. Sure, it took me a while to figure out what was really going on with my body, and I certainly made mistakes; but then again, I'm not a trained physician, like all of those easily-intimidated doctors.
You are the hypocrite, Adele. You act all self-righteous because a very sick patient intimidated his doctors into providing care that he thought helped, and I only did that because they were too stupid to know which antibiotics actually helped my acute flare-ups. Too lazy to culture, they were. Nevertheless, you have remained notably silent as I, and others, have demonstrated the significant intimidation and even blatant bribery wielded by pharmaceutical representatives, every day in doctors' offices all around the country. My indiscretion hardly seems worthy of mentioning, by comparison, but your own hypocrisy is glaringly obvious.
______________________________
You come on here, confuse or lie all the statistics like 96% efficacy instead of 39% or 75%...
People can read the study results for themselves from the link that I provided. Your "interpretations" are unnecessary, and the fact is you are wrong. You, however, seem to have trouble admitting your wrong, Adele, isn't that right? That said, here's another quote from the site that I previously provided which, incidentally, is affiliated with the Mayo Clinic in Rochester, MN:
"Recent studies by researchers at the Mayo Clinic in Rochester, Minnesota have revealed that the underlying cause for chronic rhinosinusitis may in fact be the presence of fungus in the nasal cavity that causes an immune response in some people that then results in the symptoms of CRS. This ground-breaking research has led to better understanding of the condition and the availability of new treatment options...Existing interventions have largely focused on the use of antibiotics, inhaled or oral corticosteroids, and surgery. Antibiotics are most useful in treating acute exacerbations that result from bacterial invasion of the damaged epithelial tissue that characterizes CRS. However, no antibiotic is effective in preventing the triggers for the tissue-damaging eosinophilic inflammation, and antibiotics are not effective in eradicating the causative factors for CRS.
Our good pal, Robster, was harping about prevention as the key, well here is yet another opportunity for preventing disease that modern medicine has failed to sieze for no matter how much you wish away the facts, Adele, this is an easily identifiable failure of our current health care system to adequately and timely amend treatment protocols for the most common ailment resulting in doctor visits, today -- chronic allergic rhinosinusitis. After all, this information has been around for 8 years and just like with HIV/AIDS, profit has trumped human health concerns. It's a lot more profitable for the pharmaceutical companies and the doctors to continue treating this condition with expensive antibiotics and equally expensive endoscopic surgeries (most patients have multiple surgeries) than to treat the underlying causative disease mechanism. Once the underlying fungal problem is removed, the acute bacterial infections resolve. I haven't had a sinus infection in 2.5 years and as Mr. Jefferys detective work revealed, I used to get them every 3 months, like clockwork. I guess you don't find that important either, right Adele?
Furhermore, as I've noted previously, even the Mayo Clinic doesn't fully understand the implications of their work, but at least they're on the right track and producing quality research. This research has, however, allowed alternative medicine caregivers to begin aggressively treating fungal disease, with undeniably positive results.
You and others on this blog like to pretend that I am anti-science, but that is not the case, at all. There is plenty of quality research being conducted, but unfortunately, it's only utilized once the pharmaceutical industry and/or medical professionals find a way to make the huge personal profits to which they've become accustomed. That's a fact, and there are plenty of other examples besides fungal sinusitis and HIV/AIDS. Those are just the two with which I am intimately familiar.
________________________________
But you want to believe fungus is the cause of everything including AIDS just like you wanted to believe you needed lots of antibiotics two years ago.
It was 3.5 years ago, you twit. I don't want to believe anything. I'm working with facts here. Virtually, all AIDS patients suffer from numerous fungal infections, just as it was in my case. In fact, oral candidiasis is the most common "first sign" of AIDS, just as it was in my case. The quality of my care was so poor that my thrush progressed to esophageal candidiasis before it was even diagnosed! Care to take a guess as to why? All because I was HIV test-negative. What about PCP? Systemic Candidiasis? Fungal infections of the skin? Chronic fungal sinusitis? All are extremely common in AIDS patients and I survived them all. Care to remind us again, why YOU are so eager to misinform others on this topic? I think I've made my motivations quite clear. If doctors and researchers stopped their profiteering long enough to connect the dots, I wouldn't have to spend my time helping others learn the truth. If any AIDS patients are reading this, I hope they will do their own research and definitely doctor-shop. It took me 8 months and numerous doctor visits to find one who would provide the comprehensive care I needed and who would prescribe the correct medication, a potent antifungal, at the correct dosage.
You and Richard Jefferys can call me a hypocrite till your blue in the face, but you do so only because you have no other answers for the questions that I have raised.
Kevin
If you closely read Lo's work, his peer reviewed reserach that I posted above and the several patents he filed called" pathenogenic mycoplasma" hes a very good scientist and took measures to make sure it wasnt a contaminent.
First of all he found it in 7 people who died of mysterious infections when no other microbe could be found. He identified it with electron microscopy. Secondly its unlikely that a contaminent would cause a fatal disease in mice and monkeys, and would also just happen to be a different strain that was not the same as other mycoplasmas that usually contaminate.
Lastly i believe while i was reading his patents that he had "control cultures" where no patient mycoplasma was added to the culture, if it was just a contaminent these cultures would have grown mycoplasma, and they didnt.
His new strain of mycoplasma just happened to be found in sick patients and not in controls. As far as lo's later work on antibodies to CFS, if you read Lo's earlier work this unique strain of mycoplasma didnt cause much of a immune response when they injected monkeys died with it, so looking for antibodies is not the way to go.
If you read project day lily www.projectdaylily.com you will find out why Lo spoke in riddles when it came to mycoplasma.
DR garth and nancy Nicolson phd had confidential sources within the pentagon that revealed that this was part of the bio weapons program. They are 2 respected scientists from respectable universities and i doubt they would make this up. When they were doing research on gulf war syndrome armed defense intelligence agents visited with them and threatened them to stop their research. their boss wass shot 5 times in the head when they were going to blow the whistle on illegal testing.
Anyways, im not a scientist, im just someone who was sick for years with a mysterious infection and am on the road to recovery because of Dr.lo and Dr. nicolsons research. There are many other sufferers of CFS etc that have a right to know this.
As far as the gilbert supporting bialy, my evidence for that was from the aids wiki. darin brown wrote this
"I might remind those reading that this is a serious offer from a respected scientist. Dr. Bialy has more than 30 years experience in molecular biology, has published several ground-breaking papers, and was the founding and scientific editor of the world's leading biotechnology journal for 14 years. His book has gathered praise from scientific luminaries such as George Miklos, Kary Mullis (Nobel Prize Chemistry), Gerald Pollack, Donald Miller, Walter Gilbert (Nobel Prize Chemistry), Charles Cantor, Gunther Stent, Sir. Henry Harris and Lynn Margulis."
I would ask you to check with him for his source, unless its an error i really dont know. All i know is that the medical establishment failed me, and had i known of this research many years ago I would have been cured by now.
Kevin, since your personal odyssey has taken you from the expensive macrolide antibiotics of Abbott to the expensive azole antifungals of Pfizer, I have to admit that I find your railing against medical professionals, scientists, and the pharmaceutical industry to be bizarre. The extrapolation of your situation to HIV infection and AIDS is, sadly, beyond bizarre; it's ignorant and suggests a chronic solipsism that I fear may more untreatable than your sinusitis. I don't think I need to ask if you've survived toxoplasmosis, CMV retinitis, disseminated mycobacterium avium complex, disseminated Kaposi's sarcoma, etc., all of which are also "extremely common in AIDS patients."
How much Diflucan are you taking nowadays? I hope your new doctor has discussed the potential consequences of azole antifungal overuse with you.
Since it (unsurprisingly!) got stuck in the spam filter, I should maybe note that I posted links to the studies that Andrew Maniotis falsely claims show a close correlation between CD4 counts and TLC:
http://scienceblogs.com/aetiology/2007/05/smallpox_still_takes_a_toll.p…
I apologize that a couple of the links seem to have broken, I can dredge up the cites if anyone wants them (I think the PubMed search terms I used were just total -or absolute - lymphocyte count, CD4 & correlation).
Dear All,
Dr, Lo wasn't the only one to suspect mycoplasm infections:
In a 1991 paper that was published in the journal, Virology (Laurent-Crawford, A. G., Krust, B., Muller, S., Rivière, Y., Rey-Cuillé, M.-A., Béhet, J.-M., Montagnier, L. & Hovanessian, A. G. The Cytopathic Effect of HIV is Associated with Apoptosis. Virol. 185:829-839, 1991), Montagnier and his colleagues not only denied the A,B,C's of "HIV" pathogenesis by asserting that PHA was essential for T-cell activation, but they suggested in addition, that mycoplasma played some role in "HIV" pathogenesis:
" in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, whereas maximal virus production occurred at Days 10-17."
Cell culturists know that mycoplasma infections generate confusion, because they exert cytoplathic effects on cells similar to the way the "AIDS-virus" is believed to act in humans. Cells become "weakened" by this infectious pathogen over time, but cells are not killed outright, as in lytic viral infections.
Cheers,
Andy
yes, dr. lo's work in 1990 was totally solid, there is not much more you can do to prove a microbe causes disease in humans. He made sure it wasnt a contaminent(see my previous post)
The scientists who visited lo to see his work were very impressed, the miami herald contacted fauci a year later and he, as usual sabatoged it. This microbe is being found in cfs/fibromyaligia by dr. garth nicolson with pcr and not in healthy controls, looking for antibodies is pointless, as Dr. lo showed, the animals that died with it showed weak/no antibody response.
The real reason this research gets condescendingly dismissed by mainstream docs is bc its not supported by big pharma. You can bet if merck got behind "mycoplasma" thats all we'd be hearing about. Take a look once more at Lo's research to see how a really good scientist operates......................compare this to Gallos original papers and its laughable, Lo had an animal model with a microbe that was present in sufficient quantities to cause disease, gallo had no animal model with a virus that was present in like 1 of 10,000 t cells.
Microbiology has been turned upside down, microbes w/o animal models and that are barely detectable are pushed on the public, and microbes with animal models where you can see the damage w electron microscopes are ignored!
Researchers at the U. S. Armed Forces Institute of Pathology (AFIP) in Washington, D. C., and the Warren Grant Magnuson Clinical Center at the National Institutes of Health, have found compelling evidence that a previously unrecognized opportunistic infection -- one potentially treatable with antibiotics -- may be a major cause of illness in people with AIDS. Many infections of organs including the brain, spleen, liver, or lymph nodes -- as well as some systemic infections -- might be caused by the newly-discovered organism, called Mycoplasma incognitus. Until now, these infections would be counted among the many which cannot be diagnosed.
While the first report of the organism now known as Mycoplasma incognitus was published over three years ago, most of what is now known was learned later and published last year. And only in the last few weeks has the AIDS research community paid serious attention. Until recently the new organism was mistakenly believed to be a virus, and its discovery seemed to have little immediate relevance to treatment.
Then a series of five articles by Shyh-Ching Lo and others in the American Journal of Tropical Medicine and Hygiene, between February and November 1989, showed:
(1) The new organism is a mycoplasma -- which is potentially treatable. Mycoplasma, a form of life between bacteria and viruses in complexity, was discovered about 100 years ago. Some species are known to cause human diseases.
The published articles only hint that the new organism might be treatable with antibiotics. But scientists at AFIP tested 15 common antibiotics against the Mycoplasma incognitus in the laboratory. A detailed report is being prepared for publication, but because of the public-health importance of the information, AFIP released a list of the drugs and their effective concentrations in a separate document. Doxycycline, tetracycline, clindamycin, lincomycin, and ciprofloxacin were found to be effective against Mycoplasma incognitus. But erythromycin, the antibiotic most commonly used to treat mycoplasma infections, was not effective -- and penicillin, streptomycin, gentamicin, and others also had no effect.
(2) Mycoplasma incognitus was found in the thymus, liver, spleen, lymph node, or brain of 22 of 34 persons who had died of AIDS. The patients who were selected for this autopsy study had all had evidence of organ failures.
(3) In a separate study with different patients, the mycoplasma was found in seven of ten persons with AIDS. Also, a much earlier study had found Mycoplasma incognitus in blood lymphocytes of 12 of 23 living persons with AIDS -- but in none of 22 healthy blood donors used as controls.
(4) The mycoplasma was also found in six HIV-negative patients (with no sign of AIDS) from different parts of the world, who had died in one to seven weeks of an undiagnosed infection.
No one knows how the organism spreads, but evidently it is not by casual contact, as family members of infected persons have not become infected themselves.
(5) Four monkeys were injected with Mycoplasma incognitus; all died in seven to nine months. The organism was found in the spleens of all the monkeys, and in some other organs as well. It was not found in a fifth monkey tested as a control.
(6) Extensive evidence from electron-microscope examinations, from specially designed PCR tests to look for the DNA of Mycoplasma incognitus, and from immunologic tests, showed that the organism was concentrated in lesions in affected organs. Mycoplasma incognitus is unusual in that it often infects and kills tissue without causing an inflammatory reaction, suggesting that it disables or evades part of the immune system.
The publication of this evidence, much of it in November 1989, led to a meeting between Dr. Anthony Fauci, director of NIAID (the National Institute of Allergy and Infectious Diseases) and other AIDS experts, with Dr. Lo and his colleagues at AFIP. The meeting, on December 14, 1989 in San Antonio, was chaired by Dr. Joel B. Baseman, chairman of the Department of Microbiology at the University of Texas Health Sciences Center in San Antonio, an expert on mycoplasma. An article in THE WASHINGTON POST (January 5) quoted Dr. Baseman as saying that Lo's mycoplasma "might be a significant agent for many infectious diseases, not just AIDS. There is enough information to say that this agent is real." The same article quoted Dr. Fauci as saying that Mycoplasma incognitus "may be an important opportunistic infection ...If it's real, it could have an important impact on how doctors look at AIDS patients with unexplained problems."
Sometimes I love denialists for how they make me laugh. Forty or frummy or cooler or Andy's Defender or someone says Walter Gilbert wrote a glowing review of Harvey Bialy's book about himself you know the one where he said some things about Duesberg too. Where can we find the review? Well we can ask Mr. Revolver Daren Brown who once wrote, a long list of people said good things about Bialy's book!
So we take Mule's word that Daren Brown said something and then we take Brown's word that Gilbert wrote something I can't find on the internet. And then we say if Gilbert ever said anything good about Bialy, he must be a total AIDS denialist! From there it's not a jump to say the CIA invented influenza and polio comes from looking at autumn leaves.
Kevin, I'm glad your doing better now but what matters in medicine is double blinded placebo controlled studies verified and peer reviewed and there's not even one of those proving antifungals help people with CRS. In fact there are three proving just the opposite for amphotericin B, and more with other antifungals, cited by me above. Maybe some antifungals could help CRS. I hope more studies come out soon to clear up things.
Meanwhile your press release or popular news article doesn't have much weight compared with peer-reviewed scientific evidence. Nothing personal, but on a science blog you should be able to give some science not a journalist's version of a press release.
I enjoyed the description of Garth and Nancy Nicolson too. Did you know their cat died of a mysterious illness so they dicided it had Gulf War syndrome. I'm not sure if it was a Apache pilot or if it was on the ground over there. But anyway little Fluffy got Gulf War and died so the Nicolsons started a "Institute for Molecular Medicine" and they found mycoplasma in HALF of samples from vets with Gulf War syndrome. Wonder why the AIDS denialists are ok with that? But anyway it gets better since they discovered mycoplasma was ENGINEERED and it had a "piece of HIV" in it whatever that means. George Bush and James Baker did it and Bill Clinton helped them cover it up. They got rich selling it to Saddam who used it in Desert Storm. I don't know why but Clinton thought he had to conceal it so he sent troops to threaten scientists who were getting close to the truth. I guess to protect his friends the Bushes. Whenever someone gets shot it's because of the men from the black helicopters. And then George Bush didn't even mention that mycoplasma as a WMD! Talk about a slam dunk I mean this stuff is so obvious! Meantime they've put mycoplasma in all the vaccines to control the world's population. I just can't see how anyon'es still alive.
Fruit. Cakes. All of 'em.
Bonehead,
whats the first scientific paper that proves hiv causes aids?
how does hiv cause organ failure when its only present in all small number of tcells? (1 in 100 or so)
I clearly proved lo's mycoplasma was not a contaminent, and you try to get me on technicality. People are rotting away with CFS and other chronic illnesses and deserve to know that there is a microbe in their body that DR. garth nicolson found with PCr that not usually found in healthy controls, a microbe that DR.lo proved caused a fatal illness in animals.
Whats wrong with giving patients who pay your salaries informed consent? you cant do that because most people would reject the hiv hypothesis, reject taking in toxic levels of mercury and would worry about real microbes like mycoplasma. YOu must only tell them one side of the story to do the bidding of the drug companies that own you.
The peer review process is totally rigged, did it save americans from the 100,000 people that died from vioxx? If we took these scientific arguments to the public in a trial with a scientific jury you criminals that pump kids with 100 times the epa safe level of mercury, when every other developed nation banned thimerosol, you guys would probably get thrown in jail.
Dr. garth nicolson was made an honorary navy seal because the vetarans appreciated his help so much. ARe gulf war veterans lying when they say their illness was contagious and they passed it to thier families? What have you done to help sick people?
Dr. lo folfilled kochs postulates more than your idol gallo did (it wasnt a contaminent), he had an animal model with a microbe that was present in quantities visible with the electron microscope, not only a correlation with microbe with no animal model that was barely present,( in only a tiny fraction of tcells)
Microbiology has been turned upside down, Koch is rolling over in his grave. Keep up the good work, just keep the debate out of the publics eye, thats the only way you can win.
Sorry everyone but it's just too good.
Frums I don't know what you mean by proof but you can believe whatever you want.
Frummy/Cooler also goes by BillyBipBip and is a 911 conspiracy theorist along with vax HIV and Gulf War illness. Now I wonder what Frummy thinks about the Holocaust. Maybe the result of pesticides?
Drs Garth and Nancy aren't just the worlds greatest scientists and honorary members of the Imperial Guard, they also warned the Pentagon in August of 2001 they would be attacked by terrorists on September 11. On a canadian site called "natural-person" it says their sources for this remarkable info were "individuals in key intelligence positions, the MOB, and one high level African diplomat". Other places say it was "special forces" people who were Dr. Nicolson's patients.
Then the Nicolsons told the "Director of Policy" at the Department of Defense although I don't think there is such a position. Also the Inspector General of the Army Medical Corps and probably one of the drive through people at their local Jack in the Box.
Sadly no one listened to the Nicolsons. Or to the other guy who warned about 911 a internet prophet who was warning "sinners" to abandon "Metropolis" since 1975. Prescient, wasn't he?
Kevin, how do you think they treat AIDS patients with fungal OIs?
With antifungals.
Take it to the next step. If AIDS was caused by fungi, any AIDS patient receiving antifungals would clear up like you did.
Furthermore, what do you think they treated fungal diseases with in the AIDS cases before HIV was discovered? Antifungals.
You didn't have HIV, and AIDS patients do, explaining why antifungals worked for you, but don't for them.
Furthermore, AIDS patients also have other disorders completely unrelated to fungal infections, so your hypothesis fails on two fronts.
You should be pleased that one of the better online catalogs of evidence based medicine includes remarks on fungal causes of sinus infections (free subscription required). The problem here isn't pharmaceutical companies, it is that there is so much information out there that even the most up to date MD or DO can't be up to date on everything.
You found one that was up to date on what you needed, and I don't fault you for seeking care from someone that listened to your concerns. Doctors with poor interpersonal communication skills are a scourge on the medical community. Luckily, most hospitals require communications classes for their graduates. [joke]Doctors who can't communicate become surgeons.[/joke]
lol, no evidence just ad hominem attacks. If you are so confident of your views, yet you do everything from letting the public hear both sides of a scientific argument. thats pretty suspect, if you had an open debate on any issue weve been discussing, youd lose.
Thanks for not anwering my questions about hiv and Lo's solid work, just proves my point. I suggest you stop trying to be a satirist, youre not that funny. LOL
Cooler,
What was ad hom? Are you a 911 conspiracy theorist? You are, and that's relevant to the debate because like I said people who have bizarre views on one thing often have them on other things too, so that's not an ad hominem. You might prefer a different name but that's what most people would call you.
Anything I said about the Nicolson's was wrong? Ok, "Jack in the Box" was humor but the rest I just found on web sites run by people who think like you. Even the part about their cat! Again, not ad hominem.
You want a debate? Chris Noble gave it to you. He gave you papers proving your interpretation of Lo and Nicolson is wrong. Even Lo says it. Here's the quote.
"Thus, there is no serological evidence that suggests infection by M. fermentans is associated with development of 'Gulf War illness'."
That's from the 2000 Epidemiol Infect. article by Dr. Lo that Chris Noble kindly gave you. No one is stopping debate here.
Have you written Dr. Lo? Because I don't think Dr. Lo says Mycoplasma causes AIDS either. Like Chris said.
Cooler doesn't it matter to you or don't you know that Dr. Lo's three monkeys didn't have the usual symptoms of simian AIDS. Doesn't it matter to you, Dr. Lo's own statements question what you're saying?
I told you every animal/ patient that died from lo's initial study did not have an antibody reponse, you have to look for it with pcr like nicolson and other scientists have.
Serology is meaningless.
If mycoplasma is not a cause of human disease, why did lo find it to be the cause of disease in 7 hiv negative people who died of a mysterious infection?
here is what lo said in 1990 , i wonder what he thinks now..................
"There is no good explanation for why and how the virus breaks out of the antibody protection," says Lo. "I'm not saying that HIV plays no role in AIDS -- the data shows a clear correlation with disease. But AIDS is much more complicated than HIV."
"In the spirit of "the openness" of science we salute Peter Duesberg for his challenging and courageous voice speaking out against the present scientific establishment. His extensive experience and knowledge about retroviruses lends merit to his critical evaluation of the possible causative role of HIV in the AIDS disease.
We believe the most healthy and responsible scientific attitude in dealing with AIDS research is to explore all possible avenues. To make any conclusion lightly or prematurely, such as ruling out any possible role of microbes in AIDS, or to commit oneself exclusively to a particular agent and completely rule out any other possible role of a different microbe, may all result in a greater loss of AIDS victims."
Shyh-Ching Lo M.D PHd
Chief, Division of Geographic Pathology
Col. Douglas J. Wear, MC USA
Chairman
Department of Infectious and Parasitic Disease Pathology
Department of Defense
Armed Forces Institute of pathology
Washington, DC
Anyways at least good old andy agrees with some of what i say............hes my new friend LOL
I told you every animal/ patient that died from lo's initial study did not have an antibody reponse, you have to look for it with pcr like nicolson and other scientists have. Serology is meaningless.
Lo would disagree. How did Lo know his six patients had Mycoplasma? By using antibodies.
"immunohistochemistry using rabbit antiserum raised against VLIA, the virus-like infectious agent previously identified in patients with AIDS and shown to cause fatal systemic infection in primates, revealed VLIA antigens in these necrotizing lesions." Lo et al Am. J. Trop. Med. Hyg. 1989 Sep;41(3):364-76.
What about those monkeys? All of them had some kind of antibody response. One had "a prominent antibody response" the other three had "transient or poor" response. But they all did respond. Lo et al Am. J. Trop. Med. Hyg. 1989 Apr;40(4):399-409.
Serology is one of Lo's main tools in all the papers.
If mycoplasma is not a cause of human disease, why did lo find it to be the cause of disease in 7 hiv negative people who died of a mysterious infection?
Did Lo really "find it to be the cause?" Maybe it was but Lo found evidence Mycoplasma was present, assuming it wasn't contam, but that's not proof it CAUSED anything. Like Kevin's Mayo study. Finding fungus in 96% of sick people doesn't mean it's CAUSING anything especially when you find it in 100% of healthy people. Interesting study but not proof of cause.
I don't think anyone here disagrees fungi could contribute to chronic sinusitis and I don't question some Mycoplasma could do bad stuff to people. CFS and other conditions might have some component of it. But Mycoplasma no matter what species doesn't cause AIDS. HIV causes AIDS.
Take it to the next step. If AIDS was caused by fungi, any AIDS patient receiving antifungals would clear up like you did. --- Robster
Finally, you offer an insightful comment...
I don't have time to answer fully, at the moment, but the short answer is that they are not being treated for long enough, nor with high enough dosages--not to mention, the other factors necessary are also not being addressed. Nevertheless, my treatment required 500mg/day for 16 weeks, with a small "treatment break" after every 4 weeks; thus, I was in treatment for a total of 20 weeks, with four breaks. Most doctors will only prescribe diflucan for 200mg/day (at most) and usually for only 4 weeks, which may clear up a case of oral thrush but the systemic infection remains, and will come roaring back once treatment ends. For most AIDS patients, thrush is a constant battle. Resistance then becomes a problem. Candida can be quite pernicious, if treated incompletely. In fact, even with extensive treatment, mine came back twice after the initial success but was easily treated with much lower dosages both times. In addition, my health, though still compromised during the recurrences, continued to improve.
The adjunctive therapies of strict dieting (no simple carbs and no processed foods, etc) and massive probiotic supplementation are equally necessary. Patients should also be on extensive vitamin and mineral programs aimed at boosting the immune system. Stress-reduction is equally important as an antifungal, i.e. telling someone they are going to die from a mysterious, killer virus will make recovery damn near impossible.
Lastly, I realize that these drugs are dangerous. My doctor performed liver function tests frequently, and I thankfully never developed any side effects, i.e. no "buffalo humps" or lipodystrophy and we all know why. Diflucan and other anti-fungals can certainly cause liver failure, though rare, but they are far safer than most of the HAART medications, even at such high dosages, and 16 weeks is incredibly less "treatment time" than life-long therapy. Do you not agree?
Furthermore, AIDS patients also have other disorders completely unrelated to fungal infections, so your hypothesis fails on two fronts.
Your analysis is incomplete and my hypothesis has not failed. In fact, I personally know 3 other patients, two positive/one also negative, who have dramatically improved their health from this protocol. One was even sicker than I was. As for the other disorders that you and Richard Jefferys allude, improperly treated, or even worse, untreated systemic fungal infections will significantly compromise one's immune system and more serious infections naturally may follow...
Kevin
Like Kevin's Mayo study. Finding fungus in 96% of sick people doesn't mean it's CAUSING anything especially when you find it in 100% of healthy people. Interesting study but not proof of cause.
Oh Adele, what grade are you in? Or, are you actually an adult who just reads at the 6th grade level?
The website that I posted previously contained far more than press releases, which is more than one can say for most of the claims made by HIV scientists. HIV/AIDS has been "science by press release for nearly 20 years". Nevertheless, each section of the website is very well-referenced. Here are just a few examples from the Etiology Sub-page:
References
1. Ponikau JU, Sherris DA, Kern EB et al. The diagnosis and incidence of allergic fungal sinusitis. Mayo Clin Proc. 1999;74:877-84.
[View Article (PDF)]
2. Shin SH, Ponikau JU, Sherris DA, et al. Chronic rhinosinusitis: An enhanced immune response to ubiquitous airborne fungi. J Allergy Clin Immunol.; 2004;114(6):1369-75.
3. Ponikau JU, Sherris DA, Kephart GM, et al. Features of airway remodeling and eosinophilic inflammation in chronic rhinosinusitis: Is the histopathology similar to asthma? J Allergy Clin Immunol. 2004;114(6):1369-75.
4. Taylor MJ, Ponikau JU, Sherris DA, et al. Detection of fungal organisms in eosinophilic mucin using a fluorescein-labeled chitin-specific binding protein. Otolaryngol Head Neck Surg. 2002;127:377-83.
[View Article (PDF)]
5. Braun H, Buzina W, Freudenschuss K, et al. Eosinophilic fungal rhinosinusitis: a common disorder in Europe? Laryngoscope. 2003;113(2):264-9.
6. Gosepath J, Brieger J, Vlachtsis K, et al. Fungal DNA is present in tissue specimens of patients with chronic rhinosinusitis. Am J Rhinology. 2004;18(1):9-13.
__________________________________
I encourage you to read through them all, if you must, for I know you pretend to be quite the "reading superhero", but let me save you the trouble; the research, first pioneered at the Mayo Clinic way back in 1999, has proven to anyone capable of analytical thought that most cases of chronic sinusitis are indeed caused by fungi. You're simply being a pathetic sore-loser, at this point. Nevertheless, even if there weren't dozens of studies that support the fungal connection, I know how true it is because my quality of life has been dramatically altered because of these findings and so have thousands of others--those lucky enough to have quality caregivers (mostly in Europe).
You lost this one, Adele. It's okay...you're still a valuable contributor to science in your role as monkey-poo slide technician; I'm quite sure of that.
Kevin
Dear Adele,
I didn't hear if you chanted your mantra today? Well, did you?
RE:
"But Mycoplasma no matter what species doesn't cause AIDS. HIV causes AIDS."
HIV causes AIDS..HIV causes AIDS...HIV causes AIDS...
Unless of course you buy into Fauci's extreme form of AIDS denialism...
IDIOPATHIC CD4+ T-LYMPHOCYTOPENIA - ICL
("MYSTERIOUS" AIDS CASES)
Is HIV the primary and sole cause of AIDS?
A substantial literature exists documenting that a number of patients present themselves to clinicians with signs and symptoms consistent with the so-called "AIDS defining illnesses." The defining key phrase on Medline is "T-Lymphocytopenia, Idiopathic CD4-Positive" and is often referred to as "ICL." The extraordinary feature of this patient group is that they test negative for HIV. The clinical spectrum is considered diverse and is characterized by opportunistic infections caused by one or more mycotic, bacterial and viral infections. Less frequently parasitic infections are seen. Serologic tests for HIV-1 infection are negative when a screening and confirmatory test are used. In such patients no known cause of immunodeficiency is apparent, nor should it result from immunosuppressive therapy.
I have just pasted a few reports below published over a several year period. These papers were written by deluded doctors, scientists (and their substantially numerous co-authors who should have at least stopped the publication of these reports), who were deluded into believing that "HIV/AIDS" is NOT a distinct disease, and who believed that great AIDS denialist, Anthony Fauci, who said, ICL is just AIDS without any "HIV" in it...
1993
Ostrowski, M., I. E. Salit, W. L. Gold, D. Sutton, M. L. Montpetit, D. Lepine, and T. Salas. 1993. Idiopathic CD4+ T-lymphocytopenia in two patients. Cmaj. 149(11):1679-83.
Dunn, D., and M. L. Newell. 1993. Idiopathic CD4+ T lymphocytopenia. Pediatr Infect Dis J. 12(8):705.
Tindall, B., J. Elford, T. Sharkey, A. Carr, J. Kaldor, and D. A. Cooper. 1993. CD4+ lymphocytopenia in HIV-seronegative homosexual men [letter]. Aids. 7(9):1272-3.
Cathebras, P. J., K. Bouchou, and H. Rousset. 1993. Pulmonary Mycobacterium avium intracellulare with transient CD4+ T- lymphocytopenia without HIV infection [letter]. Eur J Med. 2(8):509-10.
Spira, T. J., B. M. Jones, J. K. Nicholson, R. B. Lal, T. Rowe, A. C. Mawle, C. B. Lauter, J. A. Shulman, and R. A. Monson. 1993. Idiopathic CD4+ T-lymphocytopenia--an analysis of five patients with unexplained opportunistic infections. N Engl J Med. 328(6):386-92.
Duncan, R. A., C. F. von Reyn, G. M. Alliegro, Z. Toossi, A. M. Sugar, and S. M. Levitz. 1993. Idiopathic CD4+ T-lymphocytopenia--four patients with opportunistic infections and no evidence of HIV infection. N Engl J Med. 328(6):393-8.
Smith, D. K., J. J. Neal, and S. D. Holmberg. 1993. Unexplained opportunistic infections and CD4+ T-lymphocytopenia without HIV infection. An investigation of cases in the United States. The Centers for Disease Control Idiopathic CD4+ T-lymphocytopenia Task Force [see comments]. N Engl J Med. 328(6):373-9.
Ho, D. D., Y. Cao, T. Zhu, C. Farthing, N. Wang, G. Gu, R. T. Schooley, and E. S. Daar. 1993. Idiopathic CD4+ T-lymphocytopenia--immunodeficiency without evidence of HIV infection. N Engl J Med. 328(6):380-5.
Laurence, J. 1993. T-cell subsets in health, infectious disease, and idiopathic CD4+ T lymphocytopenia [see comments]. Ann Intern Med. 119(1):55-62.
Kaiser, F. E., and J. E. Morley. 1994. Idiopathic CD4+ T lymphopenia in older persons. J Am Geriatr Soc. 42(12):1291-4.
Grossman, D., D. E. Lewis, Z. K. Ballas, and M. Duvic. 1994. Idiopathic CD4+ T lymphocytopenia in a patient with mycosis fungoides [see comments]. J Am Acad Dermatol. 31(2 Pt 1):275-6.
McLane, N. J., J. J. Weems, Jr., and M. V. Antworth. 1994. Cytomegalovirus retinitis in a patient with idiopathic CD4+ T lymphocytopenia [letter]. Clin Infect Dis. 18(6):1012-3.
Holland, S. M., E. M. Eisenstein, D. B. Kuhns, M. L. Turner, T. A. Fleisher, W. Strober, and J. I. Gallin. 1994. Treatment of refractory disseminated nontuberculous mycobacterial infection with interferon gamma. A preliminary report. N Engl J Med. 330(19):1348-55.
Heredia, A., B. Joshi, S. H. Weiss, S. F. Lee, J. Muller, K. L. Poffenberger, J. Quirinale, J. S. Epstein, and I. K. Hewlett. 1994. Absence of evidence of retrovirus infection in intravenous drug users with idiopathic CD4+ lymphocytopenia [letter]. J Infect Dis. 170(3):748-9.
Burg, S., W. Weber, and C. Kucherer. 1994. [Idiopathic CD4 lymphocytopenia with lethal Salmonella typhimurium sepsis]. Dtsch Med Wochenschr. 119(27):956-8.
Baumgarten, R., and R. von Baehr. 1994. [Idiopathic CD4 T-lymphocytopenia. Case follow-up over 5 years]. Z Arztl Fortbild (Jena). 88(5-6):429-32.
Heredia, A., I. K. Hewlett, V. Soriano, and J. S. Epstein. 1994. Idiopathic CD4+ T lymphocytopenia: a review and current perspective. Transfus Med Rev. 8(4):223-31.
Laraque, F., and D. Sosin. 1994. Idiopathic CD4+ lymphocytopenia in New Jersey. N J Med. 91(9):604-6.
Dine, G., S. Brahimi, B. Culioli, and Y. Rehn. 1994. [Idiopathic T+CD4 lymphocytopenia: an asymptomatic form followed-up for two years (letter)]. Presse Med. 23(9):447.
Lin, J. C., and H. M. Tripathi. 1994. Pure red cell aplasia and idiopathic CD4 T-lymphocytopenia [letter]. Clin Infect Dis. 18(4):651-2.
Griffiths, T. W., S. R. Stevens, and K. D. Cooper. 1994. Acute erythroderma as an exclusion criterion for idiopathic CD4+ T lymphocytopenia. Arch Dermatol. 130(12):1530-3.
Kaczmarski, R. S., A. D. Webster, J. Moxham, F. Davison, S. Sutherland, and G. J. Mufti. 1994. CD4+ lymphocytopenia due to common variable immunodeficiency mimicking AIDS. J Clin Pathol. 47(4):364-6.
Heredia, A., J. Muller, V. Soriano, S. F. Lee, A. Castro, J. Pedreira, K. L. Poffemberger, J. Epstein, and I. K. Hewlett. 1994. Absence of evidence of retroviral infection in idiopathic CD4+ T- lymphocytopenia syndrome [letter]. Aids. 8(2):267-8.
Dev, D., G. S. Basran, D. Slater, P. Taylor, and M. Wood. 1994. Immunodeficiency without HIV. Consider HIV negative immunodeficiency in cryptococcosis [letter; comment]. Bmj. 308(6941):1436.
Deng, G. H., and A. X. Wang. 1994. [Idiopathic CD(4+)-positive T-lymphocytopenia]. Chung Hua Nei Ko Tsa Chih. 33(3):208-10.
Famularo, G., R. Giacomelli, C. De Simone, and G. Tonietti. 1994. The syndrome of idiopathic CD4+ lymphocytopenia. Ann Ital Med Int. 9(1):22-6.
Seligmann, M., B. Autran, C. Rabian, F. Ferchal, D. Olive, M. Echard, and E. Oksenhendler. 1994. Profound and possibly primary "idiopathic CD4+ T lymphocytopenia" in a patient with fungal infections. Clin Immunol Immunopathol. 71(2):203-7.
Park, K., B. J. Monk, S. Wilczynski, J. I. Ito, Jr., and S. A. Vasilev. 1994. Idiopathic CD4+ T-lymphocytopenia and recurrent vulvar intraepithelial neoplasia. Obstet Gynecol. 84(4 Pt 2):712-4.
Wakeel, R. A., S. J. Urbaniak, S. S. Armstrong, H. F. Sewell, R. Herriot, N. Kernohan, and M. I. White. 1994. Idiopathic CD4+ lymphocytopenia associated with chronic pruritic papules. Br J Dermatol. 131(3):371-5.
Ohashi, D. K., J. S. Crane, T. J. Spira, and M. L. Courrege. 1994. Idiopathic CD4+ T-cell lymphocytopenia with verrucae, basal cell carcinomas, and chronic tinea corporis infection. J Am Acad Dermatol. 31(5 Pt 2):889-91.
Thomas, D., D. Leslie, P. Stanley, and B. Clarke. 1994. Disseminated Mycobacterium avium-intracellulare infection in an HIV- negative male. Aust N Z J Med. 24(4):403.
Monteil, M. A., D. C. Henderson, and S. Obaro. 1994. Immunodeficiency without HIV. Clinical presentation vary [letter; comment]. Bmj. 308(6941):1436.
Piketty, C., L. Weiss, and M. Kazatchkine. 1994. [Idiopathic CD4 lymphocytopenia (editorial) (see comments)]. Presse Med. 23(30):1374-5.
Stasi, R., G. Delpoeta, A. Venditti, U. Coppetelli, M. Masi, and G. Papa. 1994. Clinical heterogeneity of idiopathic CD4+ T lymphocytopenia [letter]. J Intern Med. 235(1):92-3.
McNulty, A., J. M. Kaldor, A. M. McDonald, K. Baumgart, and D. A. Cooper. 1994. Acquired immunodeficiency without evidence of HIV infection: national retrospective survey [see comments]. Bmj. 308(6932):825-6.
Wortley, P. M., and S. D. Holmberg. 1994. No evidence of blood-borne transmission of idiopathic CD4+ T- lymphocytopenia [letter]. Transfusion. 34(6):556.
Girotto, M., D. A. Verani, and P. P. Pagliaro. 1994. Idiopathic CD4+ T-lymphocytopenia in blood donors: cohort study [letter]. Transfusion. 34(10):935-6.
Djomand, G., L. Diaby, J. M. N'Gbichi, D. Coulibaly, A. Kadio, A. Yapi, J. M. Kanga, E. Boateng, K. Diallo, L. Kestens, and et al. 1994. Idiopathic CD4+ T-lymphocyte depletion in a west African population. Aids. 8(6):843-7.
Grosshans, E. 1994. [HIV seronegative human immunodeficiency syndrome (letter; comment)]. Presse Med. 23(39):1833.
1995
Vertes, D., M. D. Linden, and J. L. Carey. 1995. Idiopathic CD4+ T-lymphocytopenia: analysis of a patient with selective IgA deficiency and no evidence of HIV infection. Cytometry. 22(1):40-4.
Seddon, M., and R. B. Ellis-Pegler. 1995. Idiopathic CD4+ T-lymphocytopenia: case report [letter]. N Z Med J. 108(997):134.
Sanchez Roman, J., M. J. Castillo Palma, R. Torronteras Santiago, and M. T. Pastor Ramos. 1995. [A new case of idiopathic T CD4+ lymphocytopenia and opportunistic infection without HIV infection (letter)]. Med Clin (Barc). 104(5):198-9.
Richert, S. M., and J. L. Orchard. 1995. Bacterial esophagitis associated with CD4+ T-lymphocytopenia without HIV infection. Possible role of corticosteroid treatment. Dig Dis Sci. 40(1):183-5.
Rhew, D. C., M. B. Goetz, and M. H. Louie. 1995. Reversible CD4+ T lymphocyte depletion in a patient who had disseminated histoplasmosis and who was not infected with human immunodeficiency virus [letter]. Clin Infect Dis. 21(3):702-3.
Pohl, W., C. Armbruster, K. Bernhardt, M. Drlicek, and N. Vetter. 1995. [Idiopathic CD4+ T-lymphocytopenia in 2 patients without indications for HIV infection]. Wien Klin Wochenschr. 107(3):95-100.
O'Brien, T. R., L. Diamondstone, M. W. Fried, L. M. Aledort, S. Eichinger, M. E. Eyster, M. W. Hilgartner, G. White, A. M. Di Bisceglie, and J. J. Goedert. 1995. Idiopathic CD4+ T-lymphocytopenia in HIV seronegative men with hemophilia and sex partners of HIV seropositive men. Multicenter Hemophilia Cohort Study. Am J Hematol. 49(3):201-6.
Neumeister, B., T. M. Zollner, D. Krieger, W. Sterry, and R. Marre. 1995. Mycetoma due to Exophiala jeanselmei and Mycobacterium chelonae in a 73- year-old man with idiopathic CD4+ T lymphocytopenia. Mycoses. 38(7-8):271-6.
Neukirch, B., and G. J. Kremer. 1995. [Disseminated extrapulmonary tuberculosis in idiopathic CD4- lymphocytopenia]. Dtsch Med Wochenschr. 120(1-2):23-8.
Lobato, M. N., T. J. Spira, and M. F. Rogers. 1995. CD4+ T lymphocytopenia in children: lack of evidence for a new acquired immunodeficiency syndrome agent. Pediatr Infect Dis J. 14(6):527-35.
Kirtava, Z., J. Blomberg, A. Bredberg, G. Henriksson, L. Jacobsson, and R. Manthorpe. 1995. CD4+ T-lymphocytopenia without HIV infection: increased prevalence among patients with primary Sjogren's syndrome. Clin Exp Rheumatol. 13(5):609-16.
Frassanito, M. A., G. Iodice, R. Rizzi, and F. Dammacco. 1995. [Idiopathic CD4+ lymphocytopenia: a case report]. Ann Ital Med Int. 10(3):188-92.
Quiles, I., P. Anaut, F. Cibrian, J. Gainzarain, L. Vega, and A. Andia. 1995. Idiopathic CD4+ T-lymphocytopenia with opportunistic infection and non- Hodgkin's lymphoma [letter]. J Intern Med. 238(2):183-4.
Confalonieri, M., S. Aiolfi, L. Gandola, A. Scartabellati, A. Colavecchio, G. Cannatelli, and A. Mazzoni. 1995. [Disseminated histoplasmosis and idiopathic CD4+ T-lymphocytopenia. An autochthonous Italian case (letter)]. Presse Med. 24(9):459.
Dupon, M., M. Bonnefoy, P. A. Bohu, M. Pinsard, B. Dumon, and H. Fleury. 1995. [Idiopathic CD4 lymphocytopenia syndrome disclosed by meningeal cryptococcosis. A new case (letter; comment)]. Presse Med. 24(37):1752.
Caminal Montero, L., D. Ramos Barbon, J. Ferro Mosquera, and J. B. Diaz Lopez. 1995. [CD4+ lymphocytopenia and sarcoidosis (letter; comment)]. Med Clin (Barc). 105(4):158.
Sanchez Roman, J.,M. J. Castillo Palmo, C. Rey Romero, and M. D. Mendoza Muro. 1995. [Idiopathic T CD4+ lymphocytopenia and opportunistic infection without human immunodeficiency virus infection (letter)]. Rev Clin Esp. 195(2):127-8.
Calderon, E., B. Sanchez, F. J. Medrano, P. Stiefel, and M. Leal. 1995. CD4+ T-lymphocytopenia in the elderly [letter]. Eur J Clin Microbiol Infect Dis. 14(1):75-7.
Blum, A., and B. Shohat. 1995. CD-4 lymphopenia induced by streptokinase [letter; comment]. Circulation. 91(6):1899.
Ferrer, X., C. Vital, M. Larriviere, S. Richard, and J. Julien. 1995. Idiopathic CD4+ T-cell lymphocytopenia and subacute inflammatory demyelinating polyradiculoneuropathy. Neurology. 45(1):196-7.
1996
Urnovitz, H.B. and R. W. Stevens. 1995. AIDS research priorities [letter; comment] [published erratum appears in Science 1995 Mar 24;267(5205);1753]. Science. 267(5202):1249-50.
Belmin, J., M. N. Ortega, A. Bruhat, A. Mercadier, and P. Valensi. 1996. CD4 lymphopenia in very elderly people [letter] [see comments]. Lancet. 347(8997):328-9.
Anzalone, G., M. Cei, A. Vizzaccaro, B. Tramma, and A. Bisetti. 1996. M. Kansasii pulmonary disease in idiopathic CD4+ T-lymphocytopenia. Eur Respir J. 9(8):1754-6.
Zollner, T. M., S. Stracke, B. Neumeister, B. Manfras, W. Boehncke, B. O. Boehm, R. Marre, and W. Sterry. 1996. Idiopathic CD4+ T lymphocytopenia presenting as mycetoma in a patient with a mutation in the cystic fibrosis transmembrane regulator gene [letter]. Arch Dermatol. 132(10):1247-9.
Yonetsu, M., K. Sato, T. Michimata, T. Sekiguchi, M. Mori, K. Hoshino, and H. Murakami. 1996. [Case of idiopathic CD4+T-lymphocytopenia complicated by Mycobacterium avium infection]. Nippon Naika Gakkai Zasshi. 85(8):1293-4.
Wolf, P., R. Mullegger, L. Cerroni, R. Aigner, G. Fueger, G. Hofler, J. Derbaschnig, and H. Kerl. 1996. Photoaccentuated erythroderma associated with CD4+ T lymphocytopenia: successful treatment with 5-methoxypsoralen and UVA, interferon alfa- 2b, and extracorporeal photopheresis. J Am Acad Dermatol. 35(2 Pt 2):291-4.
Sinicco, A., A. Maiello, R. Raiteri, M. Sciandra, G. Dassio, C. Zamprogna, and B. Mecozzi. 1996. Pneumocystis carinii in a patient with pulmonary sarcoidosis and idiopathic CD4+ T lymphocytopenia. Thorax. 51(4):446-7: discussion 448-9.
Rodot, S., J. P. Lacour, L. Van Elslande, and J. P. Ortonne. 1996. [Idiopathic CD4 lymphocytopenia]. Ann Dermatol Venereol. 123(12):852-6.
Rijnders, R. J., I. E. van den Ende, and F. J. Huikeshoven. 1996. Suspected idiopathic CD4+ T-lymphocytopenia in a young patient with vulvar carcinoma stage IV. Gynecol Oncol. 61(3):423-6.
Reichart, P. A., H. D. Pohle, and H. R. Gelderblom. 1996. Oral manifestations in a patient with idiopathic CD4+ lymphocytopenia. Int J Oral Maxillofac Surg. 25(4):290-2.
Pohl, W. 1996. [A patient with idiopathic bronchiolitis obliterans with organizing pneumonia and idiopathic CD4+ T-lymphocytopenia]. Wien Klin Wochenschr. 108(15):473-7.
Petersen, E. J., M. Rozenberg-Arska, A. W. Dekker, H. C. Clevers, and L. F. Verdonck. 1996. Allogeneic bone marrow transplantation can restore CD4+ T-lymphocyte count and immune function in idiopathic CD4+ T-lymphocytopenia. Bone Marrow Transplant. 18(4):813-5.
Paolini, R., E. D'Andrea, A. Poletti, A. Del Mistro, P. Zerbinati, and A. Girolami. 1996. B non-Hodgkin's lymphoma in a haemophilia patient with idiopathic CD4+ T-lymphocytopenia. Leuk Lymphoma. 21(1-2):177-80.
Navarro, V., C. Tuset, and C. Gimeno. 1996. [T CD4+ lymphocytopenia syndrome without human immunodeficiency virus (HIV) infection. Study on 4 patients (letter)]. Med Clin (Barc). 107(4):157.
Michel, J. L., J. L. Perrot, D. Mitanne, S. Boucheron, L. Fond, and F. Cambazard. 1996. [Metastatic epidermoid carcinoma in idiopathic CD4+ T lymphocytopenia syndrome]. Ann Dermatol Venereol. 123(8):478-82.
McBride, M. 1996. CD4 lymphopenia in elderly patients [letter; comment]. Lancet. 347(9005):911; discussion 912.
Laurence, J., D. Mitra, M. Steiner, D. H. Lynch, F. P. Siegal, and L. Staiano-Coico. 1996. Apoptotic depletion of CD4+ T cells in idiopathic CD4+ T lymphocytopenia. J Clin Invest. 97(3):672-80.
Tassinari, P., L. Deibis, N. Bianco, and G. Echeverria de Perez. 1996. Lymphocyte subset diversity in idiopathic CD4+ T lymphocytopenia. Clin Diagn Lab Immunol. 3(5):611-3.
Garry, R. F., C. D. Fermin, P. F. Kohler, M. L. Markert, and H. Luo. 1996. Antibodies against retroviral proteins and nuclear antigens in a subset of idiopathic CD4+ T lymphocytopenia patients. AIDS Res Hum Retroviruses. 12(10):931-40.
Fernandez-Cruz, E., J. M. Zabay, and M. A. Munoz-Fernandez. 1996. Idiopathic CD4+ T-lymphocytopenia in an asymptomatic HIV-seronegative woman after exposure to HIV [letter]. N Engl J Med. 334(18):1202-3.
Bordin, G., M. Ballare, S. Paglino, P. Ravanini, D. Dulio, M. C. Malosso, R. Boldorini, and A. Monteverde. 1996. Idiopathic CD4+ lymphocytopenia and systemic vasculitis. J Intern Med. 240(1):37-41.
Belmin, J., M. N. Ortega, A. Bruhat, A. Mercadier, and P. Valensi. 1996. CD4 lymphopenia in elderly patients [letter; comment] [see comments]. Lancet. 347(9005):911-2; discussion 912.
1997
Yinnon, A. M., B. Rudensky, E. Sagi, G. Breuer, C. Brautbar, I. Polacheck, and J. Halevy. 1997. Invasive cryptococcosis in a family with epidermodysplasia verruciformis and idiopathic CD4 cell depletion. Clin Infect Dis. 25(5):1252-3.
Torikai, K. 1997. Idiopathic CD4+ T-lymphocytopenia [editorial; comment]. Intern Med. 36(11):759.
Shimano, S., N. Murata, and J. Tsuchiya. 1997. [Idiopathic CD4+ T-lymphocytopenia terminating in Burkitt's lymphoma]. Rinsho Ketsueki. 38(7):599-603.
Pilheu, J. A., M. C. De Salvo, J. Gonzalez, D. Rey, M. C. Elias, and M. C. Ruppi. 1997. CD4+ T-lymphocytopenia in severe pulmonary tuberculosis without evidence of human immunodeficiency virus infection [see comments]. Int J Tuberc Lung Dis. 1(5):422-6.
Louis, E., M. P. Moutschen, P. De Marneffe, R. Malherbe, T. Closon, M. T'Jean, J. Demonty, and J. Belaiche. 1997. Extensive ulcerative colitis and extraintestinal manifestations in a patient with HIV infection and significant CD4 T-cell lymphopenia. Gastroenterol Clin Biol. 21(11):884-7.
Hayashi, T., Y. Hinoda, T. Takahashi, M. Adachi, S. Miura, T. Izumi, H. Kojima, S. Yano, and K. Imai. 1997. Idiopathic CD4+ T-lymphocytopenia with Bowen's disease [see comments]. Intern Med. 36(11):822-4.
Hardman, C. M., B. S. Baker, J. Lortan, J. Breuer, T. Surentheran, A. Powles, and L. Fry. 1997. Active psoriasis and profound CD4+ lymphocytopenia. Br J Dermatol. 136(6):930-2.
Hanamura, I., A. Wakita, S. Harada, K. Tsuboi, H. Komatsu, S. Banno, O. Iwaki, G. Takeuchi, M. Nitta, and R. Ueda. 1997. Idiopathic CD4+ T-lymphocytopenia in a non-Hodgkin's lymphoma patient. Intern Med. 36(9):643-6.
Galie, M., M. Cassone, C. Ausiello, and P. Serra. 1997. [Idiopathic CD4+ T-lymphocyte deficiency: the clinical evolution of a case (see comments)]. Ann Ital Med Int. 12(4):233-7.
Dammacco, F. 1997. [Idiopathic CD4+ lymphocytopenia: a clinico-immunological syndrome of uncertain significance (editorial; comment)]. Ann Ital Med Int. 12(4):197-8.
Coutant, G., J. P. Algayres, H. Bili, and J. P. Daly. 1997. [CD4 lymphocytopenia, Gougerot-Sjogren and systemic lupus erythematosus]. Ann Med Interne. 148(7):503-4.
Venzor, J., Q. Hua, R. B. Bressler, C. H. Miranda, and D. P. Huston. 1997. Behcet's-like syndrome associated with idiopathic CD4+ T- lymphocytopenia, opportunistic infections, and a large population of TCR alpha beta+ CD4- CD8- T cells. Am J Med Sci. 313(4):236-8.
Chikezie, P. U., and A. L. Greenberg. 1997. Idiopathic CD4+ T lymphocytopenia presenting as progressive multifocal leukoencephalopathy: case report. Clin Infect Dis. 24(3):526-7.
al-Attas, R. A., A. H. Rahi, and F. E. Ahmed el. 1997. Common variable immunodeficiency with CD4+ T lymphocytopenia and overproduction of soluble IL-2 receptor associated with Turner's syndrome and dorsal kyphoscoliosis. J Clin Pathol. 50(10):876-9.
1998
Tumbarello, M., E. Tacconelli, C. Colosimo, R. Cauda, and L. Ortona. 1998. Meningoencephalomyelitis caused by herpes simplex virus-1 in a patient with idiopathic T CD4+ lymphocytopenia. Neurology. 50(2):569-70.
Suzuki, Y., S. Suzuki, M. Numata, Y. Matsumoto, J. Suzuki, H. Ikeda, and T. Okubo. 1998. Acute respiratory failure due to miliary tuberculosis in a patient with idiopathic CD4+ T-lymphocytopaenia. Respir Med. 92(7):977-9.
Menon, B. S., I. L. Shuaib, M. Zamari, J. A. Haq, S. Aiyar, and L. M. Noh. 1998. Idiopathic CD4+ T-lymphocytopenia in a child with disseminated cryptococcosis. Ann Trop Paediatr. 18(1):45-8.
Ishida, T., T. Hashimoto, M. Arita, I. Ito, and M. Osawa. 1998. Pulmonary Mycobacterium avium disease in a young patient with idiopathic CD4+ T lymphocytopenia. Intern Med. 37(7):622-4.
Ho, C. L., B. C. Chang, G. C. Hsu, and C. P. Wu. 1998. Pulmonary cryptococcoma with CD4 lymphocytopenia and meningitis in an HIV-negative patient. Respir Med. 92(1):120-2.
Hayashi, T., M. Adachi, Y. Hinoda, and K. Imai. 1998. [Idiopathic CD4+ T-lymphocytopenia]. Ryoikibetsu Shokogun Shirizu. (21(Pt 2)):185-7.
Freier, S., E. Kerem, Z. Dranitzki, M. Schlesinger, R. Rabinowitz, C. Brautbar, M. Ashkirat, and Y. Naparstek. 1998. Hereditary CD4+ T lymphocytopenia. Arch Dis Child. 78(4):371-2.
Cook, M. A., D. Bareford, and D. S. Kumararatne. 1998. Non-Hodgkin's lymphoma: an unusual complication of idiopathic CD4+ lymphopenia. Hosp Med. 59(7):582.
Cascio, G., A. M. Massobrio, B. Cascio, and A. Anania. 1998. Undefined CD4 lymphocytopenia without clinical complications. A report of two cases. Panminerva Med. 40(1):69-71.
Cheers, and yes, "HIV" causes AIDS...And "HIV" causes AIDS...
andy
Kevin, your combination of profound ignorance and vacuous arrogance is far more insulting than your insults. You clearly do not even know how Diflucan has been studied and utilized in people with AIDS, yet here you are with your sneeringly expressed theories on it's curative potential (having done so well with your insistence on lots of Biaxin for your sinusitis). Go to PubMed and you'll see that fluconazole has been chronically administered to people with AIDS at dosages of up to 800mg/day. Works very well as a treatment for cryptococcal meningitis and several other fungal infections; does not cure AIDS.
I'll leave you to your theorizing now, have a great life and remember to watch out for C. glabrata.
Good call, Adele. Found some of Cooler's copypasta on a 911 conspiracy theory website. Looks like his quote from Lo is cobbled together from a couple different sources.
Cooler, could you add some punctuation and capitalization to your comments? Thanks.
As to Cooler's quote from Shyh-Ching Lo, the paragraph starting with "There is no good explanation..." is from a 1990 Miami Herald article.
"In the spirit of "the openness" of science and We believe the most healthy and responsible are from a letter written in response to an article by Duesberg and Ellison in Policy Review (Dec 1990) reprinted on Duesberg's self promotion site.
Interestingly, there are a few intervening paragraphs that cooler left out.
Here they are
Of course, as Kevin will attest, one's views can change over the matter of a few years, so 17 year stale quotes isn't exactly indicative of Lo's current beliefs. It doesn't help that the quotes are cherry picked and pasted together without noting that they were from separate sources.
(6) Extensive evidence from electron-microscope examinations, from specially designed PCR tests to look for the DNA of Mycoplasma incognitus, and from immunologic tests, showed that the organism was concentrated in lesions in affected organs. Mycoplasma incognitus is unusual in that it often infects and kills tissue without causing an inflammatory reaction, suggesting that it disables or evades part of the immune system....
From lo's paper "One VLIA inoculated animal had a prominent antibody response, which occurred 7 months after VLIA inoculation. The other 3 monkeys had a transient or poor antibody response in the later stages. These 3 animals revealed periodic VLIA antigenemia during the course of the experiment. A control monkey was killed 8 months after the last VLIA inoculated monkey succumbed and showed neither an antibody response nor evidence of antigenemia"
guess what what little antibodies they show comes late only when they are near death, antigenemia was only sporadic, and antibodies non existant at the beggining/middle of illness.
Clearly the PCR is far more reliable to detect this microbe
Kevin, one doesn't need to be a "reading superhero" to notice that your Mayo clinic authors find fungus growing in samples from 100% of healthy individuals. They found no statistical difference between the total number of fungus varieties growing in sick and healthy people.
What if HIV was found in everyone? You would jump on that right away and you would have a point. If everyone has it, why don't most people get AIDS? But in fact very few people have HIV and most of them develop AIDS in the end if they're not treated with the right drugs.
But everybody has fungus growing in their noses and only 1-4% of people have chronic sinus problems. That doesn't mean antifungals couldn't ever help with them in some cases. But it's not the fungus, it's the body's response to it. That's all there is to say.
Cooler, from your own quote,
"These 3 animals revealed periodic VLIA antigenemia during the course of the experiment." That means they showed antibody sporadically throughout.
But whatever, yes PCR is almost always more sensitive than antibody-based methods. That's why HIV denialists hate it so much and try to say Kary Mullis says it's not valid as if that matters. PCR detects mycoplasma and HIV better than most or all techniques out there.
Well id be glad to post the entire post from Duesberg site and from the Miami Herald article. It would take up too much space, thats why I copied and pasted, none the less it wouldnt be so good for your cause, because the father of hiv Luc montagnier talks about how many flaws that are in the hiv hypothesis in the 1990 Miami Herald article.
http://www.virusmyth.net/aids/data/ebhiv.htm
I will try to use good punctuation from now on, but I'd rather make a few grammatical errors than support pumping kids with mercury far beyond the EPA's safe limit like you sanctimonious establishment sycophants do. If the CDC said it was healthy to drink gasoline you guys would probably support it. LOL
Andrew's latest is more unattributed copypasta from here. The last update was in 2001.
Andrew doesn't mention that he swapped out the following paragraph for his own diatribe against "deluded" doctors. The delusion? Not agreeing with the denialists (while childishly calling Fauci a denialist).
Andrew also leaves out the abstracts listed with some of the citations. I can only guess that it was to offer us some mercy from his long comments. Another mystery is why he didn't link directly to the page. Is he quoting his own writing? His own list?
I will try to use good punctuation from now on, but I'd rather make a few grammatical errors than support pumping kids with mercury far beyond the EPA's safe limit like you sanctimonious establishment sycophants do.
False dichotomy, ad hominem, and mercury militia silliness thrown in to boot.
The Montagnier (argument from authority) stuff is 17 years old, too. What does he think now?
Robster, if ya wanna read up on ALU sequences or "alu-mediated recombinations," I refer you to our work...
Also we really should discuss the basics of genetics sometime, especially as it might/might not relate to mutation and resistance.
The argument would begin, well -like gives rise to like, otherwise it doesn't work too good (H.J. Mueller, who discovered that x-rays cause mutations had a lot to say, as do some of us in the cancer community regarding the mechanisms of tumor resistance. Microbial resistance is mediated by biofilms. Tumors have biofilms. No mutations necessary.
Maniotis AJ, Valyi-Nagy K, Karavitis J, Moses J, Boddipali V, Wang Y, Nuñez R, Setty S, Arbieva Z, Bissell MJ, and Folberg R: Chromatin organization measured by Alu I restriction enzyme changes with malignancy and is regulated by the extracellular matrix and the cytoskeleton. Am J Pathol 166: No. 4 April 2005.
Folberg R, Arbieva Z, Moses J, Hayee A, Sandal T, Kadkol S, Lin AY, Valyi-Nagy K, Setty S, Leach L, Chevez-Barrios P, Larsen P, Majumdar D, Pe'er J, Maniotis AJ.
Tumor cell plasticity in uveal melanoma: microenvironment directed dampening of the invasive and metastatic genotype and phenotype accompanies the generation of vasculogenic mimicry patterns. Am J Pathol. Oct;169(4):1376-89, 2006.
Tone Sandal, Klara Valyi-Nagy, Robert Folberg, Mina Bissell, Virginia Spensor, Andrew Maniotis. Epigenetic reversion of breast carcinoma phenotype and DNA sequestration. May, Vol 170 No. 5, American Journal Of Pathology, 2007.
Klara Valyi-Nagy, Robert Folberg, Tibor Valyi-Nagy, Andrew J. Maniotis. Susceptibility of Herpes simplex Virus Type I and II, The Role of Tumor Invasiveness, The Extracellular Matrix, and Chromatin Sequestration. In press. Experimental Eye Research, 84, pps. 991-1000, 2007.
Gary Stein. Commentary: Mechanogenomic control of DNA exposure and sequestration. American Journal of Pathology,
Vol 166 No. 4, April 2005. (This is a decent review of the concepts.)
Can you offer any kind of explanation for your blatantly false statements about the correlations between CD4 T cells and total lymphocyte count, Dr. Maniotis?
Do you think correlation coefficients of 0.08 - 0.19 (from the Paediatric Prognostic Markers Collaboration Lancet paper) indicate a strong correlation?
How about informed consent.
Look we are all not going to change eachothers mind, so its pretty pointless to endlessly argue.
Considering patients and Americans pay for the reasearch and juries in criminal trials (which involve a lot of science) usually get the verdict right, while experts in criminal trials (because of conflicts of interest) usually get it wrong I propose this.
Every American Adult should hear every side of an important health issue. For example every American should hear the best arguments from both sides on the mycoplasma/cfs/aids link the hiv debate and the mercury debate. Once they hear all sides they can decide for themselves what makes sense, and what doesnt.
I find it strange that we are only exposed to one side of these important arguments concerning hiv/mercury etc, and the reason given is.....You cant hear another side of an argument because you might believe it!
Can you Imagine if you were a juror and a prosecutor or defense attorney said something like that, you would demand to hear all opposing viewpoints to get to the truth. Unfortunately that does not happen in America, and it should, and people are dying because of it.
Andrew,
Just how low will you stoop with your distortions and lies. Twice (on this thread) you've posted the following:
The "quote" you attribute to Laurent-Crawford et al. does not appear in their paper. Apparently you (or perhaps one of your sock puppets) made it up so that you could pretend that they said it!
Here's the closest approximation that I can find in Laurent-Crawford's paper (from the abstract on page 829):
There is no possibility that this is merely a misinterpretation of a complex idea by an intellectually lazy blowhard. This can only be a bald-faced lie. Are you really so intellectually bankrupt that you have to "manufacture quotes" that distort the scientific work of others in order to promote your failed scientific ideas?
Please tell us where that quote comes from--it's certainly not from the source you cite.
Cooler,
I am a firm believer in free speech. I think people should be free to speak their minds. But if individuals use lies and distortions rather than honest arguments based on sound logic, they shouldn't scream censorship when mainstream society ignores them. And when they use their lies and distortions to attempt to influence important personal, financial, or medical decisions of others, they should expect to be harshly criticized.
When you argue that every American should be able to hear every side of an important health issue and decide for themselves, I agree. But we've just seen how Andrew Maniotis, a professor at a major American university posted a made-up quote from Laurent-Crawford et al. (1991) in support of the mycoplasma hypothesis. What fraction of Americans do you think is sophisticated enough to be able to track down an article from the journal Virology, read it, understand it, and realize that this University professor is basically making up lies?
How do you explain or excuse Maniotis making up a quote from a scientific paper? For God's sake, he has a PhD from Berkeley--and he's making up scientific quotes to try and convince AIDS patients to stop taking their medicine!
He can only consider behaving in this way because he realizes that, in a forum such as this one, most of the readers are not sophisticated enough in the necessary scientific disciplines to be able check up on his accuracy. In the top peer-reviewed scientific journals he could never get away with a stunt like that. But how is the average adult American, untrained in science, supposed to tell apart people like Maniotis from honest scientists?
What do you think is the proper role of scientists, health care professionals, and legislators in response to this kind of behavior? Do you think we have a responsibility to protect the general public from articulate and apparently respectable spokespeople who spout impressive-sounding, technically sophisticated lies in support of a position that will cost other people money or risk their health? How do you think we can balance this responsibility with the need to promote free speech?
EJ's parents listened to snake oil salesmen like Maniotis, and now EJ is dead without ever having the chance to benefit from all of the great science that our tax dollars has paid for.
This is very important for all new readers who are learning for the first time about the BIG LIE called HIV causes AIDS. Yes, there is HIV, and, yes there is AIDS, however, contrary to the 1984 NIH press conference at which Heckler and Gallo proclaimed HIV to be the cause of AIDS, this is the BIG LIE, HIV is NOT the cause. Notice how franklin is a perfect example of a typical believer in the BIG LIE, HIV causes AIDS.
franklin must distort the facts to fit this belief which has no rational basis in science. How do we know that HIV causes AIDS? Because a government web site proclaims that all scientists believe it to be so. Notice how franklin would rather believe a phoney newspaper story that falsely says Ariel never received AZT, and therefore died of AIDS. This is a LIE. The entire HIV causes AIDS institution is riddled with such LIES.
franklin said: The answer is that she (Ariel) died of AIDS. She did not die from intravenous AZT. Had you read the information hyperlinked to Ariel's name, you would have learned that Ariel died before any anti-retroviral drugs were available for children. Her parents tried desperately to obtain AZT for Ariel, but they were unsuccessful. Ariel never received AZT. Her death could not have been due to AZT or any other anti-retroviral therapy--because she received none. Read about Ariel and about the parents of other HIV-infected children who were forced to helplessly watch their dying children become blind and demented and still could not get approval to have their children treated with AZT in this NY Times article from 1989. Once again you prove that AIDS denialists have no regard for the facts. You are committed only to advancing a point of view and will simply ignore any and all evidence to the contrary. Ariel's tragic death was pretty much run-of-the-mill for pediatric AIDS cases back in the 1980's. Nowadays, deaths like Ariel's can largely be prevented. Unfortunately for EJ, her parents chose to ignore the lesson of Ariel Glaser.
Dear franklin,
Previously I stated the death of Ariel Glaser at the age of 7 in 1988 occurred after she was given oral and I.V. AZT. Michael Glaser's web site states that Ariel Glaser received both oral AZT tablets and INTRAVENOUS AZT. As we all know by now, AZT is a deadly toxic poison which kills those who take it. Ariel was killed by AZT. Her mother Elizabeth died Dec 1984 after taking AZT.
It is all clearly stated on:
http://www.paulmichaelglaser.org/elizabeth.html
Both Elizabeth and Michael Glaser were betrayed by their doctors, the media, and the NIH. They were convinced that they should give daughter a toxic poison, AZT.
Elizabeth later died from AZT toxicity after writing her book entitled, "Absense of Angels". Their son Jake age 22 is HIV positive and alive and well. Jake's life is an example of the truth of the statement, HIV is not a death sentence, if one avoids deadly drugs.
Ariel was born in 1981, and was well until 1986 (age 5) when she had an "undiagnosed illness", and an HIV test was found to be positive. Ariel received AZT in Dec 1986. By January 1987, Ariel could not walk or talk, clearly toxic from the AZT. In March, Ariel had pneumonia and cerebral atrophy, both from AZT toxicity. A doctor whose name is mentioned on the web site and in the NY times article you cited, gave Ariel AZT intravenously, May 1988. By July, the IV AZT was discontinued because of a low white cell count. Ariel died August 12, 1988 after receiving AZT for 20 months (Dec 86 to Aug 88). Ariel's parents were betrayed by the BIG LIE, and unwittingly sacrificed their child. The truth of this tragedy is so hideous, the BIG LIE must be continued. Not any more. Taxpayers are getting fed up with paying though the nose to fund a BIG LIE. Its time to turn off the money.
By the way, franklin is an arrogant and pompous fool.
For more true information about the science blunder called HIV/AIDS, see:
www.reviewingaids DOT com
www.livingwithouthivdrugs DOT com
If its true that he did that, than the way to combat it is with more free speech.It worked here for you. For example if this happened in a court, you could point it out and the judge/jury would rule.
What is much more dangerous is only hearing one side of an argument. Im agnostic on hiv, but I was sick with CFS for many years. I Know there is another microbe out there, and I stumbled upon research from DR. shyh Ching Lo and Garth Nicolson. Lo's mycoplasma folfilled Kochs postulates (LO had an animal model, see my posts above) much more than hpv, hep c or even hiv did in the early days. They didnt have big pharma backing and the public was not made aware of his solid reasearch and how this bug was being found via PCR in CFS patients and other chronic illnesses.
I suddenly became ill and was in limbo for many years. I cant imagine people suffering with this infection when they could be cured. An open debate on hiv, mercury and mycoplasma is what the public deserves. Those who forge documents will be found out and combatted with more free speech.
What about the HIV establishment?
Do they ever inform people that AZT was an old chemotherapy drug designed to kill dividing cells?
Do they tell people that hiv only infects a small fraction of T cells?
That most chimpanzees dont get aids?
That some experts feel the case is not closed?
What about vaccines, most patients dont even know that they are taking in 50 times the EPA daily safe limit of mercury...........this is wrong.
Hear all the arguments, then the people will decide whats psuedoscience and whats not. Forged documents will uncovered and addressed by the adversaries engaged in the debate.
Andrew,
Unless you are the original author of the piece at chronicillnet (correct link here), you presented that work as your own, while taking out the paragraph delineating acquired and induced immunodeficiencies (where the unnamed author suggests ICL should be placed). If that page is another's work then you have intentionally misrepresented and plagiarized another's work in one move.
ICL and AIDS differ in two key respects. ICL, to this point, does not appear to be transmissible and ICL does not progress in the manner of AIDS. Some ICL cases resolve with treatment, which is sadly not the case for AIDS patients. ICL is also exceptionally rare.
Does anyone have prevalence data on it? I found a 1993 number of 47 cases in the US.
------------------
Cooler,
Every American Adult should hear every side of an important health issue.
Even the ones that have no compelling evidence, such as HIV/AIDS denialism, mercury militia, antivaxers, germ theory denialism, Christian Scientists, etc? Informed consent? Misinformed consent, perhaps.
The equal time argument is compelling at first glance, but that isn't how science works. If science worked this way, we would still be debating whether or not the world is flat. Not that there aren't flat earthers still out there... However, it is the preferred argument of creationists and inteligunt desine proponents. The reality is that the public debate has already occurred in the scientific journals. Calls for debate only come from those who have already lost.
You cant hear another side of an argument because you might believe it!
If the other side is based upon long abandoned hypotheses, spurious correlations, lies and distortions, then evidence based medicine should always win out. When said lies are intended to convince AIDS patients to go off their prescriptions (leading to more OIs and a greatly shortened lives) or discourage individuals from practicing safe sex (increasing the prevalence of a wide variety of STIs including HIV), it is incredibly unethical to do so.
Its up to the people to distinguish between psuedosceince and a good theory, not a group of scientists that are bought and paid for by drug companies.
People dont believe psuedoscience, no one would beleive that the moon is made of cheese just because a few people said so. A jury of americans with no conflicts of interests works in our criminal justice system, and we are the ones that will decide what theory's have credence, we don't need Nurse Ratched telling us what we can and can't hear.
How many times have the majority of "experts" been wrong and scientific minorities and average laypeople right. Between Vioxx, selenimite, heliobacteria etc it never ends. The whole process is dominated by big money and good scientists with no conflicts of interest get igonored in favor of big drug companies.
A jury? A trial? Australia just had one and called the HIV/AIDS denialists lacking in credibility and evidence.
If we let the public decide science when so many believe such silly things, evolution would not be real, astrology would be front page news and depending on what state you live in, Jesus visited the Native Americans.
Luckily, science doesn't work that way. Good research wins through because of its convincing nature, i.e. H. pylori and stomach cancer, with drugs produced by big bad pharma used to treat H. pylori before it can cause problems. Seriously, the Galileo gambit isn't a valid form of argument. For every Galileo, there are is a basket case of nuts.
Actually, the history of AIDS research follows an interesting pattern. The behavior/ drug abuse hypothesis appeared good for a bit, but had some ugly holes. The discovery of HIV and subsequent research tying it to AIDS, filled those holes. Do we know everything about HIV and AIDS? No. But that is what continuing research is for.
This is quite possibly the most phenomenally idiotic statement I've ever heard in my life.
We don't put science up for a popular vote because most people are incapable of assimilating all the necessary background to competently judge it. If that offends your flagrant anti-intellectual sensibilities, tough shit.
Tyler totally tells it like it is!
Cooler or Gene or Andy or somebody said
People dont believe psuedoscience, no one would beleive that the moon is made of cheese just because a few people said so.
Really? I just have to look at BillyBipBip's 9-11 websites to see that's not true. People believe stuff every day with no basis at all in reality. Most people will believe whatever fits into their system of prejudices. A hundred years ago most people in this country and Europe believed one ethnic group was really smart and greedy and evil. Even though most people never knew anyone from this group. They also believed another race of people was morally and intellectually inferior and was meant to serve other races. Get this, there are still millions of people who think this way including 911 conspiracy theorists who think "Jews" did it! So in Frummy's equal time we should teach this kind of drivel alongside programs on diversity, tolerance and equality.
Most people in the United States believe a deity created the world 6000 years ago. So according to Frummy teachers should spend just as much time teaching Genesis as evolution. But why stop at that? Divide the section into three and teach Panspermia too. And its not like monotheism is the only thing around so lets give equal time to all religions ideas of how the world exists like the old turtle with the world on its back.
Most people are confused about the Earth going around the Sun or the Sun going around the Earth. So we should fund Earth-centric astronomers in equal numbers with normal astronomers.
It's amazing Cooler says censorship at the same time as promoting 911 conspiracy and HIV denialism vaccination woo and big pharma tinfoil hat nonsense on the internet. Tell me, Cooler, how many of your posts has Tara deleted?
Dear Mr. Jeffreys,
RE:
"Can you offer any kind of explanation for your blatantly false statements about the correlations between CD4 T cells and total lymphocyte count, Dr. Maniotis?"
"Do you think correlation coefficients of 0.08 - 0.19 (from the Paediatric Prognostic Markers Collaboration Lancet paper) indicate a strong correlation?"
To address the issue of why absolute lymphocytes versus CD4/CD8 ratios weren't measured before the coroners were made aware of Christine Maggiore's (inconsistent) "HIV-positive status," and before the coroners changed their initial "indeterminate" cause of death, and deemed Eliza Jane an "AIDS statistic," it is clear that there was no reason for anyone to assume that in Eliza Jane's case, they were dealing with an immune suppressed individual. Her acute symptoms during her 36-hour death appeared to be due to a hyper-immune reaction to a prescribed drug. However, despite the coroner's failure to provide an "HIV" test (ELISA, WB, or PCR) or CD4+/CD8+ ratio in support of their "AIDS diagnosis," it should be emphasized that the accuracy of total lymphocyte counts in predicting death due to "AIDS-associated indicator diseases" is considered (BY THE AIDS ESTABLISHMENT) equal or even superior to measuring the CD4/CD8 ratio. I QUOTED THE PAPER ITSELF DIRECTLY (SEE BELOW).
Therefore, and despite the fact that CD4/CD8 ratios were NOT obtained (by those attributing her death to AIDS after the revised autopsy report was filed some 4 months after the death), absolute lymphocyte numbers were obtained at the hospital, and according to "AIDS experts," (AND THE LANCET ARTICLE REFERENCED BELOW) they are just as predictive of AIDS-related death in children, if not more so.
In a study of 3917 children, it was reported that:
"For children older than 2 years, the 12-month risk of death and AIDS increased sharply at values less than 1500-2000 cells per microliter, with little trend at higher values." (Eliza Jane's count was 10,800 cells/microliter).
"Mortality risk was substantially higher at thresholds of total lymphocyte count recommended by WHO than at corresponding thresholds of CD4-cell percentage. When the markers were compared at the threshold values at which mortality risks were about equal, total lymphocyte count was as effective as CD4-cell percentage for identifying children before death..."
Dear Franklin,
I suggest you read the goddamn paper before throwing out accusations. Perhaps a little help...
Look on page 834 under the section entitled:
Accumulation of nucleosomes occur before maximal production of virus in HIV-infected cells.
"Recently it has been demonstrated that mycoplasmas can enhance the ability of HIV to induce a cytopathic effect in vitro (Montagnier et al., 1990; Lo et al., 1991). We therefore investigated the effect of an inhibitor, mycoplasma removal agent (MRA) on the HIV0-1 infection in CEM cells Under our experimental conditions, addition of MRA in HIV-infected cultures ROUTINELY RESULTED in SIGNIFICANT DELAY (3-4 DAYS) IN THE DEVELOPMENT OF SYNBCYTIA. Furthermore, the cytopathic effect was transient and fewer cells were killed although large quati9ties of infectious virus were produced."
Dear Robster,
First time in my life I've been accused of plagerism! Thank-you. The work I cited and wrote that little intro for was indeed the piece you link-in part. I believe at the time, however, I did a pub-med search on many of the articles myself, and they may be mixed up with the ones on that link you provided. No intentional plagerism, or misrepresentation, however. Just pointing out some rather severe AIDS denialism on the part of all those authors, Fauci, and others who go ahead and invent new diseases when symptoms of their other disease(s) (AIDS) don't pan out consistently. ICL is AIDS without any "HIV" in it, as I said. It also represents, much like in the case of polio, a disease category that is indistinguishable from AIDS, or that in Africa for example, in the absence of any test kits, would be treated as AIDS with those life-saving meds like nevirapine, especially after Tremont changed the toxicity data.
But you guys are getting too upset, however. Try to calm down and quit saying nasty things like bald-faced liar, plagerist, etc. It doesn't become you. Also it might help if your read your own literature once in awhile.
Thanks,
andy
...and now EJ is dead without ever having the chance to benefit from all of the great science that our tax dollars has paid for. -- Franklin
Bootlicker, alert! Your blind faith in the sanctity of modern science smacks of a religiosity that is obsequious and downright dangerous.
Seriously, Franklin, you are more than a bit naive. Perhaps, you and Robster should form a study group, too. Consider the following quote from Overdosed America (Adele's fav new book):
Ultimately, the issue is not the quality of our medical science, but the political context in which American medicine unfolds. The overwhelming power that the drug and other medical industries now wield over American politics, science, and health care has created an imbalance between corporate goals and public interest that is not longer self-correcting.
You, Franklin, like Robster, Richard Jefferys, DT, Dale and numerous others on this blog turn a blind eye to the obvious fact that modern medicine and the scientific research complex are no long self-correcting, as Dr. Abramson eloquently notes. So, you are the real denialist and you are the real danger to public health.
Just like with so many other institutions in our society, this loss of the self-correcting mechanism is incredibly important to understanding how major blunders, like HIV/AIDS, can and do occur. For an equally illuminating example, one has to look no further than the currently imploding housing market, which also radically abandoned the inherent self-correcting elements, that had previously protected public interests from destructive, but personally lucrative, practices such as predatory lending, appraisal fraud, and poor-quality construction -- all of which have combined to make this bubble, unprecedented in scale.
Greed and corporate interests have been trumping more important human concerns for some time now and if lackeys, such as yourself, Franklin, do not wake up soon, the fallout will be exponentially worse.
Kevin
Tyler,
You people can not even answer the simplest questions about hiv, so please don't imply that I'm not making any sense.
What's the first scientific paper that proved hiv caused Aids?
How does hiv cause organ failure if its only present in a small number of T cells? (see Lo's pathology studies above)
Im not saying HIV has nothing to do with AIDS, I agree with DR. LO's statement in 1990, that "AIDS is much more complicated than Hiv" I think his mycoplasma hypothesis (that folfilled Kochs postulates much more than Hep c, hpv for example) deserves to be heard by the American People with CFS and other mysterious illnesses.
Am I a holocaust denier because I feel that way? I don't know all the answers, but I don't claim to, and realize an open debate between scientists/activists with public scrutiny is the best way to deal with health issues.
As far as people are so stupid they will easily beileve in psuedoscience your examples of Hitlers Germany actually prove my point. Hitlers Germany was able to advance psuedoscience because they were only allowed to hear one view, and barred from hearing another. You hiv fundamentlists dont seem to understand that, and you are doing the same thing now.
People are not stupid, infact during a criminal trial its you experts that spread lies and psuedoscience and we average people that get it right.
Thats why you people are so petrified of taking this debate public. If a group of scientists argued that eating 20 pizzas a day was good for you no one would beleive that, the only way people would believe something like that is if you never let them hear another side of the story (Fat is bad for you), which is what you people do.
The more paranoid you are about "denialism" just shows how insecure you people are. A good prosecutor would not care if a defense attorney advanced a crazy argument, it would actually help them. A Corrupt prosecutor with a bad case would do exactly what you guys are doing, preventing, at all costs, the public from hearing another side of an issue.
I watch Andrew squirm and lie and I know why. If EJ died of AIDS when her mother was a rich white woman and no one had any antivirals denialism is cooked.
But if EJ died of antibiotic poisoning or "fifth disease" it's very sad and we all wish she hadn't but it doesn't change anything about HIV causing AIDS. Unfortunately tens of thousands of kids have died of AIDS most of them because they didn't get antivirals.
Andrew complains he's accused of "plagerism" when Robster actually said if Andy wasn't the author of that piece on chronicillnet he's plagiarizing. If Andrew is the author then he's not plagiarizing just misleading and being a crappy writer and a disgrace to his university. So maybe Andrew is the one who should calm down.
The Lancet paper Andrew clings to like a lifepreserver as usual proves him wrong when you read it. Actually the title by itself of the commentary "Total lymphocyte counts and ART in resource-limited settings" This paper measures kids in the USA but it isn't about LA and rich parents who know their seropositive and don't care because it gets them some fame and money to deny it. It's finally about places where doctors have to make hard choices about who gets drugs and who doesn't and where there aren't FACS machines in every lab.
The paper says low TLC can predict AIDS or death in HIV kids. It DOESN'T say high TLC ABSOLUTELY GUARANTEES that a 3 year old can't possibly die of AIDS. That's Andrew's logical f-up and it looks kind of dumb in someone who's a professor supposedly.
The sentence he quotes is about five year olds. Of course Andrew ignores this one "In younger children, total lymphocyte count was a less powerful predictor of death and, at an equivalent total lymphocyte count, they had higher mortality rates than older children."
So TLC can be a good test in resource poor settings and its even kind of predictive at low values. But like the paper says at high values it's not predictive and in young kids like EJ its not predictive. Also in this paper all the patients are identified and getting some kind of care. Unlike EJ who was being seen by some would say a quack hand-picked by mom to ignore the HIV elephant in the room, the failure to thrive recurrent infections etc.
And again Andy embarasses himself using someone's fictional memoirs as evidence, there's the "Christine Maggiore's (inconsistent)" test results. We have her word about these results. More likely she didn't understand what was going on or embellished later. She also said EJ was perfectly healthy but even the low quality of doctors seeing her wrote down things contradicting that. She said EJ didn't have pneumonia but the hospital said she did. I don't think I really trust this woman to tell me about her test results since they're at the bottom of everything.
Out of everyone on the thread, there's no bigger shill than Andrew Maniotis, Board Member. No one ready to accept whatever terrible quality evidence to keep his worldview together. And he's stooping, my god is he ever stooping! It's sad to see.
Franklin,
RE:
"How do you explain or excuse Maniotis making up a quote from a scientific paper? For God's sake, he has a PhD from Berkeley--and he's making up scientific quotes to try and convince AIDS patients to stop taking their medicine!"
I hope you found the quote on page 384 as I posted above. I forgot to also include from the Discussion, second paragraph, on page 837: "Inhibition of mycoplasma growth during an accute infection (figure 7), resulted in modified kinetics of infection in which maximal nucleosomal accumulation coincided with maximal syncytia formation and occurred several days before maximal production of HIV proteins."
(In other words, and Eleni got this right, effect precedes cause in this experiment).
I guess that's not too strange in "HIV/AIDS" science. People die of either too many or too few lymphocytes. They don't need to have a positive "HIV" test to be considered an AIDS or ICL patient, nutralizing antibodies are an indication of impending death, serodiscordant studies show no transmission, 68% of "HIV-positive" infants naturally serorevert by 18 months (of course if they aren't given toxic anti-retrovirals), 30 vaccine trials have failed to show a single case of humoral, cellular, or mucosal immunity, etc. etc. etc.
"He can only consider behaving in this way because he realizes that, in a forum such as this one, most of the readers are not sophisticated enough in the necessary scientific disciplines to be able check up on his accuracy. In the top peer-reviewed scientific journals he could never get away with a stunt like that. But how is the average adult American, untrained in science, supposed to tell apart people like Maniotis from honest scientists?"
On the contrary-I have tried to respond with respect even to people who considered me irrational because of where I sent proceeds from my father's funeral. I have provided references for every statement I have made. I have even referenced my own work (which you really ought to read before you start making statements about ALU sites), etc. Everybody has some value, Franklin, even me.
RE:
"EJ's parents listened to snake oil salesmen like Maniotis, and now EJ is dead without ever having the chance to benefit from all of the great science that our tax dollars has paid for."
I ain't no snake oil salesman. In fact, I have learned more from Christine than I'm sure she has ever learned from me. You oughta try reading her book. You might actually learn something about the science, and politics of "HIV/AIDS." Hers (and her family's experience) is an example of how the human spirit can even survive the Nazi-like human experimentation, and groundless tacit assumptions that have come to characterize the AIDS era.
I'm sure next time you visit your doc for your yearly flu shot, you won't balk when he or she tells you that he is going to do an "HIV" test as part of the routine. You won't even get any counciling, or warning either. I just hope, for your sake (and your family's sake and your insurance sake and your job sake), you aren't one of the 2% that will test false positive after any flu vaccine, as Klausner recently communicated and emphasized.
Andrew Maniotis wrote:
it should be emphasized that the accuracy of total lymphocyte counts in predicting death due to "AIDS-associated indicator diseases" is considered (BY THE AIDS ESTABLISHMENT) equal or even superior to measuring the CD4/CD8 ratio. I QUOTED THE PAPER ITSELF DIRECTLY (SEE BELOW).
The paper makes no mention of the CD4/CD8 ratio (the word "ratio" isn't even anywhere in it). I don't know where you get "or even superior" from since that claim is made nowhere in the paper, nor in any of the other published literature on the subject which you falsely claimed showed "similar if not identical trends" for CD4 and ALC (I note that you have not attempted to explain or defend that claim).
I'm also not sure how you define "the AIDS establishment" but I've not read any such claim about the equivalence or superiority of TLC by anyone. Given that TLC correlates better with CD8 counts than CD4 counts, it's not at all surprising that this is the case. More importantly, the Lancet paper is about using TLC as a substitute for CD4% when making decisions about initiating antiretroviral therapy, not as diagnostic criteria for active PCP in a child admitted to the PICU. Why don't you talk to a pediatric immunologist? I emailed longtime pediatric clinician James Oleske and he was absolutely unequivocal in stating that you can't rule out PCP simply based on ALC.
Therefore, and despite the fact that CD4/CD8 ratios were NOT obtained (by those attributing her death to AIDS after the revised autopsy report was filed some 4 months after the death), absolute lymphocyte numbers were obtained at the hospital, and according to "AIDS experts," (AND THE LANCET ARTICLE REFERENCED BELOW) they are just as predictive of AIDS-related death in children, if not more so.
Can you cite an "AIDS expert" saying TLC is just as predictive, if not more so? The Lancet paper does not make this claim, the most optimistic take it offers is that the TLC was "only marginally less predictive."
In a study of 3917 children, it was reported that:
"For children older than 2 years, the 12-month risk of death and AIDS increased sharply at values less than 1500-2000 cells per microliter, with little trend at higher values." (Eliza Jane's count was 10,800 cells/microliter).
But there is not zero risk at the higher values, there is just little trend for a difference in risk across the higher "selected values" (3,000, 4,000 & 6,000). The 12 month risk in a child with a TLC of 6000 was between 0.4 and 20%, depending on the age bracket. Perhaps it's also worth including the rest of this paragraph that you are quoting:
"For example, the estimated 12-month risk of death for a 5-year old child increases from approximately 1% for TLC >3,000 cells/mm3 to 2.4% at 2,000 cells/mm3, 5.3% at 1,500 cells/mm3, and 14% at 1,000 cells/mm3 (Figure 2A). In younger children, TLC is a less powerful predictor of death and, at an equivalent value of TLC, they experience higher mortality rates than older counterparts. These patterns are mirrored in the risk of progression to AIDS (Figure 2B), although incidence is typically three- to five-fold higher for the same values of age and TLC."
"Mortality risk was substantially higher at thresholds of total lymphocyte count recommended by WHO than at corresponding thresholds of CD4-cell percentage. When the markers were compared at the threshold values at which mortality risks were about equal, total lymphocyte count was as effective as CD4-cell percentage for identifying children before death..."
This is not a direct comparison of the predictive power of CD4% and TLC (the direct comparison showed that the correlation coefficients were 0.08 - 0.19). It is a comparison of mortality risk at the thresholds for TLC and CD4% recommended by WHO for the initiation of antiretroviral therapy. Again, it is in no way claiming that there is zero risk at higher values.
So where does that leave you? Essentially playing with probabilities in an attempt to exonerate yourself from culpability. If you were genuinely interested in the relationship between ALC and immune deficiency children, you're in a position where you could easily talk to someone with expertise on the subject. And the more relevant literature for the situation you're describing is the literature on ALC at PICU admission which is unfortunately very sparse, but what there is certainly does not support the claim you are attempting to make. It does, however, support what James Oleske told me, which I don't find that surprising given that he's been caring for children with HIV for more than two decades now.
As others have stated, this sudden interest in surrogate markers of immune deficiency in children when a routine CD4% or CD4/CD8 ration might have actually provided information on this child's risk of PCP while she was alive...I find it ghoulish and depressing.
andy writes 68% of "HIV-positive" infants naturally serorevert by 18 months (of course if they aren't given toxic anti-retrovirals)
Seropositive infants naturally serorevert as maternal antibodies are lost. Do you have any evidence that ARVs have any effect whatsoever on this process?
Didn't think so.
Andrew,
Did you write that piece? Apparently not. Did you tell us where it came from? No.
If you are not the original author, then intentionally or otherwise, you plagiarized. When caught, you puffed up your chest and denied it instead of saying it was a mistake. Classy.
Did you replace an original paragraph with your own diatribe, without noting that your unattributed quotation was separate from said quote? Yes.
Does your list sync up 100% with the list at the same site as the copied work? Almost exactly, yours differs by leaving out two papers, the heading for the year 1994, two [see comment] notes, but you include no citations outside of the original list, beginning in 1993 and ending in 1998. It is curious that your list is so similar to the original that goes with the quoted paragraph, but does not include any post 1998 articles. I suppose it is possible that your search turned up almost the same list, and you used the same format, including the year headings. It just wouldn't surprise me, considering your previous dishonesty about HIV/AIDS research.
testing
andy wrote I just hope, for your sake (and your family's sake and your insurance sake and your job sake), you aren't one of the 2% that will test false positive after any flu vaccine, as Klausner recently communicated and emphasized.
In fact, Klausner 'communicated and emphasized' An HIV nucleic acid amplification test was ordered to rule out cross-reactivity caused by the influenza vaccination; the patient's viral load was undetectable by this method. In accordance with accepted screening algorithms, we thus considered the patient to be HIV-negative with a high level of confidence.
So Andrew used his father's death to give money to Christine Maggiore and I mentioned it because it's in the obituary. That upset him. So he belittles me for being "naive" since I'm a tech not a professor. Fine. Doesn't bother me.
What I care about is, Andrew is proving he's a pathological liar who plays with public health to amuse himself.
Here he is talking about the influenza vaccine
I just hope, for your sake (and your family's sake and your insurance sake and your job sake), you aren't one of the 2% that will test false positive after any flu vaccine, as Klausner recently communicated and emphasized.
This is a total lie and Andrew knows it. Klausner didn't say anything like that. "Klausner" is Jeffrey Klausner, a San Francisco doctor who wrote a letter to the editor of the New England Journal of Medicine March 30 2006. Klausner describes a SINGLE
SINGLE
guy whose ELISA was reactive, Western indeterminate and PCR negative after a needle stick. Later he tested negative by all. He did have a flu vaccine but there's no proof it caused anything. I mean, who doesn't have a flu vaccine? That's why the antivaxx militia's got it so easy. Find a parent with a sick kid and guaranteed, that kid had a vaccine sometime, so blame it on that. Then they'll give your organization money or Alive and Well money or whatever. Especially if the kid dies, then you can get the gifts from the funeral. Repulsive.
Back to Andrew's lie. Klausner didn't say 2% test positive after any flu vaccine. He talked about one patient. Klausner cited a paper from 1995. Simonsen L et al American Journal of Epidemiology Vol. 141, No. 11: 1089-1096.
Here's the conclusion,
"The cluster of multiple false-positive donations in 1991 was most likely caused by the test kits used, rather than by the influenza vaccine."
The paper says in 1992 new kits were licensed for HIV and Hepatitis C and
""The new assays did not yield the false-positive results for the blood samples that gave false-positive readings" before that.
Let's summarize.
1. Nobody has proved flu vaccine or any other vaccine causes false positive on HIV.
2. People who did the work say it was test kits not flu vaccine causing the problem in a defined time 1990 to 92.
3. a couple organizations mention flu vaccine as a possible cause of false positive out of excessive precaution which is a good thing to have in medicine and to make sure people get retested if they need to be.
4. If flu vaccine increases your chance of testing HIV positive and there's really poor evidence it does Klausner's letter is very reassuring since his patient didn't test positive. Yes, the first assay was positive but that doesn't mean the conclusion was positive. ELISA + WB was indeterminate and with PCR he was negative.
I have provided references for every statement I have made.
Sure, he's provided fifty yards of screenful of references for every statment he made and they don't help him. They prove him wrong. The only problem is, some people will see all his references and think he's a kind of authority and believe him. And then another child will die or maybe an adult this time. Well, I suppose they can send the funeral proceeds to Alive and Well.
Robster wrote: Andrew, Did you write that piece? Apparently not. Did you tell us where it came from? No. If you are not the original author, then intentionally or otherwise, you plagiarized. When caught, you puffed up your chest and denied it instead of saying it was a mistake. Classy. Did you replace an original paragraph with your own diatribe, without noting that your unattributed quotation was separate from said quote? Yes. Does your list sync up 100% with the list at the same site as the copied work? Almost exactly, yours differs by leaving out two papers, the heading for the year 1994, two [see comment] notes, but you include no citations outside of the original list, beginning in 1993 and ending in 1998. It is curious that your list is so similar to the original that goes with the quoted paragraph, but does not include any post 1998 articles. I suppose it is possible that your search turned up almost the same list, and you used the same format, including the year headings. It just wouldn't surprise me, considering your previous dishonesty about HIV/AIDS research.
Robster is engaged in cheap tricks rather than any form of substantive debate. Accusing Andrew of plagiarism is a typical ploy for the AIDS apologists who have no answer for the serious questions, contradictions and inconsistencies of "AIDS" science raised by Andy. The link provided http://www.chronicillnet.org/reports/ci_report_4_ToC.html
does not contain any information which can be plagiarized, unless one considers a listing of medical literature abstracts to be plagiarism. Since it is common practice to quote from the medical literature by copying and pasting the abstract, this can hardly be called plagiarism. Robster should be ashamed of himself, and address the real issues raised by Andy and others here instead of engage in cheap tricks. For example, where is the medical research article which proves that HIV is the CAUSE of AIDS, and if it cannot be provided, then admit this fact. There has been complete stonewalling here from the AIDS apologists. Why is it that there are no pediatric AIDS studies of white suburban moms? Why is it all the pediatric AIDS studies are of inner city poor black drug addict moms? Why is it that Michael Glaser is HIV negative when HIV is "supposed" to be sexually transmitted? Why is it that Jake Glaser is Alive and Well after living 22 years with HIV? Why is it that pediatric AIDS children do not get Kaposi's Sarcoma, one of the very first AIDS defining diseases? Why is it that in African AIDS, the ratio of male:female equal while in North America it is predominantly a male drug user syndrome? Why is it that 0.4% of military recruits are HIV positive and never get sick. Why is it that there has been a steady 1 million HIV positives in the population of North American every year since 1984? And if these same HIV positives are spread evenly into the heterosexual population, where are the HIV positive white suburban babies from non-drug using moms? There aren't any.
Its time to stop the madness and turn off the public funding for a defunct hypothesis of iatragenocide called HIV/AIDS, which has been used to institutionally murder hundreds of thousands gays, impoverished drug addicts, and other minority groups deemed the undesirables of our society, with toxic drugs like AZT. Ariel Glaser was killed by 20 months of oral and Intravenous AZT toxicity. This is as plain as daylight. Ariel Glaser was, in fact, a sacrificial victim of AZT. The icon of the pre-eminent Elizabeth Glaser pediatric AIDS foundation is built on a LIE.
For more true information about the science blunder called HIV/AIDS, see:
www.reviewingaids DOT com
www.livingwithouthivdrugs DOT com
Forty,
If you don't give credit for a quote, it is plagiarism. I am giving Andrew the benefit of the doubt, suggesting that it was an honest mistake (even though it was for the dishonest intention of HIV/AIDS denialism). The reading list isn't a big deal, and pasting a paragraph from someone else in a web forum isn't that bad. More than anything, reprinting it was just embarrassing intellectual laziness and dishonesty (especially when he could have just linked to the page).
Quoting an abstract is typically done in a manner that tells who the first author is at the very least, so that you can find the full paper.
Andrew's constant misrepresentation and claims of inconsistencies have been addressed, even though he has ignored them. As to the location of the literature you request, many articles and resources have already been offered (and ignored), but a good place to start would be pubmed.
BTW, the late Elizabeth Glaser was a wealthy, white, non drug abusing mother, infected by blood transfusion for treatment of placenta previa while pregnant with Ariel (also exposing Ariel in utero and via breast milk). How is that for a case study?
No STI is 100% transmissible via sex, and I would bet that after finding out that she was HIV positive in 1985, after the birth of her kids, the Glasers practiced very safe sex, further reducing his chances of infection. In fact, from their page relating their story, it mentions that the surgeon general's statement that HIV isn't spread by kissing returned some "normalcy" to their lives. What they didn't know was that Michael carries the CCR5delta32 mutation, giving him some resistance to HIV.
Ariel passed away at age 7 (oddly some sources say she was 8, but I'll go with her parents on this one) in 1988, and AZT treatment for children was literally brand new. The oral treatment didn't help much, but an IV treatment greatly improved her condition for a while. Eventually, she had to stop treatment because of poor blood tests. About a month later, she died. Jake is alive because of the drugs that came to Ariel too late, and because he got his father's resistant CCR5 gene. As of 2006, he was off the drugs for five years, but is realistic that the infection may recur.
You fail again.
Andrew,
I can assure you that before I pointed out your misattribution of a quote to Laurent-Crawford et al. (1991), I read the paper very carefully. You might even say I read it "word-for-word". And following your instructions, I have re-read page 834, and I still cannot find the quote that you attributed to this article.
In fact, I can't even find it in the passage you extracted from the paper to provide "a little help".
Here's what you originally posted:
Now, here's your "helpful" extract from page 834:
I'm sorry, Andrew, there seems to be some confusion. Let me offer you a little help.
We are looking for the following sentence:
I do not find that sentence in here:
Nor do I find it anywhere else in Laurent-Crawford, et al. (1991) The Cytopathic Effect of HIV is Associated with Apoptosis. Virology 185:829-839.
At best, your made-up "quote" is a distortion of the data presented in the original scientific paper. Your "quote" uses the terms "apoptosis" and "cell death". The second passage uses neither of these terms but refers to "syncitia" and "cytopathic effect," very different scientific concepts.
Professor Maniotis, when one uses quotation marks, ie., these things: " ", one does so to signify a word-for-word transcript of something that what was previously said or written. The passage that you "quoted" from Laurent-Crawford et al. (1991), simply does not appear in that paper. You either made it up yourself or copied it from somewhere else--but you didn't find it in the paper by Laurent-Crawford et al.
That a member of a university faculty would engage in such an intellectually bankrupt pantomime of scientific reasoning is outrageous enough, but to then return with such a pathetically inadequate defense illustrates that you have abandoned all pretense of scientific integrity with respect to your deeply flawed views on the relationship between HIV and AIDS.
The flak is flying too fast for me to keep up with in this thread, but I thought I would just point out a couple of glaring mistakes (out of the several dozen) that Andrew Maniotis repeatedly makes. These both show he has no clinical or even laboratory understanding of HIV medicine.
First is his repeated confusion between "T cells" and "lymphocytes". In case you are wondering Andrew, not all dogs are poodles. If it is not ignorance on your part it is a deliberate ploy to misrepresent the truth, i.e. lying.
Second is your idea that patients who have HIV testing receive "councilling". No-one who has ever spoken with a patient about HIV or been involved with clinical medicine would be ignorant of the principles of counselling or not know how to spell this word.
Dear Forty Mules,
As you pointed out, the NYT article is misleading. According to the web page you directed us to, Ariel Glaser did receive AZT. Let's take the scientific approach and use the information you brought to our attention to re-evaluate your question:
The information you found makes it abundantly clear that she died of AIDS and not of AZT toxicity. And I guess you realize that because you misstate some key facts and omit others in order to argue your point. Did you learn the scientific method from Professor Maniotis at UIC?
You say that:
Unfortunately for your theory (and as stated clearly on the web page you directed us to), Ariel had been ill for long before she started on AZT in December 1987 (one year later than you claim).
None of the health problems she had prior to December 1987, can be blamed on AZT toxicity, because up to that point she had received no AZT.
Somehow you forgot to mention that Ariel's condition dramatically improved when, starting in May 1988, the AZT was administered intravenously. This omission is startling because it is the intravenous administration of AZT that provides the most direct test of your hypothesis that AZT toxicity is to blame for Ariel's condition. Your hypothesis would predict that switching form the weaker oral dosage of AZT to the much more highly potent IV form of AZT should have made Ariel dramatically worse. But the results of her treatment contradict your hypothesis--so you omit them form your version. Classic Pseudoscience.
Elizabeth Glaser's book In the Absence of Angels provides more details about Ariel's medical history:
When giving birth to Ariel, Elizabeth Glaser suffered from severe bleeding and received a blood transfusion that infected her with HIV. Ariel was exposed to HIV in her mother's breast milk. Ariel became ill in the fall of 1985, with painful stomach cramps and severe anemia (E. Glaser (1991). In the Absence of Angels: A Hollywood Family's Courageous Story. G. P. Putnam's Sons. New York: pp 45-46). She remained ill for months with intestinal and other complaints, and she was found to be HIV-positive in May of 1986 (E. Glaser (1991) pp 45-46). Her CD4 T-cell count was 4 (E. Glaser (1991) p 56).
Ariel improved with gamma-globulin therapy and was able to start kindergarten in the fall of 1986 (E. Glaser (1991): pp 80-81). During the summer of 1987, she became progressively weak and complained of "terrible stomach pains" (E. Glaser (1991): p 87-88). In August of 1987 Ariel's mother asked her pediatrician to place Ariel on AZT but was told that it was not approved for use in children (E. Glaser (1991) p 56). In November-December 1987, Ariel was hospitalized with pancreatitis (E. Glaser (1991) p 98). At this stage of her illness--two years after she first became sick with abdominal pain and anemia and 18 months after having been diagnosed with AIDS-- her mother describes her as:
Ariel's progressive 2-year deterioration had occurred in the absence of AZT.
She started oral AZT in December 1987, but it had no impact on the course of Ariel's illness (E. Glaser (1991) p 105). Her weakness progressed and by February 1988, she was unable to walk or talk (E. Glaser (1991) p 110). In March of 1988, she became critically ill and was hospitalized with pneumonia. At that time brain atrophy was found, a recognized complication of AIDS (E. Glaser (1991) p 112-113).
In May of 1998, based upon the preliminary results of a clinical trial underway at the NIH, Ariel was treated with intravenous AZT. This therapy would deliver the drug directly in to Ariel's bloodstream, bypassing her diseased gastrointestinal tract, and by administering it as a continuous infusion, the IV approach could maintain the desired levels of AZT in Ariel's blood around-the-clock. (E. Glaser (1991) p 130-136).
This is the point in Ariel's medical history in which the hypothesis suggested by Forty Mules is put to the critical test. Will intravenous AZT kill this emaciated, mute, and limp child?
In fact, no. At first there was no change in Ariel's condition. Then her mother reports:
For the next six weeks Ariel showed steady improvement in her neurological condition:
Franklin, excellent explanation of the Glaser's story, much more in depth than what I put up. Between my reading, your information and Forty's ignorance, I have decided to pick up the Glaser's book, add their charity to my giving list, and suggest Jake to the student life as a speaker. Thanks.
You either made it up yourself or copied it from somewhere else--but you didn't find it in the paper by Laurent-Crawford et al.
My guess is that he copied and pasted it from here http://www.virusmyth.net/aids/data/ept4cells.htm
and moved the quotation marks to falsely attribute the Perth Group's misinterpretation of the paper to the authors.
Here is what the perth group wrote:
And here is what Maniotis wrote:
The way that the Perth group take small quotes from "orthodox" scientists and weave them into their own misinterpreations and misrepresentations is already dishonest and deceptive. Read Judge Sulan's comments about this practice in his verdict from the recent appeal hearing in Australia.
Maniotis takes this misinterpretation to a new level of dishonesty by moving the quotation marks so that the Perth Group's words are falsely attributed to Laurent-Crawford et al.
If it is not ignorance on your part it is a deliberate ploy to misrepresent the truth, i.e. lying.
Ignorance might have been an excuse some time ago. He has been made aware of this distinction several times in this thread alone.
AZT toxicity is manifest clinically as mitochondrial toxicity due to inhibition of Mitochodrial DNA polymerase Gamma. Mitochodral toxicity causes the very obvious clinical symptoms of muscle weakness, inability to walk and talk, liver toxicity, liver failure, neurological toxicity with neuropathy, demyelination of the nervous system, and bone marrow suppression. Notice how many of the symptoms of so called "end stage AIDS" resemble this profile.
Mitochondrial toxicity explains Ariel's rapid deterioration shortly after starting AZT in December 1987. " By January there was no positive effects (from the AZT) and she became weaker and now was unable to walk or talk." Quoted from; http://www.paulmichaelglaser.org/elizabeth.html
My comment in parentheses.
Inability to walk or talk is NOT an opportunistic infection. This is a direct result of mitochondrial toxicity from AZT, and the same symptoms are seen in the videos of Kimberly Bergalis during her Senate Testimony. Kimberly appeared in a wheel chair and was obviously suffering from muscle weakness and difficulty talking, clear signs of mitochondrial toxicity from AZT. Kimberly also died of AZT toxicity, not AIDS.
http://tmh.floonet.net/articles/poisoned.shtml
AZT tablets are taken orally and absorbed by the GI tract. The AZT then enters the portal veins leading to the liver via "first pass clearance". Google first pass liver clearance to learn about it. This first pass to the liver delivers toxicity directly to the liver. When the route of administration is switched from oral to Intravenous, there is no first pass to the liver. This results in a temporary reduction in hepatotoxicity, as the the drug is delivered directly to the systemic circulation causing systemic mitochondrial toxicity and eventual death.
This switch in route of administration from oral tablets to IV AZT explains the temporary improvement in Ariel Glaser's clinical condition with a reduction in hepatotoxicity, and a temporary improvement in hepatic function. In spite of this temporary improvement, Ariel succumbed to systemic toxic effects of AZT in August 1988. Ariel received AZT from Dec 1987 and died August 1988, a span of 9 months of AZT treatment. According to the CDC, AIDS takes 10 years from onset of diagnosis to cause death. The rapidity of Ariel's clinical deterioration, and her symptoms of muscle weakness indicates death from AZT toxicity, not death from AIDS.
The temporary clinical improvement in Ariel's condition after switching from oral tablets to IV AZT DOES NOT indicate that AZT is a "miraculous life-saving drug", which it is not. It merely indicates less liver toxicity from changing the route of administration to avoid first pass liver clearance.
Ariel Glaser and her parents were betrayed by the very same doctors and institutions they trusted to help them. Ariel was a sacrificial victim to AZT toxicity, sharing he same fate as the hundreds of thousands of gay drug users, and poor minorities, in death from AZT toxicity from 1987 to 1997.
see this quote which illustrates a case of a genetic disease called Alpers Syndrome in which there is mitochodrial dysfunction similar to the effect of AZT on the mitochondria:
http://www.hivforum.org/publications/mitochondrial_toxicity.pdf
quote:Clinical aspects of DNA polymerase gamma activity, by Robert Naviaux, MD, PhD
The striking overlap between the symptoms of an inherited mitochondrial disease (i.e. Alpers syndrome) and the toxicities related to the nucleoside analogs zidovudine (AZT) and FIAU suggest that they are all mediated by the same mechanism--mitochondrial DNA polymerase gamma deficiency.
Dr. Naviaux and colleagues developed an in vitro assay that can detect mitochondrial polymerase from different tissue samples. He illustrated the use of this assay in a case report of a boy who developed normally until the age of 19 months, when a viral infection was followed by ataxia, encephalopathy, a hypotonic state, lethargy, poor feeding, and hypoglycemia. The assay showed that mitochondrial DNA content was 30% of normal in skeletal muscle and 25% of normal in liver. Despite treatment for neurodegenerative disorders, the boy suffered six more setbacks, culminating in rotaviral gastroenteritis, liver failure, cortical blindness, and death.
Liver biopsy showed steatosis and fibrosis, findings indicating chronic liver failure that had remained occult until the boy's final illness. Magnetic resonance imaging of the brain had been completely normal despite profound seizures and encephalopathy. But autopsy revealed significant loss of neuronal and cerebellar Purkinje cells.
This case illustrates apparent developmental shutdown of polymerase gamma activity.
Mitochondrial DNA depletion syndrome resembles Alpers syndrome in that both may be characterized by developmental regression, encephalopathy, hepatopathy, and sharp decreases in tissue levels of mitochondrial DNA.
Nucleoside reverse transcriptase inhibitors (NRTIs) deplete mitochondrial DNA by inhibiting DNA polymerase gamma, which regulates replication of mitochondrial DNA. Clinical symptoms that may be linked to mitochondrial toxicity include many already-identified NRTI side effects: polyneuropathy, myopathy, cardiomyopathy, hepatic steatosis, lactic acidosis,and pancreatitis.
Endquote.
for more information see; reviewingaids DOT com
Dear All,
I haven't been able to post for 2 days. Tara says I'm not blocked, so here goes.
As I am at home this weekend, and the Laurent-Crawford paper is sitting on my desk since I copied verbatim the quotes I posted above on Thursday, I won't be able to check it until Monday. I took the trouble of typing out those 2 paragraphs from the paper myself on Thursday, for Franklin. I can see they made no impact or even gave him pause for thought. The point is that Montagnier's group was aware of the mycoplasm issue, and were among the first to demonstrate it in a controlled fashion in vitro.
Although you all want to ignore the mycoplasm elephant in the AIDS clinic, I see I have struck some nerves. This is good. However, I do remember reading, and it will have to wait till Monday to check again:
" in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, whereas maximal virus production occurred at Days 10-17."
If this is an extract from Eleni's work in Genetica which I quoted above when I said she was correct that effect precedes cause in this critical cell culture experiment by Laurent-Crawford et al., or if it is in a chapter I lifted from a book I have written, and not from Laurent-Crawford directly, I will apologize to Franklin on Monday when I can look at the paper again. I can admit making such a mistake if I am wrong.
However, contrary to what you suggest, it wasn't meant to mislead-but point out that Montagnier's group was among those who demonstrated a potential role for mycoplasm in fatal immune defficiency, which prompted some of you to correct my spelling mistakes/attack my credibility, etc-the usual response predictable from folks who have a lot to lose I guess you all like the deep structure advanced by the likes of C. Gajdusek too much to ever question your own assumptions-a critical point I made above regarding "slow infections-and the origin of the science that postulated them-that was also ignored. Care to comment on Gajdusek's "slow viruses, or "Blumberg's blood polymorphisms, instead of correcting my misspelling of the word "counselling?"
I notice that there is a complete avoidance of issues that are raised. The point is that mycoplasm infections, as I stated, and as Lo and others found (as well as Montagnier's group which was the reason I posted this statement from Genetica's summary of the work, and from Laurent-Crawford's work directly), mycoplasmas have always been an important pathogen for "slow" yet cryptic infections. All I was hoping for was an acknowledgment of this issue. It is clear that you all are quite passionate in the defense of your views, and try to provide arguments in support. It isn't as if someone here will come up with "the final proof." It would be absurd in cancer research to say, "aha!" "now this proves, once and for all that metastastic cells all need to express glycoprotein X in order to be fatal." Why should it be any different for acquired immune deficiency?
Franklin, Robster; :
My reference to this paper was and is appropriate in the context of any discussion re: mycoplasm association to AIDS, especially since Montagnier's patient 1, and all of the work based on Patient 1's and others during this period of "LAV" or lymphodenopathy ASSOCIATED "virus" beginnings, must be tempered with the knowledge that the "isolates" (especially from patient 1) were obtained from a man with lymphadenopathy, who had been treated the year before for syphilis, twice for gonnorhea, he had herpes 1 and 11, plus cytomegalovirus.
Perhaps patient 1 was not the ideal patient from which to "isolate" "LAV" and characterize his serum on fresh lymphocyte cultures as described by Montagnier et al., (Barre-Sinoussi, F,m J.C. Chermann J.C., Rey F., Nugeyre MT., Chamaret, S., Gruest J., Dauguet C., , Axler-Blin C., Vezinet-Brn F., Rouzioux, C., Rozenbaum R., & Montagnier L. 1983 Isolation of a T-lymphotropic retrovirus from a patient at risk for Acquired Immune Deficiency Syndrome. Science 230: 868-871).
You might want to read it sometime-or even reference it when you are asked to provide "the paper" that "proves" "HIV" causes "AIDS," because this is the closest thing to THE paper that "proves" that "HIV" (LAV) "causes," "is associated with," is one of the many "pathogenic" signatures of acquired immune deficiency, because it was taken from a relatively healthy patient who harbored a spectrum of sexually acquired illnesses, and who was treated the year before for syphilis and 2 cases prior to that of gonorrhea. I'm surprised you AIDS apologists don't cite it more often when we ask you to provide the paper or papers that proves that "HIV" causes "AIDS?" Gallo et al., in order to AMPLIFY the signals detected by Montagnier's group when he borrowed the virus isolate from them (not purify it), used HT cells, and other human cancer cells oxidized by a number of agents that are known to stimulate the release of HERV's (human endogenous retroviral sequences), and were not really as good in vitro models of "HIV" pathogenicity, since they employed cancer cells instead of healthy human lymphocytes.
Regarding the plagerism charge, I just posted those refs because I had
them and thought you all might want them, and there was a lengthy
discussion going on at the time with Keven and others about fungal
infections and "HIV-negative" patients, but no mention of ICL. I didn't
think it was plagerism to quote scientific references.
My opening paragraph to the list of references I pasted was meant to be ironic, that's why it doesn't appear exactly like the link I got the references from, which you linked.
Regarding the stupidity charges, and the shill charges, and the charges of being misleading, lies about me telling patients what to do, funeral expenses, logical F-Ups, lack of interest in discussing what I have posted about our own work with Alu, etc., what can I say?
RE: Adele, and Jeffreys,
"The paper says low TLC can predict AIDS or death in HIV kids. It DOESN'T
say high TLC ABSOLUTELY GUARANTEES that a 3 year old can't possibly die of
AIDS. That's Andrew's logical f-up and it looks kind of dumb in someone
who's a professor supposedly."
No it doesn't say that Adele-you are quite right about the fact that it doesn't predict the outcome of higher values, but this fact doesn't matter in the context of my question-is AIDS a disease of too few lymphocytes. And you are right too, Mr. Jeffreys about the poor correlation in this study, especially amongst a population of children that were being poisoned. For instance, virological failure is a technical term among "HIV-AIDS" proponents that simply means a drug has failed to suppress virus because it doesn't work and has killed the recipient, and the AIDS establishment loves to study how drugs affect hundreds of hundreds of thousands of folks, and then attribute those morbid effects to a phantom virus's ravages or mutability instead of drug toxicity. A good recent example in support of this charge was advanced by none other than the cat-man's feline immune deficiency group led by Max Essex:
January 11, 2007 in the New England Journal of Medicine, it was reported by Max Essex's group that nevirapine increased the failure of the drug cocktail by only 41.7% compared to controls:
"Nevirapine remains central to the prevention of mother-to-child transmission of human immunodeficiency virus type 1 (HIV-1) and to combination antiretroviral treatment throughout much of the developing world. Nevirapine administered as one dose to the mother and one to the newborn reduces mother-to-child transmission of HIV-1 by 41 to
47%, and well over 875,000 women and infants have received a single dose of nevirapine. A single dose of nevirapine is the cornerstone of the regimen recommended by the World Health Organization (WHO) to prevent mother-to-child transmission among women without access to antiretroviral treatment and among those not meeting treatment criteria. However, nevirapine resistance is detected (with the use of standard genotyping techniques) in 20 to 69% of women and 33 to 87% of infants after exposure to a single, peripartum dose of nevirapine. Among 60 women starting antiretroviral treatment within 6 months after receiving placebo or a single dose of nevirapine, no women in the placebo group and 41.7% in the nevirapine group had virologic failure (P<0.001).Women who had received a single dose of nevirapine had significantly higher rates of virologic failure on subsequent nevirapine-based antiretroviral treatment than did women who had received placebo. This apparently deleterious effect of a single dose of nevirapine was concentrated in women who initiated antiretroviral treatment within 6 months after receiving a single dose of nevirapine. We did not find that a previous single dose of nevirapine compromised the efficacy of subsequent nevirapine-based antiretroviral treatment in women who started antiretroviral treatment 6 months or more after delivery. Among the 30 HIV-infected infants, a single dose of nevirapine (one each to mother and infant) as compared with placebo was associated with significantly higher rates of virologic failure and smaller CD4+percentage increases in response to subsequent nevirapine-based antiretroviral treatment" ( Lockman S. et al., Response to Antiretroviral Therapy after a Single, Peripartum Dose of Nevirapine. The New England Journal of Medicine 356 January 11, 2007).
I suppose only 875,000 black mother-infant pairs isn't too many to try a drug out that was withdrawn in the US by its own manufacturer for toxicity, and whose toxicity data in Africa were suppressed or rewritten by that angel of compassion, Edmond Tremont (according to Johnathan Fishbein's whistle-blowing and subsequent firing from the NIH), in order to demonstrate that it is better to poison black mother-infant pairs AFTER 6 months rather than BEFORE 6 months of age. Little boo-boo's like this are necessary, I suppose, in order to save the African continent from the WHO statisticians. Nothing to get concerned about though. The current Bush plans and budgets for the current roll-outs will make this 875,000, 47% increase in "breakthrough" boo-boo "virological failure" appear small in comparison.
It just struck me as strange when I saw Eliza Jane's blood work (because other than the amoxicillin and whatever other undisclosed antibiotic they gave her in the PICU to treat her for cardiac arrest, she was recorded as being severely neutropenic, and presented at the ER with 10,800 total lymphoctes. The neutropenia is on the amoxicillin package insert (that I
posted above), and the high lymphocyte count COULD have been the result of
her 2-week ear infection (even children that don't have AIDS get ear infections-especially when their canals are very small-they tend to outgrow them as they age and grow and as their immune systems mature).
Alternatively, a release of lymphocytes at a level that is twice normal
COULD have been the result of a massive immune reaction as they are
released into the peripheral circulation during such "cytokine storms"
that occur as a result of a massive and pathological reactions to a drug
or toxin (I know adults and children have somewhat different levels, as do
adults compared to other adults, but there is a normal reference range if
you look on any blood work from any clinic or hospital in the world). My question still is, is AIDS (amongst ARV-naive persons) a disease of too many lymphocytes, like Eliza Jane apparently had, or too few lymphocytes?
Her organ weights and distended abdomen noted by the attendings upon
admission (but not by anybody else before) were consistent with a massive
and SUDDEN release of fluids escaping from her vasculature (along with
the fluid added from the many IV's they gave her at the hospital along
with other undisclosed antibiotics during her cardiac arrest crisis period
and in the PICU).
Remember this from earlier?
"Beta lactam antibiotics-
Anaphylactic reactions manifested by urticaria, flushing, pruritus,
laryngeal edema, and CARDIOVASCULAR COLLAPSE may occur within minutes or,
less frequently, HOURS after administration of beta lactam antibiotics
(ie, drugs that have a common beta lactam ring structure)."
"SIDE EFFECTS AND SPECIAL PRECAUTIONS
Gastro-intestinal side effects including diahrroea, nausea and vomiting
may occur quite frequently. Pseudomembranous colitis has also been
reported.Super-infection is relatively common. Doses should be reduced in
severe renal failure."
Nausea and vomiting occurred after Eliza Jane's second dose of
amoxicillin. Eliza Jane's kidneys were measured at 146% of normal, without
significant damage exhibited microscopically, consistent with massive
edema and recent injury.
"Unpredictable reactions occur independent of the dose and route of
administration and reflect such factors as drug intolerance, allergy, and
other idiosyncratic responses.
Are there any words here that you would like me to explain?
"These reactions seem to preferentially affect certain body systems, most
commonly blood, skin, and liver."
Eliza Jane's bood work was abnormal to the extent that she was profoundly
anemic and exhibited a low hematocrit (Her hemoglobin and hematocrit
counts were low (6.3 g/dl instead of 12-16g/dl, and 21% instead of 37-48%,
respectively). (2). Her neutrophils were measured at 12% (normal=45-74%)
(2). Her monocyte percentage was in the normal range at 8% (normal is
4-10%) and her platelet count (214 k/µl) was in the normal range (130 k/µl
-400 k/µl) (2).
2=Medical record # 856441, Valley Presbyterian Hospital, 15107 Vanowen Street, Van Nuys, Ca, 91404.
And as indicated on the amoxicillin package insert:
"Additional unique life-threatening reactions caused by beta-lactam
antibiotics are referred to as "late" reactions. They include such events
as hemolytic anemia, Stevens-Johnson syndrome, and exfoliative
dermatitis."
Is there something about the words, "life-threatening" that cause confusion here? Or "late reactions?" Are you gonna still tell me that that entire literature I posted was from pre-sensitized individuals only? I think you are wrong on this score-go and check. I gave you some VAERS data before in support of my claims that persons do not have to be sensitized to anything and many still die of unfortunate reactions, unpredictably.
Her liver findings were abnormal as well: Eliza Jane autopsy showed liver
changes consistent with an immune reaction to amoxicillin, which in some
cases of acute toxicity has been noted to resemble
pregnancy-fat-like-accumulation and steatosis (refs provided above).
I emphasize, Mr. Jeffreys, that most if not all of the stats regarding correlations between CD4, total lymphocytes
counts, and prediction to death from "AIDS" have been done on ARV drugged
people-so the value of these stats needs to be dissociated from the
effects of the meds on the enrolled populations (of Human guinea pigs
coerced, brow-beaten, threatened, frightened to death into taking these
vile poisons), because most of the meds claim on their package inserts
that they are extremely suppressive (in about 1/2 of patients) to all
blood cells-necessitating transfusions in many cases (which are themselves
extremely dangerous and immune suppressive treatments-look again at the
refs I pasted above regarding the frequencies of transfusions in AIDS
patients and also the immune-suppressive nature of especially the
DNA-chain terminating drugs, as well as some of the protease inhibitors).
When I presented Eliza Jane's blood work to a number of clinical
pathologists here and elsewhere for their advice, and I asked them how on
earth a person with a total lymphocyte count of 10,800 could be suffering
from PCP, they said, its impossible. PCP is almost universally, I was
told, a disease associated with too few lymphocytes/a weakened immune
system. This is my problem-not with the correlation between CD4 and TL
counts. My question was do AIDS-defining illnesses (such as PCP) occur in
drug-naive persons with high total lymphocyte counts? Do you understand
the context of the question now?
It is important because when we all learned that Ribe was facing charges
for cooking data in the past that got parents thrown in jail for life,
many of us realized that one really can't trust the coroner's changed
reports regarding Eliza Jane's autopsy findings, and perhaps only could
rely on that data that was obtained at the hospital admission (such as her
total lymphocyte count/blood work).
Adele, and Mr. Jeffreys, I suppose I should thank you for finally answering my question: you all agree that:
"The Lancet paper says low TLC can predict AIDS or death in HIV kids." Thus AIDS is a disease that is best characterized by too few (about 1000 or less), rather than almost 11,000 total lymphocyte counts?
So why would you insist that a perfectly healthy child, with clear lungs as determined by 3 physicians, and an ear-ache, died 36 hours after imbibing the drug with perhaps the
most frequently chronicled number of adverse reactions in the world, next
to ARVS and cancer chemo is an AIDS case?
Thanks much, finally, for your answer to my question.
More about Simonson, Klausner, flu vaccines, hep b vaccines, later. I want to see if I still am blocked from posting...and responding to your concerns.
I notice that there is a complete avoidance of issues that are raised.
Read the literature. The role of mycoplasmas in AIDS was investigated.
Montagnier looked at one cell line, CEM, that was contaminated with mycoplasma penetrans [not m. fermentans(incognitus)]. There is no strong association between mycoplasmas and AIDS by antibodies or PCR.
There is some evidence that mycolpasmas may affect the rate of progression but the aetiological factor is HIV. Montagnier does not argue with this.
The fact that you selectively quote (and get it wrong) Montagnier from 1990 rather than look at the literature from the intervening 17 years suggests to me that you intend to deceive the people reading this blog.
Dr. Maniotis,
Keep up the good work, your posts are so solid, yet they just want to focus on fine details. Typical Adhominem atatcks, like they do with Kary Mullis "he surfs and likes girls so hes a kook"
They dont want to address that mycoplasma incognitus has got an animal model, unlike hiv, hpv and hep c. as Dr. Lo showed.
read www.projectdaylily.com this mycoplasma was part of the bioweapon program, you can read the first chapter for free, its scary.
With all the copying pasting, heat of the moment stress, there might be some mistakes. youd better have some good evidence to accuse someone of plagarism, look at the bigger picture, montegnier did say in 1990 mycoplasma was a key cofactor, and that hiv might be benign.............I doubt fully anyone here would intentionally plagerize, whats the need when Dr. montagnier meant what he said back then?
Montagnier looked at one cell line, CEM, that was contaminated with mycoplasma penetrans. Montagnier speculated that mycoplasmas might play a strong role in the rate of progression to AIDS.
Since 1990 it has been found that there is not a consistent pattern of mycoplasma infection in AIDS cases, mycoplasma DNA is not found in PBMCs of AIDS patients and mycoplasma does distinguish between progression and non-progression.
Montagnier has made it abundantly clear since 1990 that HIV is the aetiological agent in AIDS.
Thanks Cooler! I intend to. They won't even touch the Gajdusek issue I raised above-their model pedophile hero who gave birth to "slow viruses" along with Blumberg-who was in fact studying blood group polymorphisms, associations of HbsAG with Down syndrome, leukemia, and healthy black australian aboriginals and Southeast Asians. I'd rather go surfing with Kary anyday than be alone with Gajdusek, his apeteties, and his "slow viruses" that Laura Manueledes debunked years ago.
Concession to Adele and Jeffreys,
I noticed that a small part my post above was corrupted: it happens to be a critical part so here it is so as to avoid more charges of plagerism, lying, distorting, stupidity, shilling, being dumb, etc. It highlights sort of a concession on my part to Adele and Jeffreys. But I must thank them for finally answering the question that AIDS is thought of typically as a disease of too few rather than too many lymphocytes, as in the case of EJ.
RE: Adele, and Jeffreys who both pointed out that:
"The paper says low TLC can predict AIDS or death in HIV kids. It DOESN'T
say high TLC ABSOLUTELY GUARANTEES that a 3 year old can't possibly die of
AIDS. That's Andrew's logical f-up and it looks kind of dumb in someone
who's a professor supposedly."
No it doesn't say that Adele-you are quite right about the fact that it doesn't predict the outcome of higher values, but this fact doesn't matter in the context of my question-is AIDS a disease of too few lymphocytes? And you are right too, Mr. Jeffreys about the poor correlation in this study, especially amongst a population of children that were probably being poisoned.
For instance, virological failure is a technical term among "HIV-AIDS" proponents that simply means a drug has failed to suppress virus because it doesn't work and has killed the recipient (Arthur Ashe, Rodolf Neurev, Hudson, a generation of high-dosed men at the peak of their sexual but mostly drug revolution, etc., and the AIDS establishment loves to study how drugs affect hundreds of thousands of folks, and then attribute the often frequent morbid effects of these poisons to a phantom virus's ravages, or its mutability (remember-like gives rise to like, Franklin-)instead of drug toxicity. A good recent example in support of this charge was advanced by none other than the cat-man's feline immune deficiency group led by Max Essex:
January 11, 2007 in the New England Journal of Medicine, it was reported by Max Essex's group that nevirapine increased the failure of the drug cocktail by only 41.7% compared to controls:
"Nevirapine remains central to the prevention of mother-to-child transmission of human immunodeficiency virus type 1 (HIV-1) and to combination antiretroviral treatment throughout much of the developing world. Nevirapine administered as one dose to the mother and one to the newborn reduces mother-to-child transmission of HIV-1 by 41 to 47%, and well over 875,000 women and infants have received a single dose of nevirapine. A single dose of nevirapine is the cornerstone of the regimen recommended by the World Health Organization (WHO) to prevent mother-to-child transmission among women without access to antiretroviral treatment and among those not meeting treatment criteria. However, nevirapine resistance is detected (with the use of standard genotyping techniques) in 20 to 69% of women and 33 to 87% of infants after exposure to a single, peripartum dose of nevirapine. Among 60 women starting antiretroviral treatment within 6 months after receiving placebo or a single dose of nevirapine, no women in the placebo group and 41.7% in the nevirapine group had virologic failure (P<0.001).Women who had received a single dose of nevirapine had significantly higher rates of virologic failure on subsequent nevirapine-based antiretroviral treatment than did women who had received placebo. This apparently deleterious effect of a single dose of nevirapine was concentrated in women who initiated antiretroviral treatment within 6 months after receiving a single dose of nevirapine. We did not find that a previous single dose of nevirapine compromised the efficacy of subsequent nevirapine-based antiretroviral treatment in women who started antiretroviral treatment 6 months or more after delivery. Among the 30 HIV-infected infants, a single dose of nevirapine (one each to mother and infant) as compared with placebo was associated with significantly higher rates of virologic failure and smaller CD4+percentage increases in response to subsequent nevirapine-based antiretroviral treatment" ( Lockman S. et al., Response to Antiretroviral Therapy after a Single, Peripartum Dose of Nevirapine. The New England Journal of Medicine 356 January 11, 2007).
Not even Tara's website likes the Lockman/Essex paper-as it keeps cutting it off! I guess even the web-bots cringe at this boo-boo involving 875,000 human mother-infant guinea pigs!
But I will post it here to prove I ain't no plagerist!
Lockman S. et al., Response to Antiretroviral Therapy after a Single, Peripartum Dose of Nevirapine. The New England Journal of Medicine 356 January 11, 2007
read www.projectdaylily.com this mycoplasma was part of the bioweapon program, you can read the first chapter for free, its scary.
The scary part is that somebody could read this low quality fiction and mistake it for reality.
Project Day Lily An American Biological Warfare Tragedy
Typical Adhominem atatcks, like they do with Kary Mullis "he surfs and likes girls so hes a kook"
Do you mean Andrew's fascination with Gajdusek and paedophilia? This strikes me as being the perfect example of the ad hominem fallacy.
franklin said How did you miss the part about Ariel's neurologic condition showing dramatic improvement after three weeks of intravenous AZT? Perhaps because it is exactly the opposite result to that predicted by your theory that AZT toxicity was the cause of Ariel's illness. Not only did Ariel's illness progress for more than 2 years before she received any AZT, but switching from oral AZT to the more intense intravenous AZT made her dramatically better!
Dear franklin, Even a first year nursing student with a rudimentary knowledge of human physiology will know that the temporary improvement in Ariel's condition after switching from oral to IV AZT does not equate with any evidence of drug efficacy. Instead it is a perfect example of reduction in toxicity by avoiding first pass through the liver.
AZT Toxicity is manifest clinically as mitochondrial toxicity due to inhibition of Mitochondrial DNA Polymerase Gamma. Mitochondrial toxicity causes the very obvious clinical symptoms of muscle weakness, inability to walk and talk, liver toxicity, liver failure, neurological toxicity with neuropathy, demyelization of the nervous system, and bone marrow suppression with pancytopenia, anemia, and granulocytopenia.
Mitochondrial toxicity explains Ariel's rapid deterioration shortly after starting AZT in December 1987. " By January there was no positive effects and she became weaker and now was unable to walk or talk." Quoted from the Paul Michael Glaser web site:
Inability to walk or talk is NOT an opportunistic infection. This is a direct result of mitochondrial toxicity from AZT, same symptoms were seen in the videos of Kimberly Bergalis during her Senate Testimony. Kimberly appeared in a wheel chair and was obvious suffering from muscle weakness and difficulty talking, clear signs of mitochondrial toxicity from AZT.
AZT taken as oral tablets is absorbed by the GI tract lining, then enters the portal veins and is delivered to the liver via "first pass clearance", delivering toxicity directly to the liver. The switch in route of administration from oral tablets to Intravenous AZT (peripheral arm vein is not a portal vein) explains the temporary improvement in Ariel Glaser's clinical condition with a reduction in hepatotoxicitiy, and a temporary improvement in hepatic function. In spite of this temporary improvement, Ariel succumbed to bone marrow suppression and other systemic toxic effects of AZT in August 1988. Ariel received AZT from Dec 1987 and died August 1988, a span of 9 months of AZT treatment. According to the CDC, AIDS takes 10 years from onset of diagnosis to eventual death. The rapid deterioration Ariel's clinical picture after treatment with AZT was most compatible with death from AZT toxicity, not death from AIDS.
Elizabeth and Ariel Glaser's were both betrayed by their doctors, the medical system and institutions they entrusted to help them. They both succumbed to AZT toxicity, sharing the same fate as hundreds of thousands of other HIV positive gays, drug users, blacks and poor minority groups who died from AZT treatment in the decade after 1986. No wonder the government of South Africa is opposed to these deadly drugs, and offers instead lemon and garlic, benign foods incapable of killing the patient.
Begin quote:
Clinical aspects of DNA polymerase gamma activity by Robert Naviaux, MD, PhD
The striking overlap between the symptoms of an inherited mitochondrial disease (i.e. Alpers syndrome)and the toxicities related to the nucleoside analogs zidovudine (AZT) and FIAU suggest that they are all mediated by the same mechanism--mitochondrial DNA polymerase gamma deficiency.
Dr. Naviaux and colleagues developed an in vitro assay that can detect mitochondrial polymerase from different tissue samples. He illustrated the use of this assay in a case report of a boy who developed normally until the age of 19 months, when a viral infection was followed by ataxia, encephalopathy, a hypotonic state, lethargy, poor feeding, and hypoglycemia. The assay showed that mitochondrial DNA content was 30% of normal in skeletal muscle and 25% of normal in liver. Despite treatment for neurodegenerative disorders, the boy suffered six more setbacks,culminating in rotaviral gastroenteritis, liver failure, cortical blindness, and death. Liver biopsy showed steatosis and fibrosis, findings indicating chronic liver failure that had remained occult until the boy's final illness. Magnetic resonance imaging of the brain had been completely normal despite profound seizures and encephalopathy. But autopsy revealed significant loss of neuronal and cerebellar Purkinje cells.
This case illustrates apparent developmental shutdown of polymerase gamma activity. Mitochondrial DNA depletion syndrome resembles Alpers syndrome in that both may be characterized by developmental regression, encephalopathy, hepatopathy, and sharp decreases in tissue levels of mitochondrial DNA.
Nucleoside reverse transcriptase inhibitors (NRTIs) deplete mitochondrial DNA by inhibiting DNA polymerase gamma, which regulates replication of mitochondrial DNA.
Clinical symptoms that may be linked to mitochondrial toxicity include many already-identified NRTI side effects: polyneuropathy, myopathy, cardiomyopathy, hepatic steatosis, lactic acidosis, and pancreatitis. ENDQUOTE
for more information see www.reviewingaids DOT com
And you are right too, Mr. Jeffreys about the poor correlation in this study, especially amongst a population of children that were being poisoned.
So now the Lancet study isn't so useful to you? You're shifting your argument and claiming that the correlation between CD4% and TLC is influenced by some undefined "poison."? Perhaps you can look at the citations on the correlation between TLC and CD4 and see if you can find any evidence to support this new claim? The correlation doesn't seem much better in this study, which also shows that TLC correlates far more closely with absolute CD8 T cell counts:
My question still is, is AIDS (amongst ARV-naive persons) a disease of too many lymphocytes, like Eliza Jane apparently had, or too few lymphocytes?
Your question makes no sense, because it's based on your own ignorance of the immunology literature. The science has progressed a little further than just counting lymphocytes. If you really want to frame it like this, AIDS is a disease of too many lymphocytes that don't work and too few that do.
Here is doctor Maniotis, expounding on his views in person:
http://www.youtube.com/watch?v=HIX35HyQXg8
I'm not 100% certain, but I think this represents the first collaboration between a tenured member of the faculty at the University of Illinois at Chicago and Gary Null. It must have been filmed recently because he mentions the Klausner NEJM letter from March 2006 (he suggests that Jeff Klausner is Richard Klausner). He also makes the usual false claims about no chimpanzees developing AIDS, etc. etc.
I would suggest paying particularly close attention to his closing "amusing story" about how terribly awkward it would be for a putative HIV positive vaccine recipient to explain that they had not in fact been infected by "catching HIV from some...um... er..er.. person...er...who is considered by the AIDS establishment to be high risk...that is blacks, homosexuals, people of color, and other people."
According to Maniotis, the source of this amusing story is his friend Jon Rappaport who runs a website called "No More Fake News," reporting on paranormal activity, US government mind control experiments on children and other such delights.
Maniotis also mentions both Etienne de Harven (now president of "Rethinking AIDS") and the old US Government Special Virus Cancer Program. I've often wondered why de Harven never seems to be mention his close involvement with the SVCP or include it on his CV (http://perso.orange.fr/sidasante/edh/edh.htm). As of 1963 de Harven sat on two program subcommittees (the PPLO and Electron Microscope subcommittees) - http://history.nih.gov/articles/SpecialVirusCaPrgm.pdf. He was still listed as a consultant to the SVCP in 1978 (http://www.boydgraves.com/svcp/), shortly before he left the United States and moved to Toronto in 1981.
Mitochondrial toxicity of AZT as pointed out by Dalakas and others:
Dalakas MC et al. Mitochondrial myopathy caused by long-term zidovudine therapy. NEJM. 1990;322(16):1098-1105 wrote:
"Before 1986, when zidovudine (formerly called azidothymidine [AZT]) was introduced...the number of patients with HIV-associated myopathy was small, and myopathy [muscle disorders] was considered a rare complication of HIV infection. During the past two years [1988-1989], an increasing number of patients receiving long-term zidovudine therapy have had myopathic symptoms such as myalgia (in up to 8 percent of patients), elevated serum creatine kinase levels (in up to 15 percent), and muscle weakness. These symptoms generally improve when zidovudine is discontinued...We conclude that long-term therapy with Zidovudine can cause a toxic mitochondrial myopathy, which... is indistinguishable from the myopathy associated with primary HIV infection."
Lewis W, Dalakas MC. Mitochondrial toxicity of antiviral drugs. Nat Med. 1995 May;1(5):417-22.
"Clinical manifestations of ANA [Antiviral Nucleoside Analogs, such as AZT] toxicity: It is self-evident that ANAs, like all drugs, have side-effects. However, the prevalent and at times serious ANA mitochondrial toxic side-effects are particularly broad ranging with respect to their tissue target and mechanisms of toxicity: ... Haematalogical toxicity [anemia, and other blood disorders] ... Myopathy [muscle disorders] ... Cardiotoxicity [heart disorders] ... Hepatic toxicity [liver disorders] ... Peripheral neuropathy [nerve damage]."
Chariot P, Gherardi R. Partial cytochrome c oxidase deficiency and cytoplasmic bodies in patients with zidovudine myopathy. Neuro muscul Disorders. 1991;1:357-363 reported:
"Long term therapy with [AZT] can induce a toxic myopathy associated with mitochondrial changes"
Hayakawa M et al. Massive conversion of guanosine to 8-hydroxy-guanosine in mouse liver mitochondrial DNA by administration of azidothymidine. Biochem Biophys Res Commun. 1991;176:87-93 reported that:
"typical mitochondrial myopathy has been reported to be expressed among many patients with AIDS treated with long-term azidothymidine (AZT) therapy" and "for AIDS patients, it is urgently necessary to develop a remedy substituting this toxic substance, AZT."
Coker R et al. Exacerbation of HIV-associated myopathy by zidovudine. AIDS. 1991;5(2):229-31 claimed that:
"A clinically significant myopathy that precedes the development of zidovudine associated mitochondrial myopathy has been a rarity in our experience."
Till M, MacDonnell KB. Myopathy with Human Immunodeficiency Virus type 1 (HIV-1) infection: HIV-1 or zidovudine?. Ann Int Med. 1990;113(7):492-4 reported that:
"In our review of our clinic patients who have received zidovudine therapy for more than 6 months, 16% (14 of 86 patients) have had persistently elevated creatine kinase values. Six percent of these patients (5 of 86) developed symptomatic myalgia and objective proximal muscle weakness. These 5 symptomatic patients had received zidovudine for an average of 45 weeks and had had creatine kinase elevations for several weeks before onset of symptoms. Of these 5 patients, 4 had creatine kinase values return to normal and symptoms resolve after zidovudine was withdrawn...Three patients were rechallenged with zidovudine: each had recurrent creatine kinase elevations at a dose of 600 mg/d. The zidovudine dose was increased to 1200 mg/d in 2 patients: after a few days, both developed recurrent muscle symptoms that again responded to dose reduction. ...Results of quadriceps muscle biopsies done on our patients who responded to zidovudine withdrawal showed severe myopathic changes without evidence of inflammatory infiltrates. Electron microscopy revealed many ultrastructural changes, including destruction of the sarcomere profile with z-band change in the form of streaming and rod bodies. Muscle mitochondria showed wide variation in size, swelling, degeneration and laminar bodies. ...There have been 40 case reports [to 1990] of patients who have developed myopathy while taking zidovudine (including our 5 symptomatic patients). Zidovudine therapy was discontinued in 34 of these patients and 26 improved."
Helbert M et al. Zidovudine-associated myopathy. Lancet. 1988 Sep 17;2:689-90 claimed that:
"A severe proximal myopathy, predominantly affecting the legs, seems to be a significant complication of long-term zidovudine therapy, even at reduced doses; it affected 18% of our patients who had received treatment for more than 200 days. Other drugs could not be implicated. The pathogenesis is obscure; the myopathy resolves on cessation of zidovudine, but not on dose-reduction, though there is then a risk of rebound encephalitis."
Blanche S et al. in "Persistent mitochondrial dysfunction and perinatal exposure to antiretroviral nucleoside analogues," Lancet, 1999 Sep 25 concluded that:
"We analysed observations of a trial of tolerance of combined zidovudine [AZT] and lamivudine and preliminary results of a continuing retrospective analysis of clinical and biological symptoms of mitochondrial dysfunction in children born to HIV-1-infected women in France....Findings: Eight children had mitochondrial dysfunction. Five, of whom two died, presented with delayed neurological symptoms and three were symptom-free but had severe biological or neurological abnormalities. Four of these children had been exposed to combined zidovudine and lamivudine, and four to zidovudine alone. No child was infected with HIV-1.."
" Our findings support the hypothesis of a link between mitochondrial dysfunction and the perinatal administration of prophylactic nucleoside analogues. Current recommendations for zidovudine monotherapy should however be maintained[!]. Further assessment of the toxic effects of these drugs is required!"
Neenyah Ostrom (07/12/2000) reviewed the Blanche study in the following way:
"The French study, led by Stephane Blanche at the Necker Hospital in Paris, was published in The Lancet. Of 1,754 mother-child pairs exposed to AZT during the mother's pregnancy (or just after birth, for the child), Blanche and colleagues discovered eight children whose mitochondria didn't function properly. The mitochondria are our cells' energy producing organelles; if they malfunction, neurological development is delayed, and the result can be fatal. Four of the children with mitochondrial dysfunction had been exposed to a combination of AZT and another anti-HIV drug, lamivudine; the other four had been exposed to AZT alone. "No child was infected with HIV-1," Blanche and co-workers pointed out."
"Five of the eight children developed "delayed" neurological symptoms (meaning they weren't present at birth, but became obvious later); two of these children died. The other three children "were symptom-free but had severe biological or neurological abnormalities," according to the French scientists."
"One of the two children with neurological symptoms who died, Patient A, was partially blind. When Patient A was 4 months old, an MRI showed that the child had demyelinating lesions in the brainstem (a primitive part of the brain that controls basic life functions). Over time, these lesions -- which were really just areas of dead brain tissue -- spread throughout the child's brain. Patient A's growth was "abnormal," according to the doctors, and the child vomited frequently. At 13 months of age, Patient A died from heart and lung disorders."
"Patient B died at the age of 11 months. At 4 months old, Patient B developed epilepsy as well as suffering severe deterioration of cognitive and motor abilities. This child, too, was found to have "diffuse demyelinating lesions associated with massive cortical necrosis," that is, widespread brain tissue death."
"The other children who developed symptoms of mitochondrial dysfunction had seizures, heart dysfunction, brain lesions (one child with, and one without, brain tissue death), blindness associated with a too-small head ("microencephaly," a problem identified earlier in babies treated in utero with AZT [5]), and numerous biochemical abnormalities (including abnormal liver and pancreatic enzyme levels, among others).
"In their discussion of how AZT probably contributed to the illness and deaths of these children, Blanche and colleagues noted that researchers at the US National Cancer Institute have demonstrated that AZT crosses the placenta from mother to fetus. In monkey fetuses, AZT is incorporated into the mitochondrial DNA. Fetal monkeys dosed with AZT for periods of time and with doses similar to those used for pregnant women developed mitochondrial dysfunction after birth, Blanche and co-workers pointed out. They added, 'The experimental [monkey] model does not show whether the toxic effects are reversible after birth. Also, it gives no insight into the possible clinical impact of this type of dysfunction throughout a tissue, especially a long time after the drug is stopped.... As with other drug-induced toxic effects in mitochondria, these lasting abnormalities may be associated with a symptomless constitutional dysfunction.' In other words: Many more children exposed to AZT in utero may have mutations in their mitochondria that we don't detect because they don't immediately produce identifiable symptoms. The type of mitochondrial illness observed in these eight children (out of 1,754 French children treated with AZT) was found in only 21 children out of 12 million studied in the United Kingdom."
"We are aware that the suggestion that antiretroviral drugs are toxic raises delicate issues," the French scientists wrote, concluding that "the current recommendations for zidovudine [AZT] monotherapy prophylaxis should be maintained." They added, however, "Pregnant women should be informed of the potential effects associated with these treatments during pregnancy."
"The UK's Committee on Safety of Medicines in Perinatal AZT: New warning on potential risk to infants. www.aidsmap.com. 1999 Jul 21, http://www.aidsmap.com/namsearch.htm/news/07jul99/story6.htm issued a warning to doctors about the risk of mitochondrial dysfunction in infants born to HIV infected mothers treated with zidovudine (AZT) to prevent vertical transmission."
Gerschenson M et al. Fetal mitochondrial heart and skeletal muscle damage in Erythrocebus patas monkeys exposed in utero to 3'-azido-3'-deoxythymidine. . AIDS Res Hum Retroviruses. 2000 May 1;16(7):645-44 reported that:
"3'-azido-3'-deoxythymidine (AZT) is given to pregnant women positive for the human immunodeficiency virus type 1 (HIV-1) to reduce maternal-fetal viral transmission. To explore fetal mitochondrial consequences of this exposure, pregnant Erythrocebus patas monkeys were given daily doses of 1.5 mg (21% of the human daily dose) and 6.0 mg (86% of the human daily dose) of AZT/kg body weight (bw), for the second half of gestation. At term, electron microscopy of fetal cardiac and skeletal muscle showed abnormal and disrupted sarcomeres with myofibrillar loss. Some abnormally shaped mitochondria with disrupted cristae were observed in skeletal muscle myocytes. Oxidative phosphorylation (OXPHOS) enzyme assays showed dose-dependent alterations. At the human-equivalent dose of AZT (6 mg of AZT/kg bw), there was an approximately 85% decrease in the specific activity of NADH dehydrogenase (complex I) and three- to sixfold increases in specific activities of succinate dehydrogenase (complex II) and cytochrome-c oxidase (complex IV). Furthermore, a dose-dependent depletion of mitochondrial DNA levels was observed in both tissues. The data demonstrate that transplacental AZT exposure causes cardiac and skeletal muscle mitochondrial myopathy in the patas monkey fetus."
All these folks are AIDS denialists! AZT was "the backbone" of the life-saving arsenal. The fact that AZT worked so well, like a virtual penicillin for viruses," can be seen by the fact that so little effort since AZT's 4 month "rapid" approval by the FDA, has been made to replace AZT with other drugs:
Despite the fact that AZT worked so well and was so "life-saving," Hayakawa's and other's suggestion of replacing the life-saving drug, AZT, with others was heard:
For example, here is a short list of the few additional "life saving drugs that have been improperly called or considered as "antiretrovirals" that have been aggressively developed and marketed by the pharmaceutical giants in collusion with the current Public Health Service administrations, proving how well AZT actually worked:
Agenerase (amprenavir),
GlaxoSmithKline; Combivir, lamivudine,
GlaxoSmithKline;
Crixivan, (indinavir, IDV, MK-639),
Merck; Emtriva, (FTC, emtricitabine),
Gilead Sciences;
Epivir, (lamivudine, 3TC Epzicom, abacavir
GlaxoSmithKline; Fortovase, (saquinavir),
Hoffmann-La Roche;
Fuzeon, (enfuvirtide, T-20),
Hoffmann-La Roche & Trimeris;
Hivid, (zalcitabine, ddC, dideoxycytidine),
Hoffmann-La Roche; Invirase,
(saquinavir mesylate, SQV),
Hoffmann-La Roche; Kaletra,
(lopinavir and ritonavir),
Abbott Laboratories; Lexiva, (Fosamprenavir Calcium), GlaxoSmithKline; Norvir,
(ritonavir, ABT-538),
Abbott Laboratories; Rescriptor, (delavirdine, DLV),
Pfizer; Retrovir (zidovudine, AZT, azidothymidine, ZDV) GlaxoSmithKline;
Reyataz, (atazanavir sulfate),
Bristol-Myers Squibb; Sustiva, (efavirenz),
Bristol Myers-Squibb; Truvada, (tenofovir disoproxil/emtricitabine),
Gilead Sciences, Inc.; Videx EC, (enteric coated didanosine),
Bristol Myers-Squibb; Videx, (didanosine, ddI, dideoxyinosine),
Bristol Myers-Squibb;
Viracept, (nelfinavir mesylate, NFV),
Agouron Pharmaceuticals; Viramune, (nevirapine, BI-RG-587), Boehringer Ingelheim; Viread, (tenofovir disoproxil fumarate),
Gilead; Zerit, (stavudine, d4T)
Bristol Myers-Squibb; Ziagen (abacavir) GlaxoSmithKline.
If 10mg of each of these would be given, perhaps no "breakthrough" escape viruses would have emerged. A lot to give a pregnant woman, however, or her infant. 1 shot nevirapine is better, as it only induces 41% resistance after a single dose.
Dear Forty Mules,
Here is what you wrote:
This is a good first step for you. In the scientific method, it is known as:
"Generating a hypothesis".
Unfortunately, you seem to have mistaken it with the step known as:
"Drawing a conclusion".
Your hypothesis states that the difference in Ariel's response to oral vs. intravenous AZT is explained by the lack of "first pass through the liver" when the AZT is delivered intravenously. You hypothesize that the lack of "first pass through the liver" makes intravenous AZT less toxic than oral AZT, explaining Ariel's dramatically improved neurologic condition following three weeks of round-the-clock administration of intravenous AZT.
You then provide some background information on AZT toxicity:
However, you fail to use this information to evaluate your hypothesis. To scientifically evaluate a hypothesis, one must use the hypothesis to make predictions. The scientist then gathers data to see if the predictions are correct. If the predictions are not borne out by the data, the scientist can reject the hypothesis as false.
Let's attempt this exercise with your hypothesis. Your hypothesis predicts that toxic effects of AZT that depend on "first pass through the liver" will be worse with oral AZT than with intravenous AZT. To determine if Ariel Glaser's clinical picture is consistent with this hypothesis, we need to understand what you mean by "first pass through the liver."
You explain that:
So, your hypothesis predicts that switching from the oral tablets to the IV administration of AZT will reduce hepatotoxicity, since the liver is no longer exposed to a higher concentration of AZT than the rest of the organs.
It may have escaped your attention that a further prediction of your hypothesis is that switching to intravenous AZT will increase the toxic effects of AZT on all of the other organs except the liver, since the AZT is no longer being cleared by the liver in the portal circulation before reaching the peripheral circulation and having a chance to affect the rest of the organs.
So with respect to the clinical symptoms that Ariel Glaser was experiencing while receiving oral AZT, your hypothesis predicts that switching to intravenous AZT will improve them if they were due to the hepatotoxicity of AZT but will make them worse if they were due to a toxic effect on other organs (such as muscle).
The most dramatic change in Ariel's clinical state with intravenous AZT was the improvement in her weakness. This change can be consistent with your hypothesis only if her weakness was due to a toxic effect of AZT on the liver.
So, how does AZT toxicity cause weakness--by affecting the liver or by affecting some other organ?
It is well-documented that AZT toxicity causes muscle weakness by a direct effect on muscle. As you noted, AZT toxicity in the muscle is due to inhibition of a mitochondrial DNA polymerase, a toxicity often referred to as "AZT myopathy". The muscle weakness caused by AZT toxicity is associated with pathologic changes in the muscle--changes that can be observed in muscle tissue under a light or electron microscope. When muscle cells from patients with AZT myopathy are examined pathologically, they have abnormal-looking mitochondria (Dalakas MC et al (1990) N Engl J Med. 322:1098-1105). In this classic paper, the authors found that:
Furthermore, they reported that "repeat muscle biopsy from two patients in whom the myopathy responded to the discontinuation of zidovudine showed remarkable histologic improvement."
The weakness associated with AZT toxicity is due to a direct toxic effect of AZT on the mitochondria of muscle cells. Your hypothesis predicts that this non-hepatic toxicity of AZT should get worse after switching to round-the-clock IV administration of AZT, since muscle cells are now continuously exposed to a higher concentration of AZT than they were with the less efficient oral tablets.
The data disprove your hypothesis. However, they are consistent with the hypothesis that the weakness was due to the effect of HIV infection of the central nervous system (CNS). Because of the absence of first-pass clearance by the liver, intravenous administration of AZT is predicted to increase delivery of AZT to the CNS, thereby more efficaciously inhibiting viral replication in the CNS and improving the neurological symptoms caused by HIV infection of the brain and spinal cord.
Noble,
Project Day Lily was written by scientists that are far more accomplished than you. A Nobel Laurete gave it rave reviews. So I
will take their words over yours any day.
Have you recieved thousands of letters from people with CFS/gulf war syndrome thanking you for your research, like they have? Have you ever helped any sick people for that matter? The Nicolsons were not bought and paid for, and neither was Dr. shyh Ching Lo, And they used Kochs postulates to make you hiv fundamentalists look like fools.
Were the gulf war veterans lying when they said they were passing this illness on to their families?
I still have not received an answer from you people on this question, how does HIV, that only infects a small fraction of T cells cause organ failure?
I posted a response to Dr. Maniotis with some links which has been caught in the spam filter. But there are a few additional things that I'd like to point out now:
- If Dr. Maniotis actually reads the literature on the correlation between TLC & CD4 counts, he will see that he is wrong to state that "most if not all of the stats regarding correlations between CD4, total lymphocytes counts, and prediction to death from "AIDS" have been done on ARV drugged people".
This claim is as accurate as his previous claim that "Absolute counts reflect similar if not identical trends according to all the available studies that have compared the two (CD4 and absolute)." He has at least belatedly acknowledged that this latter claim is false.
- Dr. Maniotis says he consulted pathologists about total lymphocyte counts & PCP in children. I surely don't need to explain why pathologists are not the best source of information on surrogate markers of cellular immune deficiency in HIV-infected children.
- I'd been hoping to avoid doing so, but I looked at the coroners report, and the bloodwork Dr. Maniotis has been referring to throughout this thread was taken after the child in question had undergone three cardiac arrests and been resuscitated three times. In other words, Dr. Maniotis - apparently a serious scientist, with tenure, at a supposedly reputable institution - is attempting to draw parallels between blood values in the published literature on surrogate markers of immune deficiency and those taken from a child whose circulation had stopped and been restarted three times.
Eliza-Jane had a single blood count taken following acute cardiovascular collapse and cardiorespiratory arrest and repeated resuscitation attempts with fluids and drug therapy. She had an antecedent illness before her death that may well have been an acute viral infection (a very common cause of a raised TLCount). Peripheral blood lymphocyte counts are subject to large natural diurnal variation.
We will never know her CD4 count in "health", but it would be an extremely stupid clinician who would make dogmatic assertions about what EJ's usual lymphocyte count and CD4 count were like usually. Clinicians never place emphasis on single counts - they are always repeated to check the degree of concordance.
For Maniotis to use a one-off lymphocyte count in a critically ill child as his basis for claiming EJ could not be immunodeficient is totally ridiculous.
As for he idea that EJ had "late" amoxicillin allergy, don't make me laugh. She did NOT have a hemolytic anemia, did NOT have Stevens Johnson Syndrome and did NOT have exfoliative dermatitis, which you state are the classic features.
That's right, Mr. Jeffreys,
TL counts after 3 arrests is poor data at best-assuredly, but more trustworthy than Ribe's "resolution of the case." If she was an end stage AIDS case as the witch-hunters of the Majorie-Scovill family have doggedly advanced, where did the extra 5,000+ lymphocytes come from after her 3rd arrest? Like 18th century mice, from under blankets? I said above that in an acute late reaction, one hypothesis is that they may have been released (in a person with a normal immune system) in the peripheral vascular system due to the sudden toxic reaction from amoxicillin, or alternatively, the Total T-cell count (is it really affected by cardiac arrest Mr. Jeffreys???), was a result of a 2 week ear infection. I don't think the extra lymphocytes came from the long-term ravages of "HIV" "disease," do you, since end-stage AIDS is thought to be disease of too few, rather than too many lymphocytes, as in the case of Eliza Jane's admittedly belated, but hospital -recorded blood work shows. Unless lymphocytes can divide after a 3.5 year "HIV" infected, weight-gaining, clear-lunged, bright, energetic, and suddenly, organ-distended, vomiting, 36 hour-experienced B-lactam-dosed cardiac arrested child (given even more undisclosed antibiotics after her cardiac arrest(s)), then I suggest you consider the remote possibility that she died in the manner described almost exactly by amoxicillin package inserts I have posted the relevant parts from above.
It certainly couldn't hurt to apologize to the family! Who knows, they might someday forgive the pain you people put them through.
RE:
"I'd been hoping to avoid doing so, but I looked at the coroners report,"
You mean you and your people, who called for a Salem Witch Hunt to destroy this family never looked at the coroner's report for yourselves before now? I can't even hardly believe it! This is wrong! For shame, Mr.(Dr.) Jeffreys!!!
And you try to impeach my harping on this fact after checking the medical record (finally!!!!) yourself two years after the fact?
I've given you the reasons why I would trust the hospital count over any evidence submitted by Ribe:
As stated:
An autopsy was performed and "no cause of death" was found by the Los Angeles County coroner's office where her case had been referred. Approximately one week after the autopsy, the coroner's office learned of her parents' unorthodox views on HIV and AIDS and the testing history of the mother (inconclusive, positive, inconclusive, positive, negative, and positive). Rather than ordering a second analysis, another medical examiner (James K. Ribe) not originally assigned to the case was "brought in to help resolve the case," and revised autopsy findings were released claiming Eliza Jane died of "Pneumocystis carinii pneumonia" and "HIV encephalopathy."
How could the "no cause of death" was pronounced by the first coroners, and it somehow transformed miraculously into a death attributed to PCP pneumonia after Ribe was called in to "resolve" the case (after the coroner's office found out about Christine's book)? What's the matter? Were the first team of coroners incompetent, unwilling to change their report of undetermined or "no cause," or perhaps they didn't read Christine's book?
I don't really know, Mr. Jeffreys (I believe it is Dr. Jeffreys, is it not-I haven't looked up your credentials because I am not interested in your credentials-Adele's view and your view and Nobel's views are just as valuable in this case as anyone else's, as long as there is some semblance of logic and evidence. Perhaps I should look you up-I know there is a Jeffreys of some stature somewhere in the AIDS establishment as I have seen the name on papers.
Therefore, I'd trust a lymphocyte count after cardiac arrest (given that like mice, lymphocytes don't reproduce under blankets in anyone, especially "end-stage PCP patients because they, like lymphocytes come from pre-existing cells, over Ribe's "resolving" of the case after he changed the first coroner's reports.
http://www.justiceforej.com/ribeflipflops.html
Testimonial Flip Flops: A report on Los Angeles County Coroner Dr. James K. Ribe
Lewis Owen Amack, Esq.
California Bar No. 177774
"Everyone sees what you seem to be, but few discover what you are; and those few will not dare oppose the voice of the many who have the majesty of the prince on their side." From Niccolo Machiavelli's The Prince.
Los Angeles County Deputy Coroner James K. Ribe has a long, disturbing history of medical misjudgments and reversals of opinion that have subjected innocent people to miscarriages of justice, especially wrongful murder convictions. Because his tendentious testimony overwhelmingly favors the prosecution, however, he has been protected by the Los Angeles County District Attorney's Office, which has hidden Ribe's incompetence and bias from everyone, including defense attorneys and even deputy district attorneys.
Dr. Ribe admits that he reshapes his opinion over time-that is, his medical judgments evolve as he is presented with additional evidence before, during, and after trial. Thus, he has been known to change his opinion after his testimony and caused the conviction of innocent persons (see, e.g., the Wingfield-Helms case, infra), or when a metamorphosis in testimony is necessary to win a prosecution (see, e.g., the Rathbun-Sobek case, infra). Disturbingly, if not shockingly, Ribe apparently regards such intellectual ambivalence as progressive and laudatory. In actuality, Ribe's belated remolding of medical findings reflects a lack of objectivity and reliability. Post-autopsy changes in medical observations based upon evidence presented by third parties are very likely to be biased by the information presented by those third parties. As the examples below demonstrate, the transmutations in Ribe's forensic impressions tend to bend toward the will of the prosecution. Note that each of these examples is referenced from newspaper articles instead of legal citations because the D.A. and court system have been completely remiss in dealing with issues such as the Ribe problem, where the goal of the prosecution and its witnesses is simply to convict at any cost, irrespective of justice or the presumption of innocence.
Item 1: Rathbun-Sobek. Charles Rathbun, convicted of murdering model Linda Sobek, was nearly acquitted in his 1996 trial, because Ribe could not explain the cause of Sobek's death four months after he performed her autopsy. He eventually conceded that Sobek's asphyxiation was not accidental, thereby assuring a guilty verdict against Rathbun. During cross-examination, Ribe admitted that he revised his opinion based on the courtroom testimony of another prosecution witness. (Greg Krikorian, Sobek's Death Not an Accident, Deputy Coroner Testifies, LOS ANGELES TIMES, October 24, 1996, at p. 3.)
Item 2: Cauchi. Ribe changed his testimony in another 1996 trial, the prosecution by Deputy District Attorney Daniel Wright of Robert Cauchi of Van Nuys for the alleged torture and murder of his four-year-old stepdaughter. Because Wright knew of other cases where Ribe revamped his opinion during the course of a trial, he filed an internal memorandum to the District Attorney's Bureau of Special Operations alleging "serious errors" in Ribe's testimony and reliability. According to the memo, the prosecution was "almost derailed" by Ribe's "surprise reversal of opinion." (Greg Krikorian, Records on Deputy Coroner are Sought. Court: Judge's order could affect murder cases. District attorney's office repeatedly used official despite questions about his credibility, LOS ANGELES TIMES, November 22, 1997, at p. 1.)
Item 3: Arce/Urbano. During the 1997 trial of Edith Arce and Roy Urbano of Huntington Park for the alleged starving death of their three-year-old son prosecuted by Deputy District Attorney Dinko Bozanich, a sweeping order was issued by Norwalk Superior Court Judge Dewey L. Falcone demanding:
1. transcripts of all testimony by Ribe dating back to 1990,
2. copies of all coroner's reports relating to Ribe's testimony, and
3. all internal memoranda and complaints about Ribe's credibility.
Bozanich supported the order, because of his consternation that the district attorney's office does not share data about the unreliability of expert witnesses like Ribe with its own prosecutors. Bozanich lamented:
"How can I make an intelligent decision on how to prosecute a case when my own office has information that the credibility of a centerpiece witness may be so impaired that it may not only be worthless to put him on but damaging to the prosecution?"
Bozanich said that witnesses like Ribe expose him to "the risk of being blindsided" (Greg Krikorian, Courts: Judge gives office three more weeks to find data on deputy coroner whose credibility is questioned, LOS ANGELES TIMES, November 25, 1997, at p. 8.).
Item 4: Wingfield/Helms. Ribe's most notorious flip-flop may have occurred after the 1995 prosecution of Eve Wingfield and David Helms of North Hollywood for the murder of two-year-old Lance Helms. Initially, Ribe testified that Lance died thirty to sixty minutes after he was beaten when Ms. Wingfield was with the toddler. As a result, Ms. Wingfield, although innocent, made a plea bargain under duress, accepting a ten-year sentence for Lance's death. When two LAPD detectives who suspected that David Helms was the murderer interviewed Ribe years later, he told them that Lance died instantaneously, while he was under the control of David Helms. Ribe disavowed his earlier testimony as "just ridiculous," arguing "I had zero time to prepare." According to the defense attorney, Jack Stone, Ribe "tailor[s] his scientific opinion" to coincide with prosecution theories. Only after the fortuitous revelation of Ribe's change of mind was Wingfield released from prison, and David Helms finally convicted of murder. (Andrew Blankstein, Lawyer to Seek Release of Woman Imprisoned in Toddler's Death. Courts: New medical testimony suggests the boy's father, not she, was present when the 2-year-old was fatally beaten in 1995, LOS ANGELES TIMES, September 11, 1997, at p. 5; Andrew Blankstein, Woman to Be Freed in Toddler's Slaying. Court: Judge says new evidence indicates she may be innocent. Case sparked change in state law, LOS ANGELES TIMES, September 13, 1997, at p. 1; and Andrew Blankstein, Father Goes on Trial in Son's Slaying. Court: David Helms is accused of beating 2 1/2-year-old Lance. Coroner's testimony on time of death could be pivotal, LOS ANGELES TIMES, August 3, 1998, at p. 1.)
Item 5: Jacobo/Vildosola. Ribe's negligence-if not venality-was responsible for the 1997 wrongful murder convictions of William Jacobo, Jr. and Patricia Inez Vildosola of Monterey Park after the sudden death of their twenty-month-old baby Destiny. Ribe contended Destiny was the victim of "Shaken Baby Syndrome"-a controversial if not fallacious diagnosis based upon damage to and hemorrhaging of the brain. Yet Ribe did not provide crucial "contre-coup" brain matter to Los Angeles County's chief neuropathologist, Dr. Hideo H. Itabashi; nor did he present the brain tissue at trial. Evidently, Ribe destroyed or concealed the purported "contre-coup" material because it was exculpatory, and he wanted to ensure a successful prosecution. Ribe also withheld evidence that Destiny was suffering from pneumonia and other medical problems, and that she was fatally mistreated in the Emergency Room of Santa Marta Hospital by Joseph Boggs, a doctor with a suspended medical license whose licensesure was never reinstated. The principal cause of Destiny's death was pneumothorax, the consequence of overaggressive cardiopulmonary resuscitation by Boggs. Although Destiny was dying of acute respiratory distress syndrome caused by the pneumothorax, Boggs transferred Destiny out of Santa Marta to another hospital eighteen (18) miles away in order to hide his malpractice. Mr. Jacobo was exonerated and released after spending five long years in state penitentiaries, but Ms. Vildosola, who is equally innocent, remains incarcerated for life.
Items 1-5 above are presented as concise examples for illustrative purposes only, and should not be regarded as an exhaustive litany, or as a complete accounting of all instances of Dr. Ribe's forensic and testimonial unreliability.
The Appellate Court expressed its concern about Ribe's indecisiveness as follows:
"Had this Court been informed of [Coroner Ribe's] prior changes of opinion, it would have ordered additional disclosure if requested and allowed further defense inquiry on cross examination. Moreover, knowledge of the change of opinion would likely have led any defense counsel to have known to ask for more specific information, as opposed to a general, informal discovery letter on other Ribe cases. Such discovery might have shown such a pattern as has resulted in the so called 'Ribe box' of discovery, or additional, other, expert testimony." Salazar, 110 Cal.App.4th at 1634, 3 Cal.Rptr.3rd at 275.
Likewise, in the trial of Ms. Vildosola, if the prosecution had made information about Ribe's dubious credibility and forensic irresoluteness available to the court and defense attorneys, there is a strong likelihood that Patricia would have been properly exonerated of all charges.
The extent of Deputy Coroner Ribe's history of unreliability, vacillation, and bias may never be fully determined. (Jean Guccione, County Reviews Doctor's Trial Testimony. Reversals of verdicts prompt public defender to look at proceedings involving a deputy coroner known for changing his findings, LOS ANGELES TIMES, August 27, 2003, at p. B.4. See also Jean Guccione, Child-Murder Conviction Tossed. L.A. Coroner's Credibility Cited, LOS ANGELES TIMES, August 23, 2003, at p. B.1.)
Moreover, the district attorney's office continues to conceal information about Ribe's inconsistencies, and its lack of confidence in Ribe's credibility. (David Watson, Court Rules Withheld Evidence Requires Reversal in Child's Death, METROPOLITAN NEWS ENTERPRISE (Los Angeles, California), August 6, 2003, at p. 1)
All cases for which Ribe testified may be tainted, and should be reopened immediately by the Los Angeles County District Attorney's Office. (Katherine Gaidos, Ruling Bashes DA for Hiding Witness's Flaws, LOS ANGELES DAILY JOURNAL, August 25, 2003 Vol. 116, No. 164, at pp. 1ff.
Furthermore, a federal investigation may be needed in order to determine the extent and impact of Ribe's improprieties. (Jim Crogan, Web of Deceit: Murder conviction overturned because D.A. withheld evidence, LA WEEKLY, August 15-21, 2003)
http://www.justiceforej.com/ribeflipflops.html
And as both you and Adele have agreed, in the absence of any "HIV" test (PCR, ELISA, WB,even though none of these have been standardized and differ from place to place (test positive in Fiji and Fly to New Zealand and different standards hold-especially for the dead, and there is a substantial literature on "HIV" testing on cadavers, and they are unreliable), end stage AIDS is a disease of too few rather than too many lymphocytes.
Mr. Jeffreys,
I almost forgot:
RE:
"I surely don't need to explain why pathologists are not the best source of information on surrogate markers of cellular immune deficiency in HIV-infected children."
Sure you do need to explain it. Try explaining it to Redman, Burke, The Armed Forces Institute of Pathology, The American Red Cross, etc.
EG.
Burke DS, Brundage JF, Redfield RR, Damato JJ, Schable CA, Putman P, Visintine R, Kim HI, AIDS researchers (New England Journal of Med. 319, 961-964, 1988) reported that:
"...We studied the frequency of false positive diagnoses retrospectively among applicants seropositive for HIV in a subpopulation with a very low prevalence of infection... Approximately 1 percent of all initial screening ELISAs were reactive, 50 percent of repeat ELISAs were reactive, and 30 to 40 percent of first Western blot assays were reactive and diagnostic." (i.e., 60 to 70% of the twice positive ELISAS were false).
Or perhaps, since you don't think Pathologists aren't knowledgeable about diagnostics using surrogate markers, why don't you go ask the test-kit makers themselves:
Abbott's Axsym kit says on its label:
"At present there is no recognized standard for establishing the presence of absence of antibodies to HIV-1 and HIV-2 in human blood."
Abbott's 1997 Laboratory's ELISA test kit package insert says:
"ELISA testing alone cannot be used to diagnose AIDS." (Abbott 1997).
Epitope's 1997 (the maker for one of the Western Blot kits) package insert says:
"Do not use this kit as the sole basis for HIV infection." (Epitope 1997).
Roche's 1996 "Amplicor" test kit's insert states:
"The amplicor HIV-1 monitor test is not intended to be used as a screening test for HIV, nor as a diagnostic test to confirm the presence of HIV infection." (Roche 1996).
Then what the hell is it used for? Is it a lie detector?
Presumably, as grave as an "HIV" or "AIDS" diagnosis is, one might expect there should be awareness generated about the lack of a gold standard (virus isolation) disclosed to the public. Or one might minimally expect, if the test kits predict progression to an "AIDS-defining illness," at least one test kit type or brand available of the 31 on the market, that by itself, can serve as a gold standard to identify individuals who carry specific antibodies against the "HIV" virus, or components of the "HIV" virus itself.
Assuming that these conditional statements on the "HIV" test kits aren't typos, and are stated as they are by the manufacturers for a reason (if they were typos Abbott's should say "Elisa testing can be used alone to diagnose AIDS," Epitope's should read, "Use this kit as the sole basis for HIV infection," and Roche's should read, Amplicor HIV-1 monitor test can be used as a screening test for HIV, and as a diagnostic test to confirm the presence of HIV infection"), we must assume there is yet no gold standard for virus identification.
Obviously, these kinds of qualifications also present us with an intractable paradox regarding any recommendation that advocates universal testing, or believing recommendations from studies which identify cohorts in clinical trails on the basis of these tests (or statistical procedures based on antibody tests. Nor will the proliferation of recent rapid test kits that claim to have been validated by comparing positive or negative (or indeterminate) outcomes against the more widely used and non-validated test kits such as Abbott's, Epitope's, or Roche's increase the certainty of "HIV" diagnosis, if, or until, a gold standard is developed against which all kit results can be validated, which is virus isolation itself.
The new "rapid" "HIV" tests which claim near 100% accuracy and specificity are considered even by the Federal Trade Commision to be fraudulent.
But if the standard tests (and they don't specify what "the standard tests" are) say they cannot be used to detect "HIV" or "AIDS" as their inserts claim, then how is it possible that a rapid test based on these standard test results can? Apparently the answer to this question was advanced in 2004 in an article entitled, "AIDS Home Test Kit Called Deceptive, (John Bulloch, Wall Street Journal, June 9th, 2004):
"A District Court in Seattle has granted a request from the Federal Trade Commission and issued a temporary restraining order to prevent the sale and distribution of "defective" home HIV test kits. According to FTC, the kits' maker, Seville Marketing of British Columbia, Canada, on two Web sites had advertised the "Discreet" home HIV test kits as producing 99.4% accurate results based on three independent studies. However, CDC studied the test kits and found they were not as accurate as the company claimed on its Web site."
"Three minutes after performing the test according to the package instructions, 15.4% of the results were inaccurate; after eight minutes, 29.6% of the results were inaccurate; and 59.3% of the tests produced inaccurate results after 15 minutes. The kits gave both false-positive and false-negative results, according to the release. The kits, which cost $29.95, have been available on the Web through the company's Internet sites. FTC noted in its complaint that the kits cannot be sold legally in the United States because they are not approved by FDA as a diagnostic tool, according to the release."
"FTC will seek a permanent ban on sales and advertising of the kits in the United States and a permanent order to seize any kits that are imported. Consumers who have used the kits are advised to see a health professional for another test to determine their HIV status, according to the release."
Some other test kits have the following qualifications:
NucliSens(R) HIV-1 QT -- HIV QT Nov. 13, 2001 (http://www.fda.gov/cber/pma/p0100010.htm
http://www.fda.gov/cber/pmalabel/P0100010LB.pdf):
"The NucliSens(R) HIV-1 QT assay is not intended to be used as a screening test for HIV-1 nor is it to be used as a diagnostic test to confirm the presence of HIV-1 infection."
COBAS AmpliScreen HIV-1 Test, version 1.5
Approval Date: 12/19/2003 (http://www.fda.gov/cber/products/hiv1roc121903.htm
http://www.fda.gov/cber/label/hiv1roc121903LB.pdf):
"This test is not intended for use as an aid in diagnosis."
Procleix(R) HIV-1/HCV Assay -- IN0076-01, Rev. A
Approval Date: 6/4/2004 (http://www.fda.gov/cber/products/hivhcvgen060404.htm
http://www.fda.gov/cber/label/hivhcvgen060404LB.pdf):
"The Procleix HIV-1 Discriminatory Assay may be used as an aid in the diagnosis of HIV-1 infection."
GENETIC SYSTEMS (TM) rLAV EIA (http://www.fda.gov/cber/products/hiv1gen062998.htm
http://www.fda.gov/cber/sba/hiv1gen062998S.pdf):
"The rLAV EIA is intended to be used as a screening test for donated blood or plasma and as an aid in the diagnosis of infection with HIV-1."
VIRONOSTIKAT(R) HIV-1 PLUS O MICROELISA SYSTEM (http://www.fda.gov/cber/pma/P020066.htm
http://www.fda.gov/cber/pmalabel/P020066LB.pdf):
"System is intended for use as an aid in diagnosis of infection with HIV-1. It is not intended for use in screening blood donors."
THE CAMBRIDGE BIOTECH HIV-1 WESTERN BLOT KIT (http://www.fda.gov/cber/products/hiv1cam052898.htm
http://www.fda.gov/cber/label/hiv1cam052898Lb.pdf):
"Accurate diagnosis of HIV-1 infection is important in determining an individual's risk for developing AIDS. Accuracy is complicated by false-positive and false-negative (EIA) results. It would appear that in some limited infections, a compartmentalized response occurs in which expression of HIV-1 or its respective Immune response is limited to a restricted number of organs and tissues.(17)"
"Although a blot POSITIVE for antibodies to HIV-1 indicates infection with the virus...a POSITIVE blot results using any specimen type (serum, plasma, or urine) should be followed with additional testing. Such testing may rely on alternative test methods or specimen types."
This is one I really like that ends this paragraph:
"The clinical implications of antibodies to HIV-1 in an asymptomatic person are not known."
OraSure(R) HIV-1 Western Blot Kit (http://www.fda.gov/cber/pma/P950004.htm
http://www.fda.gov/cber/pmalabel/P950004Lb.pdf ):
AND:
The OraSure HIV-l Western Blot Kit is not intended for use with blood, serum/plasma or urine specimens, or for screening or reinstating potential blood donors."
Regarding nucleic "HIV" tests that claim to specifically detect "HIV" nucleic acids, it is well known that the amplification of a nucleic acid moiety with PCR also cannot be used quantify the true number of nucleic acid copies of the "HIV" genome, since none of the current nucleic acid tests have been standardized and validated against "HIV" isolation (indeed some of these ultra-sensitive tests have detected "HIV" infection at titers of virus BELOW that which is theoretically possible to detect by a particular test kit (i.e below 50 copies/ml-see the CDC's MMWR 316, 2001 50, RR20). Apparently, this view is widely appreciated by many "HIV/AIDS" researchers and doctors who have done the most "HIV" nucleic acid testing themselves:
Defer et al. in a paper entitled, "Multicentre quality control of polymerase chain reaction [viral load] for detection of HIV DNA" (AIDS 6: 659-663, 1992), reported that:
"False-positive and false-negative results were observed in all laboratories (concordance with serology ranged from 40 to 100%").
Busch et al., in a paper entitled, "Poor sensitivity, specificity, and reproducibility of detection of HIV-1 DNA in serum by polymerase chain reaction. (The Transfusion Safety Study Group. J Acquir Immune Defic Syndr; 5 (9):872, 1992), reported that:
PCR-DNA tests on 151 ELISA-negative people found that 18.5% (28 people) had positive PCRs. Furthurmore, only 25.5% of people diagnosed HIV-positive had positive PCR's.
In their conclusion section they draw attention to how close the two numbers, 18.5% and 25.5%:
"This study of PCR detection of HIV-DNA in serum identified a disturbingly high rate of nonspecific positivity with a widely employed gag primer pair system [gag is a protein considered to be specific to HIV]. In fact, the overall positivity was not significantly different for serum specimens from seropositive patients and seronegative control donors (25.5% vs 18.5%). ... In contrast to the high rate of false positive results observed with gag primers, env DNA [env is another protein thought to be specific to HIV] was not detected by laboratory B in any of the specimens from either seronegative or seropositive individuals. Absence of reactions with both primer pairs from all 59 specimens from seropositive persons meant that no serum sample could be confirmed positive for HIV-DNA, i.e. 0% sensitivity. This finding is in marked contrast to the high sensitivity reported previously by Laboratory B for both gag and env primers." (Busch et al. 1992, pages 874-875)."
But these aren't pathologists, so you can trust em. However, our molecular pathologists here would agree with all of these statements.
Viral load does not correlate with T-cell numbers, and progression of disease can only be predicted in 4%-6% of any HIV-positives studied (out of 2,800):
A nationwide team of orthodox AIDS researchers led by doctors Benigno Rodriguez and Michael Lederman of Case Western Reserve University in Cleveland are disputing the value of viral load tests-a standard used since 1996 to assess health, predict progression to disease, and grant approval to new AIDS drugs after their study of 2,800 HIV positives concluded viral load measures failed in more than 90% of cases to predict or explain immune status...""Viral load is only able to predict progression to disease in 4% to 6% of HIV-positives studied, challenging much of the basis for current AIDS science and treatment policy" [] Rodriquez B, Sethi AK, Cheruvu VK, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA 296(12):1498-506, 2006; Cohen J. Study says HIV blood levels don't predict immune decline. Science 313(5795):1868, 2006].
My favoritest of all:
The Red Cross recently reported that even after repeated testing using different test kits, low-risk populations, such as blood donors (or military recruits) will typically yield 12 (PCR-positive) or 2 (ELISA positive) out of 37,000,000 samples, leaving potentially 10 out of 12 false positives, depending on which test kit you believe [Stramer et al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing. New England Journal of Medicine, Volume 351:760-768, August 19, Number 8, 2004].
franklin said: So, your hypothesis predicts that switching from the oral tablets to the IV administration of AZT will reduce hepatotoxicity, since the liver is no longer exposed to a higher concentration of AZT than the rest of the organs.
correct
It may have escaped your attention that a further prediction of your hypothesis is that switching to intravenous AZT will increase the toxic effects of AZT on all of the other organs except the liver, since the AZT is no longer being cleared by the liver in the portal circulation before reaching the peripheral circulation and having a chance to affect the rest of the organs.
No it did not escape my attention, and yes you are correct, systemic toxicity continued after a short period of temporary clinical improvement.
So with respect to the clinical symptoms that Ariel Glaser was experiencing while receiving oral AZT, your hypothesis predicts that switching to intravenous AZT will improve them if they were due to the hepatotoxicity of AZT but will make them worse if they were due to a toxic effect on other organs (such as muscle).
Wrong, the hypothesis only predicts a temporary clinical improvement when discontinuing liver first pass oral administration. This temporary improvement is from the reduced hepatotoxicity and relative improvement in liver function.
The most dramatic change in Ariel's clinical state with intravenous AZT was the improvement in her weakness. This change can be consistent with your hypothesis only if her weakness was due to a toxic effect of AZT on the liver. So, how does AZT toxicity cause weakness--by affecting the liver or by affecting some other organ?
Wrong again . Liver toxicity, and liver dysfunction produces clinical symptoms of weakness and fatigue as any nursing student who has cared for patients with liver disease (hepatitis, cirrhosis, metastatic disease to liver etc) will inform you. Improved liver function will relieve the weakness and fatigue temporarily. As you say, direct AZT muscle and brain toxicity will unfortunately continue and cause death, as it did in this case.
It is well-documented that AZT toxicity causes muscle weakness by a direct effect on muscle. As you noted, AZT toxicity in the muscle is due to inhibition of a mitochondrial DNA polymerase, a toxicity often referred to as "AZT myopathy". The muscle weakness caused by AZT toxicity is associated with pathologic changes in the muscle--changes that can be observed in muscle tissue under a light or electron microscope. When muscle cells from patients with AZT myopathy are examined pathologically, they have abnormal-looking mitochondria (Dalakas MC et al (1990) N Engl J Med. 322:1098-1105). In this classic paper, the authors found that: "Numerous "ragged-red" fibers, indicative of abnormal mitochondria with paracrystalline inclusions, were found in the biopsy specimens from the zidovudine-treated patients but not in those from the other patients. The number of these fibers appeared to correlate with the severity of the myopathy." Furthermore, they reported that "repeat muscle biopsy from two patients in whom the myopathy responded to the discontinuation of zidovudine showed remarkable histologic improvement." The weakness associated with AZT toxicity is due to a direct toxic effect of AZT on the mitochondria of muscle cells. Your hypothesis predicts that this non-hepatic toxicity of AZT should get worse after switching to round-the-clock IV administration of AZT, since muscle cells are now continuously exposed to a higher concentration of AZT than they were with the less efficient oral tablets.
The systemic toxicity did get worse, and it eventually, tragically, killed the unfortunate child. Bone marrow suppression is a result of systemic AZT toxicity, and this was described in the narrative shortly before her death. AZT is directly toxic to mitochondria in all cells of the body. Both Elizabeth and Ariel succumbed to AZT mitochondrial toxicity.
The data disprove your hypothesis. However, they are consistent with the hypothesis that the weakness was due to the effect of HIV infection of the central nervous system (CNS). Because of the absence of first-pass clearance by the liver, intravenous administration of AZT is predicted to increase delivery of AZT to the CNS, thereby more efficaciously inhibiting viral replication in the CNS and improving the neurological symptoms caused by HIV infection of the brain and spinal cord
franklin, even a first year nursing student with rudimentary knowldge would reject your qbove unsubstntiated claim that Ariel had viral encephalitis. There was no CSF report available to indicate viral encephalitis. And even if there was, AZT is a pitiful treatment for it.
Ariel's CNS symptoms were obviously due to AZT CNS toxicity. If AZT is such a great drug, Ariel's temporary clinical improvement after switching from oral to IV administration should have continued with complete clinical recovery.
It obviously did not, and instead killed the poor girl with systemic AZT toxicity. This is as plain as day to everyone by now. The only people still clinging to your irrational belief in the healing powers of AZT, the greatest poison ever created by humankind, are the drug company shills and paid political activists (are you one of these?).
By now this information is out in the open and everyone knows about it. The old days are over and gone. We can't bring back Ariel and Elizabeth, but we can speak truthfully and warn others not to misplace their trust in medical institutions that will betray them with deadly drugs.
For more information see, www.reviewingaids DOT com
Regarding the EJ case, a few comments.
Number one, EJ's blood and CSF cultures showed no growth. If EJ had terminal AIDS, she should have had opportunistic infection in her blood and/or CSF. There wasn't any. She didn't have AIDS. The second coroner cooked the books as he had a history of doing with many other cases. He was a crooked coroner, that is clear from his history.
Number Two, there was fluid in the pericardium indicating EJ's cardiac arrest and death was from pericardial tamponade, acute fluid collection in the pericardium. Acute pericardial fluid, like the more commonly seen example of laryngeal edema is an allergic drug reaction, not an opportunistic infection. Acute edema, i.e. fluid collecting in spaces where it doesn't belong is a drug reaction, not an opportunistic infection. Allergic Reaction with acute pericardial tamponade was the probable cause of death.
It's time to let this matter rest and respect the family. EJ's mother doesn't have AIDS, and neither did the child.
Dr. Maniotis, you are asserting that your interpretation of these total lymphocyte values is more trustworthy than the LA coroner's report. This is a ridiculous assertion, and given the level of trustworthiness you have displayed in this one thread, a completely unconvincing one.
EJ did not have "end stage AIDS," she died, according to the coroner's report, of her first bout of PCP. The literature is absolutely clear that PCP is one of the first opportunistic infections people become at risk for. The literature also makes it clear that acute respiratory failure due to PCP is one of the most common causes of PICU admission for HIV-infected children. It seems no one has any idea what EJ's CD4% was, or any idea how many CD8 T cells, NK cells, B cells, NKT cells and gamma/delta T cells she had.
Given these facts, your apparent attempt at sarcastic humor regarding lymphocytes coming out of blankets is as ignorant as it is offensive. The blood represents no more than 1-2% of the total body lymphocyte pool. And if you were familiar with the literature on the immunology of HIV infection you'd also know that a substantial contribution to the decline in peripheral blood CD4 T cell counts comes from redistribution of cells to the lymphoid tissue. As I mentioned in the post that has yet to appear, immunology has progressed a little further than counting lymphocytes and if you want to try and adhere to your simple formulation then you could correctly say that AIDS is a disease of too few lymphocytes that work and too many that don't.
I am not claiming to know with any certainty whether EJ was HIV-infected - how can I? - all I can say is that based on the literature and an exchange with James Oleske I can see no reason to question the cause of death as reported by the coroner. Your attempts to explain that report away have consisted of lies and ghoulish handwaving. Like Duesberg, it seems you have decided that tenure is a license to lie about the published work of other scientists; I think you're a disgrace to your profession.
As long as there no positive HIV test, or cd4 count than this all seems pretty political to me. With no ill health, wasting, normal WBC's and the suddenly she "broke out" with hiv dememtia.............sounds much more like a allergic reaction.
I have learned alot from Dr. Mantious posts, especially the ones describing the horrible reactions to gardisil, AZT's toxicity and am glad to see a very good scientist stand up agaisnt the medical industry complex.
The things he and many other scientists are saying about mercury/vaccines and AZT deserve public scrutiny. Why don't mainstream scientists just debate these people and conduct a poll of the audience to see who wins?
They will never debate publicly because they are scared.
Project Day Lily was written by scientists that are far more accomplished than you. A Nobel Laurete gave it rave reviews. So I will take their words over yours any day.
You seem to be having major problems distinguishing fiction from reality. "Project Day Lily" is a work of fiction. It reads like the script of a B grade movie.
I still have not received an answer from you people on this question, how does HIV, that only infects a small fraction of T cells cause organ failure?
That's an ironic choice of a Denialist canard to play with.
How does a mycoplasma that doesnt infect PBMCs cause the depletion of CD4+ cells?
No evidence of mycoplasmas in peripheral blood mononuclear cell fraction of HIV-infected patients.
No mycoplasmas found in the PBMCs but they did find HIV!
It's time to let this matter rest and respect the family.
Isn't that ironic. It was Andrew Maniotis that hijacked this thread and turned it from a thread about smallpox to one about EJ Scovill and AIDS.
This is how Adele responded.
Andrew, let me suggest you leave the Maggiore issue alone. This is the third or fourth time I've said it on here, it's YOU and other denialists who ALWAYS bring up EJ. ANd then people respond with facts and you accuse them of victimizing someone.
Its a fictionalized version of true events based on confidential sources he had in the Pentagon according to him. They were respected scientists, and I doubt they would lie, but the again you would probably deny the Tuskegee expirement while it was occuring.
The earned a tremendous amount of respect in the Department of defense and were made honorary Navy Seals, because they helped thousands recover their health from the mysterious "gulf war syndrome"
I never said mycoplasmas cause AIDS in all patients, I Just it can complicate it in some patients. I agree with what DR. Lo said in 1990 that "Aids is much more complicated than hiv" More experiments need to conducted.
Again you couldn't answer the question about hiv and organ failure, so you attacked a position that I didnt even have to create a distraction. Nice one.
Richard Jefferys and his pharmaceutical corporate sponsors have made repeated ad hominem attacks on Andrew Maniotis which are disgusting and repulsive.
Jefferys is a typical paid political activist, with no understanding of science or the medical literature. In other words, he is a hack paid by drug money to make ad hominem attacks. His words are lies and distortions and he cannot be trusted.
Notice how he has not addressed a single issue raised by Dr Maniotis except to play phoney tricks. The reason for this is that Jefferys cannot even understand how to begin to read Andy's comments.
Go peddle your death drugs elsewhere, Mr. Jefferys. You belong in South Africa leading a band of loyal paid protestors with garlic and lemon in hand organized by drug company money. You are the disgrace to the human race, you arrogant pompous ignorant repulsive small man. A simple google seach on his name will reveal all you need to know about him.
Its a fictionalized version of true events based on confidential sources he had in the Pentagon according to him.
My confidential source in the Pentagon tells me that George Bush is really a shape-shifting reptiloid.
I never said mycoplasmas cause AIDS in all patients, I Just it can complicate it in some patients. I agree with what DR. Lo said in 1990 that "Aids is much more complicated than hiv" More experiments need to conducted.
You previously claimed that mycoplasmas fulfil Koch's postulates. Now you say mycoplasmas just complicate AIDS in some patients. You appear to be very, very confused.
Again you couldn't answer the question about hiv and organ failure, so you attacked a position that I didnt even have to create a distraction. Nice one.
Whoever claimed that all cases of organ failure in AIDS were caused directly by HIV? Many cases of organ failure are caused by opportunistic infections that arise after the immune suppresion caused by HIV. Hepatitis C is a cause of a large proportion of liver failure in patients with AIDS. As people with AIDS live longer and longer drug toxicity also plays a role.
They do folfill kochs postulates, so for those that test positive it will cause illnesses like CFS, fibromyalgia and if you Have Aids it will complicate it.
Jefferys is a typical paid political activist, with no understanding of science or the medical literature. In other words, he is a hack paid by drug money to make ad hominem attacks. His words are lies and distortions and he cannot be trusted.
That one broke my irony-meter.
Andrew,
Several times in this thread you have claimed that an autopsy was performed on Eliza Jane Scovill and found "no cause of death". For example you stated:
On what basis do you make this claim? I notice that by using quotation marks you indicate that the phrase "no cause of death" is a direct quote, apparently from the Los Angeles County Coroner's Office. Have you ever seen an autopsy report from the Los Angeles County Coroner's Office which states that "no cause of death" was found for Eliza Jane Scovill? Pardon my skepticism, but you already have a history of making up or misattributing quotes in earlier posts on this thread.
Let's see if I understand your claim. EJ died on 5/16/2005, and her autopsy (Case # 2005-03767) was performed on 5/18/2005. In the course of EJ's autopsy, the Medical Examiner performed an external examination, radiological studies, a gross dissection of all the major organs, and collected samples for microscopic studies, microbiological cultures, neuropathological studies, and toxicology.
Are you claiming that all of these studies were completed and a report was issued stating that "no cause of death" was identified, all in less than a week? As a "Professor of Pathology," is your usual experience that an autopsy of this complexity is usually completed in less than a week? Oh, I forgot, you've never actually performed an autopsy because you aren't a Pathologist.
If that is your claim and if your claim is true, why haven't EJ's parents posted the original report on their web page, for all the world to see?
Well, I think you and I both know that the reason her parents have not produced such a report is most likely that no such report exists. Most Pathology departments will save an autopsy brain in formaldehyde for at least a week (often longer) to assure proper fixation before slicing the brain to search for internal abnormalities. According to EJ's autopsy report (page 12), the gross examination of her fixed brain wasn't performed until June 22, 2005, and that doesn't include the microscopic analysis of the brain sections. How could the Coroner have issued a report stating "no cause of death" less than a week after the autopsy, if the gross examination of the brain wasn't performed until more than a month after the autopsy?
Likewise, page 19 of the autopsy report indicates that the toxicology analysis was not completed until June 22, 2005, also long after you claim the Coroner issued a determination that "no cause of death" was found. How do you think the Coroner could determine "no cause of death" without toxicolgy studies?
Andrew, how do you explain this discrepancy. All of these studies take time, and they would all need to be completed before the Coroner could conclude that "no cause of death" was found. As far as I can tell, the only results that might have been available within a week of the autopsy were the gross examination of the organs (except the brain) and the X-Rays of the body, neither of which would have allowed a determination of the cause of death in this case. A pathologic diagnosis of Pneumocystis pneumonia and of AIDS simply cannot be made solely on the basis of gross examination of the organs and skeletal X-Rays, the only results that might have been available in the time frame you claim. If such a report was issued less than a week after performing the autopsy, the most it could report is that:
Based soley on gross examination of the organs and X-Rays of the skeletal system, no cause of death is identified, but additonal studies including microscopic analysis, neuropathologic analysis, toxicologic analysis, and microbiologic analysis are pending.
Maybe the report says something like that? Please identify the source of your "quote." Who reported that "no cause of death" was found in EJ's auopsy--and on what basis did they make this determination?
They do folfill kochs postulates, so for those that test positive it will cause illnesses like CFS, fibromyalgia and if you Have Aids it will complicate it.
Mycoplasmas are only found in a small percentage of people with CFS. They are also found in a comparable percentage of healthy people. Clearly Koch's postulates are not fulfilled.
That mycoplasmas may well be a complication of AIDS is hardly surprising. There are many other pathogens such as tuberculosis and Hep C that complicate HIV/AIDS.
No, Lo's studies clearly show that healthy controls dont test positive for his novel strain. Its intersting because hiv, hpv, hepatitis c dont have animal models so you dont know what your talking about, it's not wise to bring up Kochs postulates when the microbes that you and the drug companies that own you push on the public failed Koch's postulates from day one.
Garth nicolson found mycoplasmas in about 60% of cfs patients, much like if 10 people had a fever 6 of those people tested positive influenza, and with 4 it will be an allergic reaction, just because the symptoms are similar doesnt mean the cause of the disease is the same.
As far as asymptomatic people testing positive, most every person who tests hiv positive is symptom free. Another part of koch's postulates is having the microbe being present in quantities sufficient to cause disease, that fool Robert Gallo said in his book that Hiv was only in 1 out 10,000 t cells, how the hell does it destroy the immune system when its totally nuetralized by antibodies and barely present and doesnt cause disease when injected to pretty much every species of animal?
Mr. Jeffreys,
I almost forgot:
RE:
"I surely don't need to explain why pathologists are not the best source of information on surrogate markers of cellular immune deficiency in HIV-infected children."
Sure you do need to explain it. Try beginning with Redman, Burke, The Armed Forces Institute of Pathology, The American Red Cross, etc.
EG.
Burke DS, Brundage JF, Redfield RR, Damato JJ, Schable CA, Putman P, Visintine R, Kim HI, AIDS researchers (New England Journal of Med. 319, 961-964, 1988) reported that:
"...We studied the frequency of false positive diagnoses retrospectively among applicants seropositive for HIV in a subpopulation with a very low prevalence of infection... Approximately 1 percent of all initial screening ELISAs were reactive, 50 percent of repeat ELISAs were reactive, and 30 to 40 percent of first Western blot assays were reactive and diagnostic." (i.e., 60 to 70% of the twice positive ELISAS were false).
Or perhaps, since Pathologists haven't contributed a plumb-nickel to the world, why don't you go ask the test-kit makers themselves:
Abbott's Axsym kit says on its label:
"At present there is no recognized standard for establishing the presence of absence of antibodies to HIV-1 and HIV-2 in human blood."
Abbott's 1997 Laboratory's ELISA test kit package insert says:
"ELISA testing alone cannot be used to diagnose AIDS." (Abbott 1997).
Epitope's 1997 (the maker for one of the Western Blot kits) package insert says:
"Do not use this kit as the sole basis for HIV infection." (Epitope 1997).
Roche's 1996 "Amplicor" test kit's insert states:
"The amplicor HIV-1 monitor test is not intended to be used as a screening test for HIV, nor as a diagnostic test to confirm the presence of HIV infection." (Roche 1996).
Then what the hell is it used for? Is it a lie detector?
Presumably, as grave as an "HIV" or "AIDS" diagnosis is, one might expect there should be awareness generated about the lack of a gold standard (virus isolation) disclosed to the public. Or one might minimally expect, if the test kits predict progression to an "AIDS-defining illness," at least one test kit type or brand available of the 31 on the market, that by itself, can serve as a gold standard to identify individuals who carry specific antibodies against the "HIV" virus, or components of the "HIV" virus itself.
Assuming that these conditional statements on the "HIV" test kits aren't typos, and are stated as they are by the manufacturers for a reason (if they were typos Abbott's should say "Elisa testing can be used alone to diagnose AIDS," Epitope's should read, "Use this kit as the sole basis for HIV infection," and Roche's should read, Amplicor HIV-1 monitor test can be used as a screening test for HIV, and as a diagnostic test to confirm the presence of HIV infection"), we must assume there is yet no gold standard for virus identification.
Obviously, these kinds of qualifications also present us with an intractable paradox regarding any recommendation that advocates universal testing, or believing recommendations from studies which identify cohorts in clinical trails on the basis of these tests (or statistical procedures based on antibody tests. Nor will the proliferation of recent rapid test kits that claim to have been validated by comparing positive or negative (or indeterminate) outcomes against the more widely used and non-validated test kits such as Abbott's, Epitope's, or Roche's increase the certainty of "HIV" diagnosis, if, or until, a gold standard is developed against which all kit results can be validated, which is virus isolation itself.
The new "rapid" "HIV" tests which claim near 100% accuracy and specificity are considered even by the Federal Trade Commision to be fraudulent.
But if the standard tests (and they don't specify what "the standard tests" are) say they cannot be used to detect "HIV" or "AIDS" as their inserts claim, then how is it possible that a rapid test based on these standard test results can? Apparently the answer to this question was advanced in 2004 in an article entitled, "AIDS Home Test Kit Called Deceptive, (John Bulloch, Wall Street Journal, June 9th, 2004):
"A District Court in Seattle has granted a request from the Federal Trade Commission and issued a temporary restraining order to prevent the sale and distribution of "defective" home HIV test kits. According to FTC, the kits' maker, Seville Marketing of British Columbia, Canada, on two Web sites had advertised the "Discreet" home HIV test kits as producing 99.4% accurate results based on three independent studies. However, CDC studied the test kits and found they were not as accurate as the company claimed on its Web site."
"Three minutes after performing the test according to the package instructions, 15.4% of the results were inaccurate; after eight minutes, 29.6% of the results were inaccurate; and 59.3% of the tests produced inaccurate results after 15 minutes. The kits gave both false-positive and false-negative results, according to the release. The kits, which cost $29.95, have been available on the Web through the company's Internet sites. FTC noted in its complaint that the kits cannot be sold legally in the United States because they are not approved by FDA as a diagnostic tool, according to the release."
"FTC will seek a permanent ban on sales and advertising of the kits in the United States and a permanent order to seize any kits that are imported. Consumers who have used the kits are advised to see a health professional for another test to determine their HIV status, according to the release."
Some other test kits have the following qualifications:
NucliSens(R) HIV-1 QT -- HIV QT Nov. 13, 2001 (http://www.fda.gov/cber/pma/p0100010.htm
http://www.fda.gov/cber/pmalabel/P0100010LB.pdf):
"The NucliSens(R) HIV-1 QT assay is not intended to be used as a screening test for HIV-1 nor is it to be used as a diagnostic test to confirm the presence of HIV-1 infection."
COBAS AmpliScreen HIV-1 Test, version 1.5
Approval Date: 12/19/2003 (http://www.fda.gov/cber/products/hiv1roc121903.htm
http://www.fda.gov/cber/label/hiv1roc121903LB.pdf):
"This test is not intended for use as an aid in diagnosis."
Procleix(R) HIV-1/HCV Assay -- IN0076-01, Rev. A
Approval Date: 6/4/2004 (http://www.fda.gov/cber/products/hivhcvgen060404.htm
http://www.fda.gov/cber/label/hivhcvgen060404LB.pdf):
"The Procleix HIV-1 Discriminatory Assay may be used as an aid in the diagnosis of HIV-1 infection."
GENETIC SYSTEMS (TM) rLAV EIA (http://www.fda.gov/cber/products/hiv1gen062998.htm
http://www.fda.gov/cber/sba/hiv1gen062998S.pdf):
"The rLAV EIA is intended to be used as a screening test for donated blood or plasma and as an aid in the diagnosis of infection with HIV-1."
VIRONOSTIKAT(R) HIV-1 PLUS O MICROELISA SYSTEM (http://www.fda.gov/cber/pma/P020066.htm
http://www.fda.gov/cber/pmalabel/P020066LB.pdf):
"System is intended for use as an aid in diagnosis of infection with HIV-1. It is not intended for use in screening blood donors."
THE CAMBRIDGE BIOTECH HIV-1 WESTERN BLOT KIT (http://www.fda.gov/cber/products/hiv1cam052898.htm
http://www.fda.gov/cber/label/hiv1cam052898Lb.pdf):
"Accurate diagnosis of HIV-1 infection is important in determining an individual's risk for developing AIDS. Accuracy is complicated by false-positive and false-negative (EIA) results. It would appear that in some limited infections, a compartmentalized response occurs in which expression of HIV-1 or its respective Immune response is limited to a restricted number of organs and tissues.(17)"
"Although a blot POSITIVE for antibodies to HIV-1 indicates infection with the virus...a POSITIVE blot results using any specimen type (serum, plasma, or urine) should be followed with additional testing. Such testing may rely on alternative test methods or specimen types."
This is one I really like that ends this paragraph:
"The clinical implications of antibodies to HIV-1 in an asymptomatic person are not known."
OraSure(R) HIV-1 Western Blot Kit (http://www.fda.gov/cber/pma/P950004.htm
http://www.fda.gov/cber/pmalabel/P950004Lb.pdf ):
AND:
The OraSure HIV-l Western Blot Kit is not intended for use with blood, serum/plasma or urine specimens, or for screening or reinstating potential blood donors."
Regarding nucleic "HIV" tests that claim to specifically detect "HIV" nucleic acids, it is well known that the amplification of a nucleic acid moiety with PCR also cannot be used quantify the true number of nucleic acid copies of the "HIV" genome, since none of the current nucleic acid tests have been standardized and validated against "HIV" isolation (indeed some of these ultra-sensitive tests have detected "HIV" infection at titers of virus BELOW that which is theoretically possible to detect by a particular test kit (i.e below 50 copies/ml-see the CDC's MMWR 316, 2001 50, RR20). Apparently, this view is widely appreciated by many "HIV/AIDS" researchers and doctors who have done the most "HIV" nucleic acid testing themselves:
Defer et al. in a paper entitled, "Multicentre quality control of polymerase chain reaction [viral load] for detection of HIV DNA" (AIDS 6: 659-663, 1992), reported that:
"False-positive and false-negative results were observed in all laboratories (concordance with serology ranged from 40 to 100%").
Busch et al., in a paper entitled, "Poor sensitivity, specificity, and reproducibility of detection of HIV-1 DNA in serum by polymerase chain reaction. (The Transfusion Safety Study Group. J Acquir Immune Defic Syndr; 5 (9):872, 1992), reported that:
PCR-DNA tests on 151 ELISA-negative people found that 18.5% (28 people) had positive PCRs. Furthurmore, only 25.5% of people diagnosed HIV-positive had positive PCR's.
In their conclusion section they draw attention to how close the two numbers, 18.5% and 25.5%:
"This study of PCR detection of HIV-DNA in serum identified a disturbingly high rate of nonspecific positivity with a widely employed gag primer pair system [gag is a protein considered to be specific to HIV]. In fact, the overall positivity was not significantly different for serum specimens from seropositive patients and seronegative control donors (25.5% vs 18.5%). ... In contrast to the high rate of false positive results observed with gag primers, env DNA [env is another protein thought to be specific to HIV] was not detected by laboratory B in any of the specimens from either seronegative or seropositive individuals. Absence of reactions with both primer pairs from all 59 specimens from seropositive persons meant that no serum sample could be confirmed positive for HIV-DNA, i.e. 0% sensitivity. This finding is in marked contrast to the high sensitivity reported previously by Laboratory B for both gag and env primers." (Busch et al. 1992, pages 874-875)."
But these aren't pathologists, so you can trust em. However, our molecular pathologists here would agree with all of these statements.
Viral load does not correlate with T-cell numbers, and progression of disease can only be predicted in 4%-6% of any HIV-positives studied (out of 2,800):
A nationwide team of orthodox AIDS researchers led by doctors Benigno Rodriguez and Michael Lederman of Case Western Reserve University in Cleveland are disputing the value of viral load tests-a standard used since 1996 to assess health, predict progression to disease, and grant approval to new AIDS drugs after their study of 2,800 HIV positives concluded viral load measures failed in more than 90% of cases to predict or explain immune status...""Viral load is only able to predict progression to disease in 4% to 6% of HIV-positives studied, challenging much of the basis for current AIDS science and treatment policy" [] Rodriquez B, Sethi AK, Cheruvu VK, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA 296(12):1498-506, 2006; Cohen J. Study says HIV blood levels don't predict immune decline. Science 313(5795):1868, 2006].
My favoritest of all:
The Red Cross recently reported that even after repeated testing using different test kits, low-risk populations, such as blood donors (or military recruits) will typically yield 12 (PCR-positive) or 2 (ELISA positive) out of 37,000,000 samples, leaving potentially 10 out of 12 false positives, depending on which test kit you believe [Stramer et al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing. New England Journal of Medicine, Volume 351:760-768, August 19, Number 8, 2004].
You really are getting tiring.
Busch et al., in a paper entitled, "Poor sensitivity, specificity, and reproducibility of detection of HIV-1 DNA in serum by polymerase chain reaction. (The Transfusion Safety Study Group. J Acquir Immune Defic Syndr; 5 (9):872, 1992), reported that:
This is another paper that is repeatedly misrepresented by Denialists.
Anybody that actually read the article will note that this paper investigated the detection of cell-free HIV-DNA using PCR.
Viral load tests measure cell-free HIV RNA not DNA. There is little HIV DNA floating around in serum. Viral burden tests measure cell-associated HIV DNA ie. they separate PBMCs, lyse them, and then use PCR to amplify HIV DNA.
Busch et al demonstrated that measuring cell-free HIV DNA lacked sensitivity. Denialists deliberately conflate this result with other tests that measure cell-free HIV RNA and cell associated HIV DNA.
Hey 40 Mules,
Maybe you should brew up a pot of coffee, scroll up to the top of this page, and read every post by Richard Jefferys. I think you will find that most of them are dedicated to addressing issues raised by Andrew Maniotis, usually to point out that Maniotis is misrepresenting the results of the scientific work of others. Maniotis, for the most part, ignores the refutations as long as possible, repeating the same tired lies about the relationship between TLC, CD4 T-cells and AIDS, pretending that it is relevant to the diagnosis of AIDS in Eliza Jane Scovill.
Forty Mules Said:
In case you are too lazy to go back and read the thread, I have pasted, below, some of Jeffery's scientific critiques of Maniotis's purposely deceptive posts
Jefferys Addressing Issues Raised By Maniotis
From June 9, 2007 We find a lucid and polite debunking of one of Maniotis's favorite lies, the one that a high total lymphocyte count is incompatible with AIDS
From June 20, 2007 We find a second debunking of the same lie.
The Red Cross recently reported that even after repeated testing using different test kits, low-risk populations, such as blood donors (or military recruits) will typically yield 12 (PCR-positive) or 2 (ELISA positive) out of 37,000,000 samples, leaving potentially 10 out of 12 false positives, depending on which test kit you believe [Stramer et al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing. New England Journal of Medicine, Volume 351:760-768, August 19, Number 8, 2004].
You are one sick puppy!
Do you really think nobody is going to read the article that you completely misrepresent?
Out of the eight that were enrolled in the follow-up all of them later seroconverted. They were not false positives as you claim.
The paper demonstrates that serologic testing alone would miss a small number of blood donors during early infection before the full development of antibodies. Nucleic acid testing can catch these cases.
Defer et al. in a paper entitled, "Multicentre quality control of polymerase chain reaction [viral load] for detection of HIV DNA" (AIDS 6: 659-663, 1992), reported that:
"False-positive and false-negative results were observed in all laboratories (concordance with serology ranged from 40 to 100%").
This study is all about quality control. PCR is prone to carry over contamination and quality control is extremely important. Out of the 7 laboratories tested 3 showed both 100% sensitivity and 100% specificity by comparison with serology.
Dr. Maniotis, I see that your approach is to change the subject and start lying about something else. Antibody tests are not surrogate markers of cellular immune deficiency, as you well know.
Abbott's Axsym kit says on its label:
"At present there is no recognized standard for establishing the presence of absence of antibodies to HIV-1 and HIV-2 in human blood."
No, it does not. The Axsym HIV test is only available in Europe and the label states no such thing.
http://www.abbottdiagnostics.co.uk/Support/Package_Inserts/package_inse…
Given it's irrelevance, I was intending to ignore the rest of Maniotis's guff.
But I just noticed that he cannot stop falsely attributing quotes.
Maniotis wrote:
A nationwide team of orthodox AIDS researchers led by doctors Benigno Rodriguez and Michael Lederman of Case Western Reserve University in Cleveland are disputing the value of viral load tests-a standard used since 1996 to assess health, predict progression to disease, and grant approval to new AIDS drugs after their study of 2,800 HIV positives concluded viral load measures failed in more than 90% of cases to predict or explain immune status...""Viral load is only able to predict progression to disease in 4% to 6% of HIV-positives studied, challenging much of the basis for current AIDS science and treatment policy" [] Rodriquez B, Sethi AK, Cheruvu VK, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA 296(12):1498-506, 2006; Cohen J. Study says HIV blood levels don't predict immune decline. Science 313(5795):1868, 2006].
It goes without saying that Maniotis is misrepresenting this study. It did not evaluate progression to disease, it evaluated the ability of a single viral load measurement to predict the change in peripheral blood CD4 T cell count six months later.
Given this fact, it is rather obvious that the quote "Viral load is only able to predict progression to disease in 4% to 6% of HIV-positives studied, challenging much of the basis for current AIDS science and treatment policy" does not come from the paper.
It comes from an article Maniotis himself wrote for D. David Steele's/Harvey Bialy's blog entitled "A Brief History of AIDS." This article is now a cut-and-paste favorite among those whose pastime it is to spread denialist misinformation on the internet.
Viral load is also not a surrogate marker of cellular immune deficiency in HIV infection, CD4 counts, CD4% and CD4/CD8 ratio are. Pathologists don't work with these surrogate markers, for obvious reasons.
The question of whether viral load can predict progression to disease was addressed in a recent analysis of the MACS, which reported that baseline HIV-1 RNA measurements explained 47-58% of the variability in time to AIDS or death.
http://jama.ama-assn.org/cgi/content/full/297/21/2349
I said it before and I'll say it again: Dr. Maniotis is a disgrace to the scientific profession.
Richard Jefferys: you seem to be a smart guy with all the answers about HIV and AIDS.
kevin and cooler have a few questions for you:
Why is it that HIV test kit makers have package insert qualifications about the ability of the test to diagnose HIV? When I buy a test kit for blood sugar, cholesterol or blood pressure, the kit makers says it can used for the dianosis of these thingts. Why is it that HIV test makers make statements that their test kit is not to be used to make the diagnosis of HIV?
Which HIV test kit is the gold standard? If there is no answer to this question, then there is no gold standard to compare the results of all the other test kits. If there is no gold standard, then how can the kits be relied upon?
Since you are so proud of your assistance with the Aids Truth web site which, according to the Science article, has links to 100 references. Which of these 100 links prove that HIV causes AIDS? Which of these 100 links validate any of the HIV test kits against a gold standard? IF so, what is the gold standard? Which of these 100 links to articles is the link that shows that anyone who has taken AZT continuously for more than two years is still alive, in other words not killed by the AZT? Which of these links to 100 references shows that ANY anti-HIV drug is capable of eradicating the HIV DNA nucleotide sequence in the human genome? If not, then how can any of these drugs claim to be effective. Which of these links shows that HIV causes a disease in any animal model? Which of these links gives us the method used to isolate HIV and take electron microscope pictures of it?
Since you object to Dr. Maniotis using this quote;
"At present there is no recognized standard for establishing the presence of absence of antibodies to HIV-1 and HIV-2 in human blood."
Please tell kevin and cooler what that recognized standard is for establishing the absence or presenceof antibodies to HIV in human blood.
Your associate said;
Busch et al., in a paper entitled, "Poor sensitivity, specificity, and reproducibility of detection of HIV-1 DNA in serum by polymerase chain reaction. (The Transfusion Safety Study Group. J Acquir Immune Defic Syndr; 5 (9):872, 1992), reported that:This is another paper that is repeatedly misrepresented by Denialists.Anybody that actually read the article will note that this paper investigated the detection of cell-free HIV-DNA using PCR. Viral load tests measure cell-free HIV RNA not DNA. There is little HIV DNA floating around in serum. Viral burden tests measure cell-associated HIV DNA ie. they separate PBMCs, lyse them, and then use PCR to amplify HIV DNA. Busch et al demonstrated that measuring cell-free HIV DNA lacked sensitivity. Denialists deliberately conflate this result with other tests that measure cell-free HIV RNA and cell associated HIV DNA.
Perhaps you would like to inform kevin and cooler about the proposed life cycle of HIV, and what it means to find no significant difference in HIV DNA when comparing cells infected with HIV and cells NOT infected with HIV. Once infected, the cells are supposed to carry HIV DNA in their genome. Right? Are these NON-results because the cells aren't really infected? Or because placebo cells which are not intentionally infected still have HIV nucleotide sequences in their genomes. If so, how did they get there? Are they elite controller cells, or are they like chimpanzees who have HIV in their genomes as a natural resevoir?
Lastly Jefferys, your continued ad hominem attacks against Dr. Maniotis are a disgrace. And coming from a low-life like you, they mean nothing. Compared to Dr. Maniotis, you are a small piece of rejected dust.
I agree with Mr. Jefferys, Maniotis is a disgrace to the profession. And a disgrace to techs like me since he used to be one. We techs are usually analytical and careful and Andrew is the opposite.
I was going to suggest compiling a list of Andrew's outright lies but I don't think even our wink wink deep pocket pharma sponsors, don't I wish, would shell out the cash for the number of full time researchers THAT would take. Isn't it weird how every reference someone looks at from this Andrew guy involves a complete lie? And then he hemms and haws, oh I'll admit it if I made a mistake I left the paper on my desk at home and my ferret ate it.
I'm really hoping Andrew has something good to say about Klausner. How reporting on ONE problematic ELISA and NO false positives means two percent of all vaccinated people test POSITIVE for HIV. And how reporting this has anything to do with EMPHASIZING.
But there's so much else he has to answer for I don't think he'll get to it.
I enjoyed this one from one of the others,
It's time to let this matter rest and respect the family.
written about EJ and the Scovill/Maggiore family a few comments after accusing Elizabeth Glaser of lying about Ariel.
Forty,
This is a science blog. It's fine if you don't know much science but you should be more honest about that and stop pretending. Your comment just now hits a new low since you didn't even understand the passage you quoted.
Forty said
no significant difference in HIV DNA when comparing cells infected with HIV and cells NOT infected with HIV. Once infected, the cells are supposed to carry HIV DNA in their genome. Right?
Of course. For that last part anyway. But this assay is not looking at DNA in cells. Look again at your quote, "detection of cell-free HIV-DNA" this means cells were centrifuged out of the samples. So all you have left are very small things like viruses that have RNA not DNA. And MAYBE, not always, DNA from cells that have died a nasty messy death instead of a neat programmed death. If those cells had some integrated HIV then you MIGHT detect it. There's not much usually if any and that's why the assay is hard.
It's much easier to find RNA from HIV in cell free samples. Or DNA in samples WITH cells. This assay was looking for DNA outside of cells.
Alot of non scientists read this blog and even comment. I think of Ursula who is interested in Morgellon's disease. She is well informed bright and polite. When she doesn't understand something she asks someone who does. I know some scientists don't agree with her on Morgellon's, but she's a good example of someone who knows when to press a point and when not to.
Dear 40 mules, you said:
I endorse the comments Adele made above - this is a science blog and if you have no understanding of science/biology, I suggest you keep your 40 mouths shut. Just think about how ridiculous your claim is.... Yes when you buy a kit to test for blood sugar, it does what it says on the box, and tells you the level of glucose in plasma. So what? ....It is not a test for diabetes, or did you think it was? The manufacturers of glucose assays do not advertise thenm as "tests for diabetes". They are an aid to the diagnosis. What a singularly innapropriate comparison.
Some authorities use a high level of fasting blood sugar to indicate whether the patient has glucose intolerance. You can have a low level, but still have diabetes. You can have a borderline high level, and not have diabetes. You can have a high level and have another reason for testing high, like the use of steroids, or because you are pregnant, and still not have diabetes.
HIV assays just test for the presence of antibodies to HIV. A clinician has to interpret this result and give the patient the diagnosis within a clinical context. How can you not know this and pretend to be knowlegeable about HIV? Do you also not realise that no test kit for any infection makes dogmatic claims about being 100% accurate at confirming the disease is present?
Franklin,
Back in the office this morning and looked at the Crawford-Laurent paper.
The time-course as I wrote it is in the Abstract itself.
Look at figure 7 and its description. It is a repeat of the first experiment but using the mycoplasma removal agent as I said (which is the point of why I mentioned it in the first place). The time couse is as I described it-maximum cell death-days 6,7, maximum virus production later. My description of the experiment is an amalgam between the sentence in the Abstract, and in the description of experiment 7 in the Results of Figure 7. I did it from memory, as I have quoted this many times before to AIDS apologists, who continue to ignore their own data. Admittedly, I fused the two sentences together, which I'm sure you will find fault with. So for doing this, I should apologize. However, there is nothing dishonest, misleading, and in fact, an editor of the paper should have insisted that it be written the way I wrote it for clarity's sake.
The AIDS establishment should have paid attention to it.
Andrew wrote
"in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, whereas maximal virus production occurred at Days 10-17."
For the fourth or fifth time this is a quote from a Perth Group paper except Andrew moved the quotation marks. But Andrew is still insisting it's from Crawford-Laurent, his version of Laurent-Crawford I guess.
Andrew says it doesn't matter because the abstract SHOULD read this way, if the editor had contacted him anyway. And I guess the PERTH group just happened to put it this way too completely independently about 12 years ago.
Fusing sentences misattributing quotes not giving your source combining quotes exaggerating conclusions writing your own conclusions and implying the authors made them misrepresenting data outright lying about data. Sure Andrew, that's perfectly OK in science.
As long as you don't mind getting fired that is. Like what happened to a guy I knew a few months ago. He cooked up some data, got caught, and got fired. There's a fine fine line between being really really bad at what you do like being able to read the literature and lying about it and I think Andrew crossed that line.
Andrew, did you write this paragraph from your above post?
A substantial literature exists documenting that a number of patients present themselves to clinicians with signs and symptoms consistent with the so-called "AIDS defining illnesses." The defining key phrase on Medline is "T-Lymphocytopenia, Idiopathic CD4-Positive" and is often referred to as "ICL." The extraordinary feature of this patient group is that they test negative for HIV. The clinical spectrum is considered diverse and is characterized by opportunistic infections caused by one or more mycotic, bacterial and viral infections. Less frequently parasitic infections are seen. Serologic tests for HIV-1 infection are negative when a screening and confirmatory test are used. In such patients no known cause of immunodeficiency is apparent, nor should it result from immunosuppressive therapy.
Or did you copy it and paste it without giving credit?
Was it an honest mistake? If so, fine. Just admit it. I'm just saying that it is curious that you came up with the same title, subtitle, opening paragraph and nearly the exact same list of articles as is found here. Just linking to it would have worked.
---------
In regards to the coroner's report, it would be useful to note (again) that the coroner did not perform the p24 histology study of EJ's brain (heavy staining for HIV protein in EJ's brain, negative controls read as negative) or the analysis of her lungs. The report includes these items from consultants, in their own words regarding their results.
A case listed as "no cause of death" likely means that the examination has yet to be completed, not that there is no cause.
As to whether or not she had a previous history of health issues, having such an extremely low body weight for her age, when combined with her slide down the weight chart in the previous year would count as the equivalent of wasting in a pediatric case. One of the reasons there is a specialty called pediatrics is that children are not adults.
------------
As to Ariel, her health was failing well before she was given AZT, and improved once a proper delivery method was used. Some of her signs and symptoms could have been complicated or due to AZT (side effects exist for all drugs, especially when attempting to apply an adult therapy to children), but the root cause of death was HIV.
AZT monotherapy increased lifespan for patients over no therapy. "Cocktail" treatments are a further improvement.
------------
For the HIVNET012/ Fishbein controversy, here is an honest review of both the controversy and the science. A consistently overlooked statement from Dr. Fishbein (Cohen, Science 24 December 2004
Vol. 306. no. 5705, pp. 2168 - 2169. Reproduced here.) is that Fishbein says he is "not is disagreement" that nevirapine saves lives. "My issue is not nevirapine, but the process."
------------
For the strawman question of which one paper proves HIV causes AIDS, a single paper rarely establishes the cause of any disease. In the case of HIV/AIDS, an extraordinary amount of research (added to every day) demonstrates causation. Asking for one paper when there is such a wealth of information is simply ignorant.
If there was to be a "debate," then let it be one based not on equal time, but time for evidence. We have evidence. The denialists have conspiracy theories and nothing else.
Dear Adele,
I really really worry about you. I don't know how long you have worked in labs, or in science, and I'd sure like to know what you work on. However, as I stated earlier, I really worry about the "impressionableness" of folks with your bitterness and unwillingness to self-correct.
In fact, one of our greatest grievances with the AIDS establishment is their dogged refusal to self-correct their hypotheses even after we show them again and again to be absolutely wrong. It is the reason, as I stated above, that folks like Gajdusek are like sports stars with their Nobel prizes, and for them to do things like invent theories about slow viruses without any evidence, and then admit to the world that they really just used their positions to gain sexual favors from children, can cause impressionable scientists such as yourself to lose faith in the process of science.
Regarding my apology to Franklin that you so quickly jumped on to show the world what a dishonest scientist I am, it was firstly not addressed even to you, but to him, as an olive branch aimed at demonstrating that when a statement or reference or idea is somehow not as it should be, than as soon as possible (Monday morning in my case), the process of science demands self-correction. For Christ's sake, we have been studying cancer for centuries, and we even have animal models (that are mostly bad ones), and nobody I associate with professionally is expected to be perfect or claims to understand the cause of cancer. Same with all other human diseases. Do you know what causes gravity? Is it those little graviton particles? Is it Ashtikar's tensegrity nets? What is the substance that causes your cell phone to drop to the ground when you let go of it? What is the cause of Alzheimers? What is the cause of anything. The physicists gave up on causality in the 1930's and replaced that kind of primitive thought process with dynamical systems and quantum mechanics. I suggest you read some history of science.
By the nature of your extremely emotional response to my apology to Franklin, I feel that I should at least warn you for your own good that if you are part of a church and there are catechisms (eg. HIV causes AIDS...HIV causes AIDS...HIV causes AIDS...) and if you encounter someone who comes along (like me) and asks a simple question (eg. is AIDS a disease of too few or too many lymphocytes as in the case of Elisa Jane), a scientist wouldn't impune the question asker as you did, but actually look at the process as a positive one. The consequences for what you did are simple: since you want to make a federal case out of my exchange with Franklin, consider the following, and at least carry through with the assigned reading just once in a while at least.
RE: earlier in the blog...
Maniotis:
"I hope you found the quote on page 384 as I posted above. I forgot to also include from the Discussion, second paragraph, on page 837: "Inhibition of mycoplasma growth during an accute infection (figure 7), resulted in modified kinetics of infection in which maximal nucleosomal accumulation coincided with maximal syncytia formation and occurred several days before maximal production of HIV proteins."
(In other words, and Eleni got this right, effect precedes cause in this experiment).
What this statement means (Eleni got this right), is that I agree with the Genetica paper-that not only is cause and effect screwed up in this Laurent-Crawford paper, but that mycoplasma had a significant role to play in Montagnier's hypothesis.
http://www.virusmyth.net/aids/data/ept4cells.htm
Here is the relevant statments:
In a 1991 paper, published in Virology (Laurent-Crawford et al., 1991), Montagnier and his colleagues showed that:
(a) in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, "whereas maximal virus production occurred at Days 10-17"-that is, maximum effect precedes maximum cause;
(b) in chronically infected CEM cells and the monocytic line, U937, no apoptosis was detected although "These cells produced continuously infectious virus";
(c ) in CD4 lymphocytes isolated from a normal donor, stimulated with PHA and infected with HIV in the presence of IL-2, apoptosis becomes detectable 3 days post infection and clearly apparent at 4 days. "Intriguingly, on the 5th day" apoptosis "became detectable in uninfected, PHA stimulated cells". Figure 9, where the data are presented, shows approximately the same degree of "apoptotic events" in the PHA cultures at 5 days as in the PHA+HIV cultures on the 4th day "post infection".
Genetica 95: 5-24, 1995-A CRITICAL ANALYSIS OF THE HIV-T4-CELL-AIDS HYPOTHESIS. Eleni Papadopulos-Eleopulos, Valendar F.Turner,John M. Papadimitriou, David Causer, Bruce Hedland-Thomas,1 & Barry Page1
You really ought to read it... the logic is solid, and exemplary of how a review should be written. Moreover, it is an education in reading about the evolution of "HIV" culturing that may be of value to you people IF YOU'D EVER BOTHER TO EVEN LOOK AT IT!!!
"I will apologize to Franklin on Monday when I can look at the paper again. I can admit making such a mistake if I am wrong."
This was followed by:
"However, contrary to what you suggest, it wasn't meant to mislead-but point out that Montagnier's group was among those who demonstrated a potential role for mycoplasm in fatal immune defficiency, which prompted some of you to correct my spelling..."
"Remember when Gallo said "HIV" is like getting hit by a truck-you need no co-factors. Why don't you read Montagnier. Or is there something unusual about his sexuality or his mother, or perhaps he likes to surf and watch girls like Karry Mullis was accused of doing? Why don't you read his Lancet article on how treatments in vitro for mycoplasm infections abbrogate "HIV" positivity in vitro for some strange reason."
I even drew diagrams to help convey the meaning of these several different issues that are going on in the Laurent-Crawford paper:
"In a 1991 paper that was published in the journal, Virology (Laurent-Crawford, A. G., Krust, B., Muller, S., Rivière, Y., Rey-Cuillé, M.-A., Béhet, J.-M., Montagnier, L. & Hovanessian, A. G. The Cytopathic Effect of HIV is Associated with Apoptosis. Virol. 185:829-839, 1991), Montagnier and his colleagues not only denied the A,B,C's of "HIV" pathogenesis by asserting that PHA was essential for T-cell activation, but they suggested in addition, that mycoplasma played some role in "HIV" pathogenesis. In postulating a role for mycoplasma, the normal sequence of cause and effect during viral replication is reversed, because maximal viral production succeeded instead of preceded, the maximum number of viable virus-producing cells, thus violating what is known about viral replication being dependent on the presence rather than an absence of cells:
" in acutely HIV infected CEM cultures in the presence of mycoplasma removal agent, cell death (apoptosis) is maximum at 6-7 days post infection, whereas maximal virus production occurred at Days 10-17."
"Cell culturists know that mycoplasma infections generate confusion, because they exert cytoplathic effects on cells similar to the way the "AIDS-virus" is believed to act in humans. Cells become "weakened" by this infectious pathogen over time, but cells are not killed outright, as in lytic viral infections."
"But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7. For this to occur, Montagnier et al. would have us forget what is known about viruses. The production of viruses, and there are no exceptions, requires that viruses hijack cellular machinery and cellular materials such as cellular nucleic acids, cellular proteins, and cellular lipids to make more intact virions. Thus viral replication requires cells, not a lack of cells, to replicate, and maximal production of virus should precede and not succeed maximal cell death. Viruses (V) require cells (B) to make more V. There cannot be more V after V has killed most of B, because there would be no materials with which V can make more V, after most of B is killed off. So how are we supposed to accept the AIDS denialist hypothesis of Montagnier et al., that "HIV" actually produces more "HIV" (A) when there is less B (immune system cells)? This makes no sense."
Luc Montagnier et al., therefore advocated several forms of specific AIDS denialism:
Instead of:
"HIV" (A)-----------Immune collapse---(B)-------------------------AIDS-indicator----(C)
diseases
Montagnier et al. claimed:
(A plus but not minus PHA)------------ (B)------------------------------------------------(C)
And:
(A+Mycoplasma---------------------------(B)------------------------------------------------(C?)
removal agent)
"If this is an extract from Eleni's work in Genetica which I quoted above when I said she was correct that effect precedes cause in this critical cell culture experiment by Laurent-Crawford et al., or if it is in a chapter I lifted from a book I have written, and not from Laurent-Crawford directly, I will apologize to Franklin on Monday when I can look at the paper again. I can admit making such a mistake if I am wrong."
I even offered an apology if something wasn't conveyed correctly, as I did some of it from memory as I said earlier.
But it doesn't matter to you that effect precedes cause, that mycoplasma was implicated by Laurent-Crawford's own work in the results and discussion that I pasted above. That people test 6 different times and then their children are accused of dying of something that is associated with 10,800 lymphocytes, that ICL is AIDS without "HIV," that there aren't any animal models (unless you consider SIV an animal model-which I suppose you do because SIV has always been a better model of HIV than HIV.
You could really use some cousilling....I know of a good one in Iowa City if you need one named Mike. I could use some spelling lessons.
Perhaps you would like to inform kevin and cooler about the proposed life cycle of HIV, and what it means to find no significant difference in HIV DNA when comparing cells infected with HIV and cells NOT infected with HIV. Once infected, the cells are supposed to carry HIV DNA in their genome. Right? Are these NON-results because the cells aren't really infected? Or because placebo cells which are not intentionally infected still have HIV nucleotide sequences in their genomes. If so, how did they get there? Are they elite controller cells, or are they like chimpanzees who have HIV in their genomes as a natural resevoir?
Obviously you need things spelled out in small words.
HIV DNA is found predominantly in cells. After a cell is lysed it eventually degrades. Studies that look at cell associated HIV DNA find it in all HIV+ psotive patients. Human immunodeficiency virus type 1 detected in all seropositive symptomatic and asymptomatic individuals.
HIV RNA is found predominatly outside of cell in virus particles. HIV viral load tests quantitate HIV RNA in the cell free fraction.
Maniotis and other Denialists cite the study by Busch et al in an attempt to confuse people. You have demonstrated the success of this dishonest tactic. Maniotis relies on people neither reading nor understanding the study. Again you step up to the plate.
This isn't the first time that some Denialist has misrepresented this study. They keep on bringing it up. They are corrected and then they bring it up again. They never learn.
It really is difficult to see this pattern as anything other than deliberate dishonesty. I find it hard to believe that Maniotis can do real science when he appears to completely incapable of reading and understanding a paper.
You really ought to read it... the logic is solid, and exemplary of how a review should be written. Moreover, it is an education in reading about the evolution of "HIV" culturing that may be of value to you people IF YOU'D EVER BOTHER TO EVEN LOOK AT IT!!!
Get over it. A lot of people have read the Perth Group's "review". It is the complete opposite of what a review should be. The Perth Group start with their conclusion, that HIV does not cause AIDS, and then scour the literature for articles that they can selectively quote and misrepresent in a vain attempt to build a case. They ignore data that conflicts with their ideas. They do not give an accurate review of the available literature.
In fact if you want a model of how to write pseudoscience then this "review" is the perfect example.
"At present there is no recognized standard for establishing the presence of absence of antibodies to HIV-1 and HIV-2 in human blood."
This dates back to the first EIA licensed for the detection of HIV antibodies in 1985. At that stage there was no other standard that Abbott could use for comparison. The Abbott test became the first standard.
"ELISA testing alone cannot be used to diagnose AIDS." (Abbott 1997).
Not alone but in conjunction with a confirmatory test.
"Do not use this kit as the sole basis for HIV infection." (Epitope 1997).
Use in conjunction with an ELISA.
"The amplicor HIV-1 monitor test is not intended to be used as a screening test for HIV, nor as a diagnostic test to confirm the presence of HIV infection." (Roche 1996).
Then what the hell is it used for? Is it a lie detector?
The name of the test should give you a clue - monitoring viral load.
"The NucliSens(R) HIV-1 QT assay is not intended to be used as a screening test for HIV-1 nor is it to be used as a diagnostic test to confirm the presence of HIV-1 infection."
Another test for monitoring viral load.
.....
These different tests are all designed to fulfil different functions.
Some tests were designed for the screening of blood. They typically have high sensitivity but lower specificity. It is better to reject some uninfected blood than to let infected blood get through. These tests should not be used to diagnose HIV infection because the specificty may be too low.
Some tests are designed for use in the diagnosis of HIV infection. If you go to this webpage http://www.fda.gov/cber/products/testkits.htm you will find a number of HIV tests that are specifically licensed for use in the diagnosis of AIDS. These tests may not have as high a sensitivity as the screening tests nad hence should not be used to screen blood.
Some tests are designed to be used to quantify HIV viral load. Carryover contamination is a problem in many of these tests and hence the specificty may not be sufficient for use in diagnosis of HIV infection.
There is no mystery here. The only confusion is that spread by Denialists who try to create the false impression that the tests are all meaningless.
Dear Dr. Noble, You've no question nailed Dr. Maniotis yet again, however, since your link doesn't work for me, could you not, please, spell it out in even smaller words.
Dr. Maniotis quotes Busch et al. saying that:
"PCR-DNA tests on 151 ELISA-negative people found that 18.5% (28 people) had positive PCRs. Furthurmore, only 25.5% of people diagnosed HIV-positive had positive PCR's."
That is 28 false-positives out of 151.
But you, Dr. Noble, say that,
"HIV DNA is found predominantly in cells. After a cell is lysed it eventually degrades. Studies that look at cell associated HIV DNA find it in all HIV+ psotive patients"
The only variable pointed out by you is the risk of (cell)"degradation", so where do the false-positives come from, and, perhaps more importantly, why is this risk of false-positives (and false-negatives) no longer a problem when the HIV DNA is cell associated?
I also find your criticism of the Perth review paper very convincing so far, only I'm disappointed you didn't manage to write "liars" or "dishonest" even once. But I guess "pseudoscience" makes for a nice change. I'm looking forward to seeing all the favorite epithets again once you get to analysing the actual substance of the Perth group's "pseudoscience"... You are going to get to the substance eventually aren't you? Aren't you?
Dr. Noble,
I've been through your list. Does this mean I'm mistaken in thinking that some of these screening tests were previously - perhaps stil are in certain parts of the world - used as diagnostic tests?
Also I couldn't find the diagnostic PCR kit for adults. I remember you saying there now is one. Is that the one they use at Aaron Diamond?
Gravity denier writes:The only variable pointed out by you is the risk of (cell)"degradation", so where do the false-positives come from, and, perhaps more importantly, why is this risk of false-positives (and false-negatives) no longer a problem when the HIV DNA is cell associated?
A proportion of the false positives presumably come from carry-over contamination. When you are trying to amplify very small amounts of cell free HIV DNA then carry-over contamination will be more of a problem. Cutoffs are chosen to balance sensitivity and specificty. Busch et al could have chosen a cut-off that would have given them 100% specificity and 0% sensitivity.
In contrast using cell-associated HIV DNA you can have a test that is close to 100% senistive and 100% specific.
Human immunodeficiency virus type 1 detected in all seropositive symptomatic and asymptomatic individuals.
Hi again Dr. Noble, I've reserved a comment just for "standards". You say the 1985 Abbot test had no standard. Was it not tested against the virus itself?
"First standard" implies there are more. What's the latest standard - you know the standard that says that 2 or more different tests are unreliable singly but reliable when put together? How was that established? By using the 1985 Abbot test as gold standard?
I see, so one tries to balance specificity and sensitivity to obtain the best possible test, choose the right primers etc., the ongoing "quality control" you referred to earlier. Well I guess in the end one would get pretty near perfect results, minus of course problems like the carry over contamination, which would always explain it if things weren't as swell as in the paper you cite.
Does this mean I'm mistaken in thinking that some of these screening tests were previously - perhaps stil are in certain parts of the world - used as diagnostic tests?
Can you provide any example of a screening test by itself being used to diagnose HIV infection?
There is no point in responding to your innuendo unless you have something concrete to say.
Also I couldn't find the diagnostic PCR kit for adults. I remember you saying there now is one. Is that the one they use at Aaron Diamond?
FDA Approves Test to Help Diagnose Main Virus that Causes AIDS
Pope,
What should we call lying, dishonest pseudoscientists, then?
What should we call lying, dishonest pseudoscientists, then?
More to the point, what should we call trolls that deny gravity, get humiliated by their total ignorance of physics, and then come back under a different pseudonym (Pope)?
Here's what it does, dummy:
"The FDA has granted marketing approval for the APTIMA® HIV-1 RNA qualitative assay. The assay may be used as an aid in the diagnosis of acute and primary HIV-1 infection, and to confirm HIV-1 infection in an individual whose specimen is repeatedly reactive (positive) for HIV-1 antibodies."
What's an 'aid in diagnosis'?
So, once you use the non-standardized antibody test, 'repeatedly', you can use this non-standardized, non-specific test to show the po folk that you really doin 'science'.
And, I'll take it that the fact of this 2007 announcement being the 'first' to diagnose any specific infection (which it doesn't), you'll be writing the 40 million and tell them that they can all rest easy - cause their tests weren't valid.
Nicely done, moron. Thanks for filling us 'nonscientists' in.
Dr. Noble,
Of course I can only provide scattered 3rd World examples where 'procedure' wasn't being followed, perhaps because of economic or practical constraints, and a screening test therefore was used for diagnosis on its own. But a screening test combined with a confirmatory WB would still be part of the diagnosis because it's said they are mutually reinforcing.
But since you for some strange reason chose to focus on a question which you thought was mere innuendo, let's return to the real question, because now you're going to tell me that WB provides the diagnosis in these screening-confirmatory combination cases. So where is the gold standard for WB?
Sorry for bringing up same old, same old, but you didn't seem to understand the point that was being made about the tests. For instance, how you can have a test that cannot tell you if something is definitely there, but once another test has told you that something really is there, it can now count it for you. So again to cut to the chase, where is that gold standard?
You gave me the Aptima test, so I presume that's the one Aaron Diamond uses. But that is a prognostic aid as far as I can see, not an diagnostic test by itself. In the very appropriate words of Dr. Robert Frascino:
"Sorry to disappoint. But at this time, APTIMA HIV-1 RNA tests are not meant to be used as a stand-alone test for the diagnosis of HIV-1 infection. A positive NAT result indicates a "probable" infection and must be followed up later with traditional antibody testing to confirm the HIV diagnosis."
However, Aaron Diamodd's business card advertises that,
"IN THE LAST FEW WEEKS HAVE YOU:
-had unprotected sexual activity, especially under the influence of alcohol and/or drugs?
-shared needles and/or your works?
-acquired a sexually transmitted infection?
Do you have any of the following symptoms: Sore Throat, Headache, Joint Pain, Swollen Glands, Fever, Muscle Pain, Fatigue, Rash
If you answered YES to any of these question & don't know your HIV status...
YOU DO NOT HAVE TO WAIT 2 TO 6 MONTHS TO BE TESTED FOR HIV TO BE ACCURATELY DIAGNOSED!!!
Call ADARC for more information about free, confidential HIV viral load testing!!!"
Here it looks distinctly like one of those 'counting tests' has become an accurate diagnosis all on its own. Wouldn't you say that's a bit, what was the word again... "pseudoscientific"?
In the link you gave just above the difference bewteen Aptima and the other counting tests is explained in very small words:
"The sensitivity of the APTIMA assay is comparable to that of FDA approved viral load assays that measure the amount of HIV-1 virus circulating in the blood of patients with established HIV-1 infection to monitor the treatment and progression of AIDS. Unlike the viral load tests, the APTIMA test has been approved for the diagnosis of primary HIV-1 infection, as well as for confirming HIV-1 infection when tests for antibodies to HIV-1 are positive."
The difference between a diagnostic and a non-diagnostic test in other words, is simply that one is approved and the other is not.
But that is a prognostic aid as far as I can see, not an diagnostic test by itself.
No test is diagnostic by itself. All tests for all pathogens have false positives. Doctors make diagnoses using a variety of tests and information.
These NAT tests are meant to be used as an aid in the disgnosis of early and acute HIV infection in the period before antibodies develop. In order for this test to be approved for this purpose the manufacturers had to demonstrate that the test was sufficiently sensitive and specific
As anyone can see the test is remarkably in agreementwith HIV serology. It is also not affected by flu vaccinations, other pathogens etc. This is hardly consistent with the Denialist claims that the tests are completely meaningless.
Even though these NAT tests are highly specific it is still prudent to perform antibody tests after the window period.
Of course I can only provide scattered 3rd World examples where 'procedure' wasn't being followed, perhaps because of economic or practical constraints, and a screening test therefore was used for diagnosis on its own.
Going by your previous attempts at bluffing it is more likely that you are just making the whole thing up and you have no examples at all.
However, Aaron Diamodd's business card advertises that,
Business card? You're not being a little bit loose with the truth again?
Dr. Noble, I appreciate the affirmation that we're in agreement on the fact that no test can diagnose HIV (on its own) And I thank you for repeating the points JD and I just made back at us. You are welcome to them.
However, the question was how Aaron Diamond can claim they can diagnose you accurately with a PCR test?
Dr. Noble for someone whose answers are so desperately lacking in content, perhaps you shouldn't cry 'bluff'so often.
The issue was, has a screening test ever been used as a diagnostic test? The EIA/ELISA tests were they screening test or not. When combined with a WB, or clinical symptoms did they suddenly become part of a diagnosis or not?
Dr. Noble, I appreciate the affirmation that we're in agreement on the fact that no test can diagnose HIV (on its own) And I thank you for repeating the points JD and I just made back at us. You are welcome to them.
Do you really think anyone is fooled by your silly word games? HIV antibody tests are extremely sensitive and specific. They can be, should be and are used in the diagnosis of HIV infection.
However, the question was how Aaron Diamond can claim they can diagnose you accurately with a PCR test?
The data that I have posted demonstrates that these NAT assays are highly accurate. Are they as accurate as weighting for a few months and performing the standard protocol of antibody tests? No.
Aaron Diamond specifically states that you can be "accurately diagnosed" without having to wait for an antibody test, in effect that a confirmatory antibody test is not necessary. But we just saw the NAT test is not meant ot stand alone. Is Aaron Diamond misleading us?
And no I don't think I'm not being precise in describing Aaron Diamond's card as as business card: roping in cattle for their research is their, very lucrative, business
Dr. Noble for someone whose answers are so desperately lacking in content, perhaps you shouldn't cry 'bluff'so often.
At one stage you claimed that you had access to facilities at the University of Leiden to perform characterisation of HIV. I emailed the contact you gave and he said that he hadn't seen you for some decades and that he didn't think you had been active in science since the 1970's. ("Pope" is Wilhelm Godschalk)
You also claimed to have attempted to order HIV isolates from an AIDS reagent program. You hadn't.
You can't blame me for being skeptical of everything you say.
Do you have a reference for Aaron Diamond's "business card"?
Adele said;
Another ad hominem, Adele? It doesn't become you.
Adele wrote;
Thanks Adele for telling everyone what we already know. HIV RNA is commonly measured in the serum, not HIV DNA which is intracellular (intra-nuclear) and measured after cell lysis. The question still remains, as succinctly put by the Pope later in this thread; Some peripheral blood cells are lysing all the time. That's why our urine is orange. Hemoglobin from red blood cells is released and metabolized to urobilinogen. White cells are also turned over and release their DNA into the serum. Obviously these small amounts of cellular DNA products are then picked up in the cell-free serum test sample, and become the subject of the HIV DNA PCR test. The question still remains, why is the HIV DNA test positive(in cell free serum) in those patients who are HIV serology negative? Is it because the PCR test is too sensitive and is picking up backgrond noise? Or is it because gag sequences (which are supposed to be unique to HIV) are floating around in the serum from previous small amounts of cell lysis, as part of normal cell turnover? And if so, then how did these HIV sequences get into the genome of the HIV serology negative samples? Are they present in these serology negative genomes naturally, as they are for primates in the wild, who have HIV and do not get sick.
dt wrote:
Of course you endorse ad hominem attacks. That's your job, as a paid political activist hack.
For Kevin and Cooler; notice the crude attempt at censorship above which is so commonly successful against mindless journalists in the mass media.
dt continues;
For kevin and cooler; notice the contradictions in the above comment. The test kits are "highly accurate and specific", and yet "not 100% accurate". Exactly what is the accuracy and specificity of the test kits and how as this measured against a gold standard? And what is the gold standard? The first test kit? What gold standard was that measured against?
Pope answers both Adele and DT;
This substance meaning; how can maximum cell death(days 6-7) precede maximum virus production (days 10-17)in the 1991 paper, Laurent-Crawford et al?
Robster wrote:
Robster's points one by one:
1) EJ had AIDS because her weight was below normal for age on the pediatrics chart.
If this were true than millions of normal children of low weight on the charts should be given the diagnosis of AIDS by virtue of a weight age chart, a propositon so ludicrous as to be rejected.
2)Ariel Glaser died of AIDS not AZT. Declaring belief in this statement does not make it true. The evidence is clear that both Ariel and Elizabeth died from AZT toxicity. This is as plain as day, and clearly explained in the above thread.
3) Fishbein comment The nevirapine trial corruption is well documented. One statement from Fishbein out of context after he was fired for doing his job hardly changes the hideous crime committed by Tremont who rewrote the research results to get a highly toxic ineffctive drug approved so the drug companies can make more money.
4) For the strawman question of which one paper proves HIV causes AIDS, a single paper rarely establishes the cause of any disease. In the case of HIV/AIDS, an extraordinary amount of research (added to every day) demonstrates causation. Asking for one paper when there is such a wealth of information is simply ignorant.
Kevin and cooler; notice the typical evasion of the question with the typical accompanying ad hominem attack. Any one who asks for a paper that is non-existent is "ignorant". The recent article in Science Magazine states that there are links to 100 articles on AiDS Trueth web site. Which of these 100 articles proves that HIV causes AIDS? Lets have the links please, you brainless, paid political robster hack. There are no papers which prove HIV causes AIDS, because you would have posted them years ago.
chris noble said;
"The Abbott test became the first standard."
Since the Abbott test is the first standard. Please point Kevin and Cooler to the reference which validates this first gold standard test. In other words, how was the sensitivity and specificity of the test determined, and against what gold standard? If there is no such refernces, then you are mistaken in calling this first test a gold standard. It is, in actuality, a false standard.
Maniotis said;
"But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7."
Kevin and Cooler, Notice that was no civil response to this important question, only a continuation of ad hominem attacks typical by the usual list of paid AIDS political activists and hacks.
This is a sad display of the kind of brainless reponses from paid political hacks to serious questions about paradoxes and inconsistencies in the HIV/AIDs literature.
for more info see www.reviewingaids DOT com
Dr. Noble,
I've told you once before long ago that I'm not Wilhelm Godschalk. As it does not matter to me who you think I am, and as you accuse everybody of lying or being cranks anyway, I haven't said anything further about this.
But if Godschalk has wronged you personally in some way, I should tell you again that I am most definitely not him.
I have not published any theories on gravity on the internet or elsewhere. I have not attempted to order HIV isolates from any lab.
I could even be wrong about the exact wording on the Aaron Diamond card, since I don't hold one in my hand at this moment, but "Truthseeker" from "Newaidsreview" is in possession of a newly received card and has personally assured me that the card reads as stated.
http://www.scienceguardian.com/blog/the-aids-paradigm.htm#comment-4744
I do not intend to hold you personally responsible for what Aaron Diamond write on their cards; I am merely pointing out that it looks like clinical research subjects are being put on ARVs on the basis of a PCR test unconfirmed by an antibody test. The kind of 'info' one finds on this card to my mind blurs some ethical lines, so I was genuinely curious as to whether a PCR test, like MacDonald suggests on NAR, is now enough in itself to diagnose an adult with HIV.
For kevin and cooler; notice the contradictions in the above comment. The test kits are "highly accurate and specific", and yet "not 100% accurate"
Yes, yes, we know. Denialists live in a world where anything that is not 100% accurate is completely non-specific.
Tests that are 99.9% specific are highly specific.
I've told you once before long ago that I'm not Wilhelm Godschalk
Sorry, I missed that. In that case I admit to being wrong. I apologise for calling you a gravity denier. Various "rethinkers" have used multiple pseudonyms in the past. I confused you with one of them.
I do not intend to hold you personally responsible for what Aaron Diamond write on their cards; I am merely pointing out that it looks like clinical research subjects are being put on ARVs on the basis of a PCR test unconfirmed by an antibody test. The kind of 'info' one finds on this card to my mind blurs some ethical lines, so I was genuinely curious as to whether a PCR test, like MacDonald suggests on NAR, is now enough in itself to diagnose an adult with HIV.
All I can do is point you to information on the test kits that demonstrate that the tests can have extremely high specificities ~ 99.83%.
You could have done this yourself rather than posturing.
someone said:
Thanks for telling us the tests are 99.9% specific. For the benefit of kevin and cooler, please describe in a few words the method used to arrive at this figure of 99.9% specificity and references which describe this method. Since you have so kindly provided the specificity number of 99.9%, could you please also give us the value for sensitivity as well, along with the method used to arrive at this number.
Also, since your colleague previously told us the first Abbott HIV test represents the gold standard, please give us the reference in which this first test was validated. If there is no reference for this validation method, then this is a false gold standard. This issue has not yet been addressed yet by the paid political hacks. You guessed it. These guys are merely sock-puppets waiting for answers from their corporate sponsors.
The issue of the 1991 paper with cell death max preceding viral production max has still not been addressed. What's the problem? Nothing from the Aids Apologist web sites to cut and paste? Maybe they need more funding from the pharmaceutical companies to answer this one.
"But it should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7. For this to occur, Montagnier et al. would have us forget what is known about viruses. The production of viruses, and there are no exceptions, requires that viruses hijack cellular machinery and cellular materials such as cellular nucleic acids, cellular proteins, and cellular lipids to make more intact virions. Thus viral replication requires cells, not a lack of cells, to replicate, and maximal production of virus should precede and not succeed maximal cell death."
The Busch paper issue of HIV DNA PCR on cell free serum samples raised by the Pope is still unresolved;
The Busch et al. paper, PCR-DNA tests on 151 ELISA-negative people found that 18.5% (28 people) had positive PCRs for HIV DNA in cell free serum. Furthurmore, only 25.5% of people diagnosed HIV-positive had positive PCR's. for HIV DNA in cell free serum. That is 28 false-positives out of 151.
Assuming the PCR test is correctly identifying the presence of HIV DNA, which of course originated in the nucleus of cells in the blood stream, which during normal cell turnover, had lysed their nuclear contents into the serum sample, how did this nuclear HIV DNA get there? In the HIV positive samples, we can understand that the HIV DNA came from infected cells which had lysed. In the HIV serology (ELISA) negative samples, however, where did these HIV DNA nuclear fragments come from, which are testing positive 18.5% on HIV DNA PCR?
For kevin and cooler; notice there are no answers to this question from the hacks. They have only ad hominem attacks for this one and others like it becasue the entire HIV AIDS research machine is riddled with paradoxes. inconsistencies and outright suspension of logic in order to continue massive funding for a 20 year science mistake.
for more information about the 20 year medical blunder called HIV/AIDS research, that is gobbling up public tax dollars at a rate of 8 billion a year on a failed research hypothesis, with no vaccine, no animal model and no mechanism of disease, see:
www.reviewingaids DOT com
Taxpayers are fed up with NIH corruption, wasting public money on failed research with NO RESULTS to show for it. Time to stop the madness and turn off the money.
The Busch et al paper was pushing the limits of DNA detection. They found you can push those limits only so far. HIV RNA is easy to detect and the tests for it are reproducible. It's sensitive and you don't see HIV RNA in negative samples. HIV DNA is easy to detect too when you start with whole cells. Again you don't find HIV DNA in cells from negative samples. But cell-free HIV DNA is very difficult to find if at all.
That's why Busch wrote
"reports of cell-free HIV-1 DNA in serum were somewhat surprising and led to speculation that actively infected cells may lyse in vivo, releasing free HIV-1 DNA into plasma"
Forty tell us DNA in serum comes from lysis of red blood cells and white blood cells. Proving my point yesterday about Forty's knowledge on science. Not an ad hominem, it's just the truth.
Red blood cells don't have any DNA and white blood cells don't lyse. Not normally anyway they can in some diseases. White blood cells do apoptosis and cut up their DNA into tiny fragments while they die so it makes still less likely you can PCR the right sequence even if it's there to start with.
I wonder if Forty or Andrew read the Busch paper. Because they talk about why there are false positives. Almost no DNA to start with so you have to do extra cycles. The primers this SK38/39 pair anyway was also a problem. The more you push things the more you have to wonder how good your results are. Anyone who does PCR can sympathize here. This is a tough project.
What this result doesn't do, is, call the more normal kinds of HIV PCR in question. Absolutely not. I could be like Andrew now and paste a few hundred paper abstracts and the only difference would be, these abstracts would prove my point not disprove it. But I'll be polite so here's just one.
Patrick Braun et al Clin Chem Lab Med 2007;45(1):93-99
"Comparison of four commercial quantitative HIV-1 assays for viral load monitoring in clinical daily routine"
All four tests were 100% specific. Negative samples all IDd negative. Viral loads in patients were comparable. Using HIV standards, dilutions gave linear results. These tests all work well and the differences the authors talk about are really kind of minor.
Forty,
1) EJ had AIDS because her weight was below normal for age on the pediatrics chart.
No. I am describing how pediatric wasting is defined. Low weight and drastic drop in weight for age is how you diagnose wasting in peds cases. Andrew repeatedly is dishonest regarding this.
The nevirapine trial corruption is well documented.
You are confused as to the facts. The trial issues were based around the process of reporting flaws in the research after the study was complete and what clinical practice standards and event reporting definitions were appropriate in areas that may not be equipped to maintain them or where different definitions are used.
One statement from Fishbein out of context after he was fired after he was fired
Proof it is out of context?
...hardly changes the hideous crime committed by Tremont [sic] who rewrote the research results
A safety report was rewritten, not the research results. From the piece I linked to above.
Dr. Tramont's version provided more overview, while the previous version more deeply analyzed the problems -- and was repeatedly critical of management decisions not to investigate certain problems further.
You continue to get a highly toxic ineffctive drug approved so the drug companies can make more money.
All drugs are toxic. Nevirapine's safe use and efficacy is well documented. The point of this study was to determine if single dose Nevirapine was effective in preventing mother to child transmission where no other treatment option is available. The prevention effect isn't great, it increases the chance that the mother will develop resistance, but it is better than nothing.
You quote Andrew "But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7.
This was answered this once before. Andrew is just being intentionally dense. The study mentioned above observes two populations of cells. One population dies off quickly. The second survives to pump out virus.
Any one who asks for a paper that is non-existent is "ignorant".
Try pubmed. Instead of one, I'm offering you thousands. While you are attempting to act as a lecturer, you might point out that you are using a rhetorical gotcha game, signifying nothing.
Lets have the links please, you brainless, paid political robster hack.
You mean I can get paid for my hobby? Where do I sign up!?! BTW, ad hominem, poisoning the well.
...notice there are no answers to this question from the hacks. They have only ad hominem attacks for this one and others like it becasue the entire HIV AIDS research machine is riddled with paradoxes. inconsistencies and outright suspension of logic in order to continue massive funding for a 20 year science mistake.
Forty, there's a pot on the phone. It says you are black. As to the supposed "paradoxes. inconsistencies and outright suspension of logic," just because you don't understand it doesn't mean it is false.
Hey Morons,
Hey Noble,
would you quit using all bold? It's getting me excited.
So, there was no standard in 85, I think you wrote, because the thing was new - you know, it had just been isolated, and the test was made from the isolated thing-a-ma-bob!
Right? Right? So there was no standard? Of course!
I get it now.
And on the 2006 test insert, there is also 'no standard', because, aw hell, we don't need no stinking standard!
I get it now.
And the new PCR test - the Aquaman, or whatever it's called.. The APTIMA... where do they get these beautiful names?
I mean, what drop-out, flunky, cokehead PR advert-bot mutilated a little Latin to come up with this? Aaaptima.
So, the Aptima (hey, I think that's a car, or an autobot?) test, is validated, you creepy hacks, against what?
Against Western Blot.
Against people who test 'reactive' on Western Blot.
And then, but maybe if, and maybe not, if they sort of might also test 'reactive' against one or another standardless antibody test.
(you know, the Roman Standard was something you just wouldn't go into battle without - read the Gallic Wars, it's just bad freaking form)
The beauty of the new test - and read the file - is that they say it tells you if you're "positive" if you're also "negative" on the antibody test!
Get it?!
It's Frakin beautiful!
You see, this used to be a problem - you'd come up heads on one 'test', tails on another, and so it made both tests look like S---.
But now, NOW, NOW they say that's how it's supposed to work!
Get it?
The tests aren't supposed to work together at all!
Beautifical.
You eugenicist, population control, lab nazis sure are geniuses. I'll give you that.
Pure fascist genius. It's like the Politburo never shut down.
Hey, would anyone like to accuse me, or anyone else of being a denialist, liar, fraud, cheat, swindler, pig-farmer, or anything else?
Because here's your chance. I mean, this is where a serious thinker would have to say...
"Gosh, it does seem strange that there has never been a purified, particulate standard for hiv testing. Why is that?...
I wonder if that's ethical?
How is it possible to 'validate' one non-standardized, cross-reactive test against another, with any credulity?"
I mean, that's what a thinking, ethical person would say, so now I'll expect, from the eugenicist crowd, a weeping ream of personal attacks. Let 'em rip, just like Goebbels did.
But I'm down with Dr. Maniotis' question:
What is Aids, a disease of too many, or too few lymphocytes.
I ask because yesterday I took a major unload, after Indian food, you know, and it took a lot out of me, so I was wondering about blood levels, and such.
SO, please let me know. Because usually, I have so much blood in me that I can see it through my skin - which means, I think you're saying - that if I have too much blood - (I think that's what you smart people are talking about when you talk about 'tcells') - if I have too many of those - then I probably have GRID?
Is that Right or Wrong?
Finally, because I hate to be retarded here at the snakepit, in front of all the bright eugenicists (HEY! Isn't Population Control GREAT! Why not just start chemically sterilizing the Black People, Because Nevirapine Just costs sooo much!)...
Anyway, lost my train there...anyhoo, listen,
I'm confused, looking at this report:
One physician's assistant reported that a female patient "died of a blood clot three hours after getting the Gardasil vaccine." Two other reports, on girls 12 and 19, reported deaths relating to heart problems and/or blood clotting."
If I follow your logic correctly, and by God I try, I believe that these people ACTUALLY died of Cervical Cancer?
I mean, because when people on NEVIRAPINE die, they die of Aids? Right???
And these people are also dying, or not being very healthy, also because of Cervical Cancer, isn't that so?
"As of May 11, 2007, the 1,637 adverse vaccination reactions reported to the FDA via the Vaccine Adverse Event Reporting System (VAERS) included 371 serious reactions.
Because drugs can't hurt, and medicine is kind, and beneficent. I know it, you know it, we all know it.
It's a kind, kind business you folks are in, figuring out who can breed and when, and who gets the drug and needle slurry.
I mean, when's the last time you creeps had a hit? Penicillin?
But who cares. Most people believe, like Galileo believed in peer-review. You know, I'm betting it was actually peer-review that killed Galileo. He went up against the Ptolomites.
So, it does work, peer-review. Science. It's not a religion, a fundamentalist philosophy of life, a hierarchy that doesn't budge.
It does work! That's why big bang cosmology is so good, why hiv-ology makes so much sense, and why everybody's dead from the bird flu.
Because you satanic geniuses are always, always, always, always so right.
That said, this whole 'hiv-ology' thing is beginning to look a lot like 'Epicycles' to me.
So, I guess, you know, thanks for keeping the freaky creepshow running. It's always good for a good tear-filled, blood-soaked scream.
Lots o'love,
Oh, I forgot - this is Cervical Cancer too, right?
Of the 42 women who received the vaccine while pregnant, 18 experienced side effects ranging from spontaneous abortion to fetal abnormalities.
I mean, I'm trying to keep up, forgive a poor guy for missing a thing here and there.
Hey, did you know that if you're an 'hiv-positive' suicide in Boston, you've actually died of 'aids'?
That's one freaking amazing virus.
Is that what passes for rhetoric in your world, Demian? Go back to defending intelligent design on evolution blogs, you couldn't do any worse.
Let's put it this way. If your chances of a false result (+ or -) are 1 in 10,000 with one test A, B or C, and you run one person's sample through combination AB, AC, or BC, you get a 1 in 100,000,000 chance of a false result. Run ABC and you end up with 1 in 1,000,000,000,000. Does this begin to make sense?
Robster wrote:
Forty,
EJ had AIDS because her weight was below normal for age on the pediatrics chart.
No. I am describing how pediatric wasting is defined. Low weight and drastic drop in weight for age is how you diagnose wasting in peds cases. Andrew repeatedly is dishonest regarding this.
The nevirapine trial corruption is well documented.
You are confused as to the facts. The trial issues were based around the process of reporting flaws in the research after the study was complete and what clinical practice standards and event reporting definitions were appropriate in areas that may not be equipped to maintain them or where different definitions are used.
One statement from Fishbein out of context after he was fired after he was fired Proof it is out of context?
...hardly changes the hideous crime committed by Tremont [sic] who rewrote the research results
A safety report was rewritten, not the research results. From the piece I linked to above.
Dr. Tramont's version provided more overview, while the previous version more deeply analyzed the problems -- and was repeatedly critical of management decisions not to investigate certain problems further.
You continue to get a highly toxic ineffctive drug approved so the drug companies can make more money.
All drugs are toxic. Nevirapine's safe use and efficacy is well documented. The point of this study was to determine if single dose Nevirapine was effective in preventing mother to child transmission where no other treatment option is available. The prevention effect isn't great, it increases the chance that the mother will develop resistance, but it is better than nothing.
You quote Andrew "But is should be stressed here that it defies logic altogether to claim that maximum virus production is on days 10-17 while maximum cell death occurs on days 6-7.
This was answered this once before. Andrew is just being intentionally dense. The study mentioned above observes two populations of cells. One population dies off quickly. The second survives to pump out virus.
Any one who asks for a paper that is non-existent is "ignorant".
Try pubmed. Instead of one, I'm offering you thousands. While you are attempting to act as a lecturer, you might point out that you are using a rhetorical gotcha game, signifying nothing.
Lets have the links please, you brainless, paid political robster hack. You mean I can get paid for my hobby? Where do I sign up!?! BTW, ad hominem, poisoning the well.
...notice there are no answers to this question from the hacks. They have only ad hominem attacks for this one and others like it becasue the entire HIV AIDS research machine is riddled with paradoxes. inconsistencies and outright suspension of logic in order to continue massive funding for a 20 year science mistake. Forty, there's a pot on the phone. It says you are black. As to the supposed "paradoxes. inconsistencies and outright suspension of logic," just because you don't understand it doesn't mean it is false.
_________________________________________________
Dear Robster,
Thanks for the pubmed advice. I did go onto pubmed and found this paper and this other paper, neither of which prove that HIV causes AIDS.
For the sake of saving time, could you please select a few of the 100 links on the AIDS Truth Web site that prove HIV causes AIDS? Why is it taking so long? It does look a little suspicious that there have been no links to these articles posted here that prove HIV causes AIDS. I know they are out there. Why are you honorable gentlemen holding back this important information from kevin and cooler who would like to see it? It would only take a few minutes of your precious time. We have been asking and asking. Buying all those lemons and garlic for the next Manto demonstration must be very time consuming. IS that the reason why there is no time to post the link to the articles that prove that HIV causes AIDS?
Hey, even Adele explained in a very nice way with a minimum of ad hominems why PCR for HIV DNA on seronegative serum is false positive. It's a tough test, that's why, and they have to do multiple amplifications, sort of like taking a xerox of a xerox 100 times and then not being able to read the print any more.
The least you honorable drug company representatives can do is tell us how the first test by Abbott lab for HIV was validated as the gold standard, and then post a few links to the secret article that only you know about that proves that HIV causes AIDSs. Please don't give the rubbish answer, "go to pubmed, there are thousands of articles there". We just want one two or three, not thousands.
Someone said:
This was answered this once before. Andrew is just being intentionally dense. The study mentioned above observes two populations of cells. One population dies off quickly. The second survives to pump out virus.
Thanks for the explanation. I feel much better now, and when the ER does a routine HIV test on me when I present to the ER with chest pain, and informs me I am HIV positive, I will feel much better I am sure. Of course, it will be a false positive since I am not a gay drug user minority group member, and I have a lawyer who will sue the lab unless they change the little letters on the lab report from pos to neg.
The Nevirapine trial in Africa collected data kept in storage cabinet which was found missing. Would you mind informing kevin and cooler how to write a study of medical data when the storage cabinet holding the medical data is stolen? Just make up new data. That's exactly what they did. If nevirapine is so safe, why is it that none of you honorable gentlement are willing to sample the drug and tell us how great you feel? If nevirapine is so safe, why does it cause Stevens JohnSmith syndrome and liver failure?
Tired of the orwellian doublespeak spoken here by the honorable drug company representatives?, then go to www.reviewingaids DOT com for a breath of fresh air.
Dear Forty Mules and One Plow,
Nice summary above!
Dear Robster,
I read your link to John S. James article. Thanks. I wasn't aware of this link.
Question: How did, "First do no harm" (some misguided Greek said it),
become translated into "it is better than nothing?"
What do you mean by "the prevention effect isn't great, it increases the chance that the mother will develop resistance?"
Is this how you describe that 41.7% of the 875,000 black mother-infant pairs that Tremont, Essex, Lockman, and other concerned souls have drugged that will now supposedly develop "resistance," is better than nothing? (Remember:my question assumes here that "HIV" resistance=eventual death from drug-resistant, "mutant" viruses, while on "life saving AIDS drugs"). Is this why TAG's Harrington in my post above was describing the the effect of prayer on "HIV" and "The Chinese Menu Approach" to AIDS drugging?
Isn't this the same Edmond Tremont who pushed through the experimental anthrax vaccine on the Gulf-War I vets? Is it "better than nothing" that the consequences of this forced vaccine program on Papa Bush's 91 vets have led to 325,000 vets now that are on permanent disability today with "Gulf-War Syndrome," that Asa and Gary et al. demonstrated in every sick Gulf war vet, by linking their illness to the squalene adjuvant used in the vaccine (which they found antibodies for in every sick vet they tested) ( Vaccine A: The Covert Government Experiment That's Killing Our Soldiers and Why GI's Are Only The First Victims by Gary Matsumoto)?
Does your "better than nothing principle" capture the spirit of the oath of that Greek I mentioned above, when experiments on populations sporting numbers with seldom anything ever less than at least 3 zeros following 3-4 other numbers?
"Dr. Tramont's version provided more overview, while the previous version more deeply analyzed the problems -- and was repeatedly critical of management decisions not to investigate certain problems further."
And pigs belong to the avian class.
"All drugs are toxic. Nevirapine's safe use and efficacy is well documented. The point of this study was to determine if single dose Nevirapine was effective in preventing mother to child transmission where no other treatment option is available. The prevention effect isn't great, it increases the chance that the mother will develop resistance, but it is better than nothing."
But can't it be reasonably argued that continued use of these drugs or vaccines, without information provided about their extreme toxicity, along with the litany constantly chanted by the federal government and government-censored media and pharma shills that advocates entire nations should be poisoned with "the life-saving meds and vaccines" that are severely toxic and carcinogenic in animal experiments constitutes a violation of the 1900 Berlin Code of Ethics that established that "all medical interventions for other than diagnostic, healing, and immunization purposes, regardless of other legal or moral authorization are excluded under all circumstances if (1) the human subject is a minor or not competent due to other reasons; (2) the human subject has not given his unambiguous consent; (3) the consent is not preceded by a proper explanation of the possible negative consequences of the intervention;" a violation of Germany's 1931 "Regulation on New Therapy and Experimentation," requiring all human experiments to be preceded by animal experiments, a law that remained in effect even during the Nazi regime; a violation of the 1947 Judgment at Nuremberg Doctors Trials that set forth "Permissible Medical Experiments" - i.e., the Nuremberg Code, which begins: "The voluntary consent of the human subject is absolutely essential;" a violation of the 1962 FDA rule and requirement set in place as damage control for the thalidomide tragedy, after thousands of birth deformities had occurred and which were blamed in part on misleading results of animal studies, which established that three phases of human clinical trials must be completed before a drug can be approved for the market; a violation of the 1964 World Medical Association Helsinki Declaration, asserting "The interests of science and society should never take precedence over the well being of the subject;" a violation of the 1966 NIH's protocol for the Protection of Research Subjects ("OPRR"), calling for establishment of independent review bodies later known as Institutional Review Boards; a violation of the 1973 Ad Hoc Advisory Panel Final Report of the Tuskegee Syphilis Study, that concluded: "Society can no longer afford to leave the balancing of individual rights against scientific progress to the scientific community;" a violation of the 1974 National Research Act that established a National Commission for the Protection of Human subjects, and required Public Health Service to promulgate regulations for the protection of human subjects; a violation of the 1974 National Research Act; a violation of the Title 45 of the Code of Federal Regulations passed in 1975, known as "The Common Rule, "that requires the appointment and utilization of institutional review boards (IRB); a violation of the 1979 Belmont Report, that set forth three basic ethical principles: respect for persons, beneficence, and justice; a violation of the 1980 FDA 21 CFR 50.44 promulgation, prohibiting use of prisoners as subjects in clinical trials shifting phase I testing by pharmaceutical companies to non-prison population; a violation of the 1991 World Health Organization announcement of the CIOMS Guidelines which set forth four ethical principles: respect for persons, beneficence, nonmaleficence and justice; a violation of the 1995 NYS Supreme Court ruling (TD v NYS Office of Mental Health) against the state's policy of conducting nontherapeutic experiments on mentally incapacitated persons - including children - without informed consent. Justice Edward Greenfield ruled that parents have no authority to volunteer their children: "Parents may be free to make martyrs of themselves, but it does not follow that they may make martyrs of their children;" and finally, a violation of the 2001 Maryland Court of Appeals landmark decision affirming "best interest of the individual child" as a standard for medical research involving children. The Court unequivocally prohibited nontherapeutic experimentation on children." (Prepared by
Vera Hassner Sharav).
Is this the same Edmond Tremont, now the U.S. Government's chief of AIDS research and one of our nation's AIDS program directors, who rewrote a safety report on a U.S.-funded drug study, to change its conclusions and delete negative information, and later, ordered the research resumed over the objections of his staff, in order to promote George W. Bush's $500 million dollar plan to distribute nevirapine to African women, even though its approval was withdrawn by the manufacturer themselves in the U.S. several years before because of excessive toxicity ("AIDS Research Chief Rewrote Safety Report." By John Solomon, Associated Press Writer). It has only been a few months since the Institute of Medicine covered-up Tremont's changing toxicity data, according to Johnathan Fishbein, who blew the whistle, and was subsequently fired from his position as safety officer for the Nevaripine trials, that Tremont, his boss, fudged (Aftermath of the Tremont affair: from Washington, D.C., April 8, 2005: "Institute of Medicine Panel Betrays Mission: Covers-Up Wrongdoing, Hides Conflicts of Interest")?
Is this the same Edmond Tremont?
Is this "better than nothing" principle constitute the scientific basis you use to justify drugging millions of human beings?
Yes gulf war syndrome. Lo's mycoplasma incognitus was found in the blood of gulf war one's vets, I wonder how that got there.
www.projectdaylily.com is all about gulfwar syndrome and how when Dr. garth and nancy nicolson discovered it in sick gwi vets, there were several attempts on their life! Its a damn scary book!
Dr. Maniotis, since the name Mark Harrington keeps appearing amidst your false statements, misattributions, empty rhetoric and cringe-inducing buffoonery maybe you should mention that he's been taking combination antiretrovirals for over a decade and is robustly healthy.
The Busch paper issue of HIV DNA PCR on cell free serum samples raised by the Pope is still unresolved;
The real point that is unresolved is why people like Maniotis continually cite this paper in an effort to discredit methods that detect cell-free HIV RNA or cell-associated HIV DNA. The paper describes a technique that is not used.
Why doesn't Maniotis cite some of the numerous papers that demonstrate the sensitivity and specificity of the various NAT assays that are actually used?
Why doesn't Maniotis admit to being mistaken?
Why don't Denialists read and understand the papers they cite?
Maniotis wrote:The Red Cross recently reported that even after repeated testing using different test kits, low-risk populations, such as blood donors (or military recruits) will typically yield 12 (PCR-positive) or 2 (ELISA positive) out of 37,000,000 samples, leaving potentially 10 out of 12 false positives, depending on which test kit you believe [Stramer et al. "Detection of HIV-1 and HCV Infections among Antibody-Negative Blood Donors by Nucleic Acid-Amplification Testing. New England Journal of Medicine, Volume 351:760-768, August 19, Number 8, 2004].
I really have trouble working out what Maniotis is trying to say here. It doesn't look as if he has even read the abstract. The "2 (ELISA positives)" were ELISA negative HIV p24 antigen positive. They also weren't false positives as Maniotis claims. Eight out of the twelve were followed up and all of them seroconverted. Far from showing that NAAT assays are innacurate it shows how reliable they are.
Look at the numbers! There were 12 out of 37 million HIV RNA positive HIV antibody negative tests. Eight (and most likely all) were not false positives but initial acute infect cases. This is hardly the completely non-specific test that the Denialists would like you to believe.
How anyone can think that this article supports HIV Denialism is beyond me.
Yes gulf war syndrome. Lo's mycoplasma incognitus was found in the blood of gulf war one's vets, I wonder how that got there.
Can you guys get your conspiracy theories consistent! Which one was it squalene or mycoplasma? Perhaps you can debate each other?
Again, you are being intentionally dense, Andrew. Single dose Nevirapine is better than nothing for preventing mother to child transmission. Where there are better alternatives, single doses should not be used. When doing nothing is more likely to be harmful than using the only protocol available in that time and place, doing nothing is the unethical (and apparently your) choice.
Forty, keep looking. I'm sure you can do better than just finding denialist prattle. You want proof. I give you overwhelming proof, but you try to play games. I know you won't go there, but AIDSTruth has a page discussing denialist myths. You are looking for the section headed by Myth: HIV does not cause AIDS. The "historic" Gallo and Montagnier papers can be found from there, but require purchase if you don't have a subscription. Their joint NEJM 2003 article can be accessed for free.
The proof has only gotten stronger since the mid eighties (which is why I sent you to pubmed), while the behavior, drug abuse, malnutrition, treatment cause AIDS hypotheses fell apart in the face of more research (keep on reading the myths page). Some once great researchers couldn't admit that they could be anything but all knowing, and became the core of the denialist movement.
Gulf war syndrome was fake, all the veterans who were sick, going blind are lying, when they passed on on to their families they were lying, they had abnormal brain scans, those were fake...............
Its called different hypothesis's that honest scientists use to try and solve a problem. There are difffernt theories that are used to possibly explain cancer, so all those advancing those theories are quacks right?
Man i dont even know why I talk to you, you need to start hanging out with some hot girls, go to a bar and get a life.
Gulf war syndrome was fake, all the veterans who were sick, going blind are lying, when they passed on on to their families they were lying, they had abnormal brain scans, those were fake...............
Who said that?
Honest scientists publish their theories in peer reviewed journals. They don't write B grade science fiction stories.
nicolson has posted his reasearch on gwi/cfs in peer reviewed journals. I posted them on the other thread.
Nevertheless the peer review process is rigged, did it save the 100,000 people that died of Vioxx? If some lone scientist had evidence it was a bad drug people like you would say "witch" "charlatan"
nicolson has posted his reasearch on gwi/cfs in peer reviewed journals. I posted them on the other thread.
So can I see his evidence that mycoplasmas were developed as a part of bioweapons program and that soldiers in the Gulf War were deliberately infected? Or do you have to read his sicence fiction book for this?
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&cmd=Retrieve&dopt=Ab…
Nevertheless here is Nicolsons peer reviewed work on GWI.
It's funny how you badmouth a scientist far more accomplished than you.
Oh I see, the peer review process is perfect when it publishes a paper you like, but rigged when it publishes one you don't? How quaint.
Peer review is not rigged. You also clearly have no idea as to how the Vioxx cardiovascular problems came to light - it was not because of poor peer review of the papers but because Merck did not reveal certain side effect data. No peer review process would detect this. Red herring, straw man, whatever.
In fact, science self corrects - reports of higher than anticipated deaths began to emerge and were duly recognised (with the help of the peer process), forcing Merck to reveal all their research data to independent review.
The Vioxx deaths were estimated as 27000 initially by the FDA, and revised upwards subsequently to a maximum of 55000. Where on earth do you get your 100 000 figure? Let me guess - the same crackpot web sites you get your HIV and conspiracy theories from, no doubt.
Some more peer reviewed work on the lack of an association between Myco infections and illness in Gulf War Vets:
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=ShowDetailView&T…
http://www.ncbi.nlm.nih.gov/sites/entrez?Db=pubmed&Cmd=ShowDetailView&T…
Oh, sorry these don't count I guess, because the peer review process is "rigged".
In fact, if there is publication bias, it virtually always works in favour of papers showing a positive outcome or correlation. Papaers showing no association between events are difficult to get into press usually.
"No peer review process would detect this"
Yes this means the peer review process can fail the American people at protecting us.
I propose scientific juries, Americans are usually right in criminal trials that involve a lot of science, and experts are usually wrong because of conflicts of interest in the judicial system.
Theoretically if we had scientific courts/juries, A whistleblower inside Merck could have alerted a scientific court, and a grand jury could investigate, a whistleblower would have a tough time publishing a peer reviewed paper when most of the editors are hacks who only publish theories that don't rock the boat of big pharma/cdc's dogma.
Whistleblowers don't need to publish papers - they just need to blow the whistle.
And your 100 000 figure? Care to tell us where it came from?
hahahahaha
Man, you are really bad news to lie like this. The monkeys that Lo injected with mycoplasma incogitus all wasted and died, the control didnt, they didnt show antibodies, and when they did they did weakly, and only when near death. You have to use the PCR, a scientific jury would never let you get away with this, this is the argument Nicolson has been making for years.
See unlike the microbes you push, mycoplasma incognitus has an animal model. The real reason you do this is because you can't accept research thats from scientists without conflicts of interest, only research from the drug companies and the CDC matters to you. I feel bad for people with CFS who are lied to by drug company sycophants like you.
Oh by the way, where is the animal model for HPV and hepatitis C? Oh yeah they were backed by big drug companies so you just mindlessly accepted there hypothesis, yet when other scientists with out conflicts of interest propose a hypothesis you scrutinize it, and youre still wrong in the end.
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&cmd=Retrieve&dopt=Ab…
See unlike the microbes you push, mycoplasma incognitus has an animal model.
An animal model for what exactly?
GWS, CFS, ALS, arthritis, AIDS, autism?
Despite various claims there is no firm link between any of these and mycoplasmas.
youre right,
because your thoughtful inquiry we should alert people that hep c and HPV are not caused by microbes, because there is no animal model at all for these microbes.
Where did you buy your phd?
youre right,
because your thoughtful inquiry we should alert people that hep c and HPV are not caused by microbes, because there is no animal model at all.
Man you are really an idiot. Im going out now wont be here till late night.
Cooler, peer review is a scientific jury. A jury of your peers = peer review.
You have found pubmed. Congrats. Now, run this search. "hepatitis C animal model." You will find this article as the current second result. If you run "human papillomavirus animal model" you will get some useful results as well. Do you ever fact check your claims before you post them?
Very few animal models are perfect, and it is important to remember that humans and other animals do not always respond to viruses in the same exact manner. Human papillomavirus is a human virus. Some viruses do not readily infect other species at all, but that doesn't mean that they don't exist or that they don't cause a specific disease. In some cases, the only animal model available is the human, and we have to study patients or accidentally infected medical workers.
------------
As to the Nicholson's paper (or any paper) showing that M. fermentans incognitus contains HIV surface proteins, could you point me to that, or is it only in the novel?
Yo Yo Yo puss and blood experts,
where's the freaking purified gold standard? I mean,
Where is the gold standard? What is it? Please, don't keep me in stitches and suspense. (you cads, you're just such a bunch of teases!)
So, look, what is it, the Gold Standard, the pure particulate thing-a-ma-bob. The one and only. Where is it. what is it? When is it? What does it taste like?
Chocolate?
(I had one once, a little coin, and when you unwrapped it, it was chocolate on the inside. But I lost it, or ate it.)
What is the Gold Standard?
Where, when, how, what?
Because, well, I'm confused again. Because, well, here's the test that Spongy Noble told us, scolded us, was the new and improved PCR test that really, really showed us.
The APTIMA® HIV-1 RNA Qualitative Assay is an in vitro nucleic acid assay system for the detection of human immunodeficiency virus (HIV-1) in human plasma. It is intended for use as an aid in the diagnosis of HIV-1 infection, including acute or primary infection.
[Yay! Aiding in diagnosis for 25 years - HIV testing, the test that 'aids' in Aids!].
Presence of HIV-1 RNA in the plasma of patients without antibodies to HIV-1 is indicative of acute or primary HIV-1 infection.
[Wow. Wow! So, if the one test is positive, and the other is negative - I mean... 'reactive' and 'non-reactive', I mean - above the cut-off and below... I mean...oh, it's so confusing.... I mean, you can be 'positive' no matter what! WHOOOO HOOO!]
The APTIMA HIV-1 RNA Qualitative Assay may also be used as an additional test, when it is reactive, to confirm HIV-1 infection in an individual whose specimen is repeatedly reactive for HIV-1 antibodies. This assay is not intended for use in screening blood or plasma donors.
[But of course, it couldn't tell who's really 'positive' unless they're 'at risk', you know? Not like a healthy, non-risky blood donor. Gosh, it wouldn't work on just Anybody...duh].
But then it goes on and there's just so much more to it, like if one test is sort of positive, like once but not twice... and then, if it's sort of negative, like twice but not thrice,
3. If a specimen is nonreactive on an HIV-1 antibody test and reactive in the APTIMA HIV-1 RNA Qualitative Assay, then the specimen should be retested in duplicate in the APTIMA HIV-1 RNA Qualitative Assay.
[But, wait, I'm confused again. I thought this was a test for something. Not for nothing, or for two things? Or, I guess I'll have to wait and see...]
and then there's the importance of screening, you know, for Negro antibodies, and Gay-cells, and the like.
Anyway,
What's the standard?
Really, won't somebody send me some help, because I'm running this little clinic, all by myself, in deepest Australianus, and it's hard to know, you now, just by running the tests..
And I always get the cow and goat syrums all mixed up, and sometimes I don't have the newest software, so I'm not sure if the algorthimicization is doing right by the cut-off protocol decisionator - and it's really confusing, because everybody's not Black and Gay!
So, please send help, and tell me:
What is the Gold Standard, the Purified Particulate Smithsonian Reference Standard, for the test, and from whence did it come?
(and then, I'm still confused as to Dr. M's question - is Aids a disease of too many or too few blood cells, because the other day, and you'll find this funny - but the other day, I swore I was about to burst - I passed by this girl, I think she was from an exotic island of some sort, but whew - and suddenly.. anyway..) But, that didn't go very far, and I just paid my bill and left - it was a store, don't get cheeky you filthy monkeys!
But my question was, and I'll just reiterate it here for the people in the cheap seats:
What is Aids? Too many blood cells, or too few?
and don't forget about the 'standard' thing, while you help me out with the second question.
Thanks,
With Love and Puss and Blood,
The real reason you do this is because you can't accept research thats from scientists without conflicts of interest, only research from the drug companies and the CDC matters to you. I feel bad for people with CFS who are lied to by drug company sycophants like you.
If there was solid evidence that mycoplasmas cause CFS, GWS, ALS tec the drug companies would be telling you how great their antibiotics are for these conditions.
I cannot see any logical reason for drug companies to be part of this massive conspiracy.
What is Aids? Too many blood cells, or too few?
Your question has been answered several times.
AIDS is characterised by the depletion of a specific subset of T-cells -- CD4+ cells.
I read the entire thread. I thought global warming and religion threads brought out the stupid like no other. I was clearly very very mistaken.
Robster wrote;
Thanks for pointing us to the one single article which proves that HIV causes AIDS. First, let me ask Adele, Raven, franklin, Jefferys, cooler and Kevin if they all agree that your article is the one that proves HIV causes AIDS. I just want to be sure about this. I wouldn't want to spend all my time reading an article that is NOT the ONE that proves HIV causes AIDS. Would you? Thsi is the article, right?:
The Discovery of HIV as the Cause of AIDS by Robert C. Gallo, M.D., and Luc Montagnier, M.D. NEJM. Volume 349:2283-2285 December 11, 2003 Number 24,
"Other indirect evidence that HIV was the cause of AIDS came from the demonstration, in 1984, of its high degree of tropism for the subgroup of CD4+ T cells, its consistent isolation from patients of different origins who had AIDS, and the isolation of similar viruses that cause AIDS in nonhuman primates (specifically, macaques). "
Why does it say indirect evidence? Where is the direct evidence? That's because THERE IS NO DIRECT EVIDENCE that HV causes AIDS?
Why does it say "high degree of tropism for T cells"?, and not, "HIV infects and KILLS T CELLS"? That's because HIV DOESNT kill T cells. This is well known and accepted by all, even by the honorable drug company representatives here in this discussion.
HIV doesn't kill T cells. Right?
Why does it say "consistent isolation" from AIDS patients. Shouldn't it say isolation from ALL AIDS patients?
That's because HIV was "isolated" from only a fraction of patients with AIDS in Gallo's original papers 1981-1984.
How was HIV isolated? Does it say how HIV was isolated? Did they grow HIV on a cell culture, purify it and take an electron microscope picture of it? Why is it that there are high level electron microscopy experts who say they never did this? That's becasue they never did this.
Why do they say "similar viruses" cause AIDS in macaque monkeys. Why not say, THE EXACT SAME VIRUS causes AIDS in primates?
That's because HIV doesn't cause AIDS or ANY disease in chimpanzees, gorillas, orangutangs, baboons or any other primate.
The disease in macaques is not caused by HIV. It's caused by SIV from another monkey, and this occurs only in the laboratory and never in the wild. Hardly an animal model of HIV.
HIV injected into a primate has NEVER reproduced the kind of agonizing death suffered by Ariel Glaser. That's because the poor little girl died of AZT poisoning. There is no animal model.
Where does it mention Koch's postulates? Aren't these Koch's Postulates the ones that are used to prove an infectious agent causes an infection? It doesnt mention them.
"Thus, the causative relation between HIV and AIDS was accepted by the scientific and medical community in 1984"
This states that proof of causation that HIV causes Aids was published before 1984 and was accepted by the scienctific community. Could you please point to the articles which proves this in the time period from 1981 to 1984?
In fact, there were none, and this is essentially a false statement. A causal relationship WAS NOT and IS NOT proved, and there are no publications proving a causal relationship between HIV and AIDS from 1981 to 1984, or after 1984 for that matter. I would ask the many honorable drug company representatives to post these references, or admit there aren't any.
Yes, a causal relation was accepted by the scientific community, but this was without scientific proof. It was accepted because of MONEY from NIH and browbeating those who questioned the hypothesis.
" and was further verified through the later isolation of HIV type 2 in West African patients with AIDS." I will leave this for others to comment on this one.
" The relation was also supported by the clinical efficacy of drugs that specifically inhibit HIV enzymes and the demonstration that mutations in one of the coreceptors for HIV (CCR5) make some persons highly resistant to HIV infection and AIDS."
This statement is your basic lie. The drugs have no clinical efficacy beyond KILLING the patient. The CCR5 receptor stuff is essentially hogwash.
People are resistant to HIV because HIV is NOT the cause of death 10 to 20 years after infection by means of a long term immuno-suppressive disease which destroys immune cells. People have died from AIDS, yes, this is true. However, HIV is not the cause of the the opportunistc infections or of death.
There is no mechanism of disease which shows a diagram of HIV killing T cells in any medical publication.
HIV is, in truth, a benign passenger virus, similar to other opportunistic microbes found in malnourished, chronic drug users, and people repeatedly exposed to foreign antigens, and infectious agents like repeated STD's.
The toxic drugs, like AZT, can NEVER eradicate a nucleotide sequence in the human genome, which is what HIV is.
For the UNtruth about HIV and AIDS, goto AIDS Truth dot com.
For the TRUTH about HIV and AIDS, go to www.reviewingaids DOT com.
HIV is, in truth, a benign passenger virus, similar to other opportunistic microbes found in malnourished, chronic drug users, and people repeatedly exposed to foreign antigens, and infectious agents like repeated STD's.
If HIV is "benign" then why is the incidence of immunosuppression many times higher in those malnourished, chronic drug users or people repeatedly exposed to foreign antigens etc. who are HIV positive than it is in those who are HIV negative? Or why is the mortality rate of HIV positive babies born to HIV positive mothers so much higher than the mortality rate of HIV negative babies born to HIV positive mothers? Doesn't sound very "benign" to me.
HIV injected into a primate has NEVER reproduced the kind of agonizing death suffered by Ariel Glaser. That's because the poor little girl died of AZT poisoning. There is no animal model.
Ah the Fortieth version of science! Actually, every time someone gets HIV from IDU, another primate is getting injected with HIV and later getting AIDS.
We're all primates Forty hate to break it to you. Are you a creo too?
And what ever happened to your professed concern for the "family"? But your right on this: there's no good animal model of AZT toxicity at therapeutic dose. Go and actually read all those studies Duesberg lists. They use much higher doses than you ever get in the bloodstream OR they don't see an effect OR the only effect is at like the pre-implantation embryo stage and in culture.
And what's this about EMs and no one ever seeing virions by EM? You want to live in the past? Nitpick a paper from 1983? Go ahead. But there are thousands of people who have looked at virions by EM including me even though I'm not an expert on it at all. There are EMs from patient tissue, from culture, purified etc. You know this if you've ever read anything on the subject.
Dear Dale,
Have you ever known any chronic heroin addicts? Alcoholics? Crack-addicts? These unfortunate syndromes afflict approximately 10-15% of humanity. The only proven remedy is abstinence. They are all potentially fatal conditions for the true addict (believe it or not, alcoholism is a progressive and fatal disease, even though nearly all alcoholics you meet in life will be functional until the very latest stages, and they perform their jobs fairly well as functional alcoholics until they crash). Opiate-based addictions (and alcoholism) are known to be extremely immune suppressive in the late stages (for example, a sizable fraction of late stage alcoholics die of pneumonias when their absolute T-cell number crashes).
I have to admit, it has always absolutely dumbfounded me when AIDS apologists talk about how harmless long-term drug addition is, and how they absolutely ignore the realities of chronic additions. Although the medical profession and the insurance companies have acknowledged that alcoholism, for example, is a disease that demands treatment that is covered by medical insurance like diabetes or any other potentially fatal disease, at the same time, the church of medicine often looks the other way when the "messy" subject emerges, and still, like most people, doctors (and many many scientists for some reason) continue to treat it as a behavioral and moral issue.
Personally, I know of a drug and alcohol rehab facility near where I live. I have known both chronic heroin addicts and alcoholics. This facility is unusual because it is filled with doctors-it is a specialty program that treats addicted physicians. Many of them have been caught "diverting" (taking oxycontin while at work), or passing out on the ER floor, or caught in a routine or suspected drug screen). When these docs are caught, their shingle is confiscated until they complete the 6-10 week program.
Do these doctors have AIDS or are they immune-suppressed like an "AIDS patient" (do they have too few CD4 cells or low absolute counts)? Most of them don't, of course. Depends on how long and how heavy they have been using, their genetic background, the presence of co-morbid conditions, etc. But every now and then, there will be one who is profoundly immune suppressed.
As someone posted above:
"As of January 1, 1997, the number of infants and children in USA diagnosed with AIDS was 6,891 and ninety percent of these cases had mothers who were drug users (Fauci A.S., Braunwald, E., Isslbacher, K.J., et al. Harrison's. Principles of Internal Medicine. (McGraw-Hill Companies, Inc. New York USA, ed. 14, 1998)."
AIDS scientists themselves have even suggested that some that the immunotoxic effects of chronic intravenous drug addiction or popper use itself may lead to immune suppression meeting the surveillance definition of T-cell numbers seen in "AIDS" patients (see Haverkos, J. Biosci. 1 Vol. 281, No. 4, June, 2003).
Peutherer et al., HTLV-III antibody in Edinburgh drug addicts. The Lancet 2: 1129-1130, 1985.
The clean needle programs were the biggest joke of all.
"Here Mr. Hendrix. Let us give you a sterile shooting works so that you can continue to dose yourself with heroin. We know for instance that heroin is exceptionally immune suppressive to the extent that when we give a single cycle of morphine to certain patients in the hospital, their T-cells can drop for about a month as much as a few hundred in number. But go ahead-shoot up with this clean needle!"
According to the CDC, there has been a cumulative 956,666 US AIDS cases with 530,756 AIDS deaths in the 24 years between 1981-2005. By 1986-87 the accumulated cases of HIV was already hovering around 1 million and HIV prevalence has remained there ever since.
These are the official adjusted, back-calculated, artificially inflated by including healthy people with low CD4 cell count and AZT victims, numbers. And still the cumulative death toll by 2005 is only half the prevalence of any year from 1986 onwards.
I'm sure there are a few of the pharma reps here who would want to take this opportunity to congratulate themselves on the efficiency of their drugs, so let me add this little bit:
During the 1980s, surveillance tracked only AIDS cases. Using this information, CDC estimated how many new HIV infections were taking place each year. Estimating new HIV infections was easier back then because the time between getting infected with HIV and coming down with AIDS was predictable. One could track backwards from the time AIDS was diagnosed and estimate when the person was infected with HIV. However, starting in 1996, better treatments made the time between HIV infection and progressing to AIDS very unpredictable.
http://www.cdc.gov/hiv/topics/surveillance/index.htm
Until 1996 the rate of AIDS and death was so predictable it could be used for the government's self serving back-calculations. And still by 2005 AIDS deaths haven't caught up with HIV incidence anno 1986. One can only conclude it was the early toxic treatments that made the statisticians' calculations so easy in the eighties. When it turned out that people didn't after all die of HIV with the same certainty that tells John Moore dropped things will fall to the ground, and that the new milder drug treatments no longer killed people reliably, it became impossible to calculate anything anymore, which is why the life expectancy of an HIV+ person in the US has been rapidly pushed up standing currently at ca. 24 years.
Adele said;
Your defense of AZT as a safe drug with no toxic side effects is profoundly misplaced
Perhaps you could tell me when and where I said this. I don't deny the toxic side effects of AZT including on mitochondrial DNA. AZT was the best thing we had for a while but it's not something you want to eat in kilograms.
What I said was, AZT doesn't kill animals in doses like the ones used in people.
Your exaggeration of what I said is like the "Hendrix" exaggeration about drug users. Please don't come at us again with that "blessedly nontoxic" quote. It was taken out of context and its what fifteen years old? Of course drugs are toxic! Heroine like AZT isn't something you want in your system. It's not good for you. No one questions it.
HOWEVER toxic effects of injection drugs are not AIDS and only an idiot could confuse them with AIDS. HIV positive drug addicts almost always get immunosuppressed, get OIs, die of AIDS-related conditions while HIV negative drug addicts do not.
Why is this so difficult to understand?
EM. Above I said alot of people "looked at virions by EM including me even though I'm not an expert on it at all."
And Mules writes,
Since you are knowledgeable in this area
I'm not an expert like I said but anyway.
please tell us where the cell sample came from for the EM you saw, and how you prepared this sample, or others prepared the sample for electron microscopy, and when you looked at this EM photo, please tell us how you were able to confirm that the small structure you are seeing on the EM photo is actually an HIV retrovirus, and not a look-a-like by mistake? It is possible to see a small structure on an EM photo and mistake it for another similar looking small structure. Is this not correct? How was it confirmed that the small structure was actually an HIV retrovirus?
Cells are infected with a purified virus, one sample, and a control, second sample, like a replication def virus or heat killed virus or something like that. At different times or maybe at just one time depending on what you look for you "fix" the cells and get them ready for TEM or SEM. You can look this up on Wikipedia I'm not going throw the details of embedding and slicing.
Weird thing is, you see these little particles with cones in the middle in the cells getting good virus. And you don't see these little particles with cones in the middle in the no virus or bad virus cells. And you do a p24 assay and a reverse transcriptase assay on the same samples. There's lots of p24 and lots of RT activity in the ones that got the virus but none in the ones that got the same virus except it was inactivated. And now Andy scratches his head and says, but there's RT activity in everything. Guess not at this level!
So now you say, Gee, maybe that p24 and RT were just floating around they're not really in those particles I see. So you go back and do more EM and this time you label your sample with some antibodies to some HIV proteins. You can put some gold spheres on those antibodies so they show up in your picture. A big one like 10nm for one protein a little one like 5nm for a second protein. And holy baby orangutan, they're all clustered on those particles with the cone cores in them. And in the control sample that's the one where you don't see those same particles you also don't see any labelling!
Can you see other particles? Yeah, microvesicles are everywhere. But they don't get labeled and they are all different sizes. Sometimes you can even see, hi Eugene, an ENDOGENOUS RETROVIRUS PARTICLE. But not many and not labeled like the HIV.
Your question about "possible to see a small structure on an EM photo and mistake it for another similar looking small structure" Yeah, if it's like 1980 and your working with a new virus and you don't have good antibodies or if it's today and you're not doing your experiments right. In 2007 the tools are around for HIV and there shouldn't be mistakes like that. And thkere usually aren't.
"Yes of course, humans are classified as primates. Not disputing this. As a matter of fact, I personally know a few apes who wear three piece suits, carry a briefcase and work for major pharmaceutical companies."
LOL
40, There may be extremely uncommon exceptions (which if they do occur usually end up being written as case reports in the journals because of their rarity value) but as a general rule of thumb one can say:
Drug users without HIV do not die of severe "AIDS-related" opportunistic infections.
HIV seronegative babies of HIV seropositive Moms do not die of severe "AIDS-related" opportunistic infections.
Gay men without HIV do not die from severe "AIDS-related" opportunistic infections.
Blood transfusion recipients and hemophiliacs without HIV do not die of severe "AIDS-related" opportunistic infections.
etc... etc...
Re "other indirect evidence":
I am amazed you fail to appreciate all the "direct" evidence indicated by Gallo and Montagnier before they then turn to the other, indirect evidence. Can you read or not?
The fact that they point to additional further "indirect" evidence just strengthens the causative link.
You like asking for "one paper" that proves that HIV causes AIDS. How about you give us one paper in return...
Seeing as how the majority of drug users in the world do not have HIV, it should be easy to provide us with a paper showing that thousands of HIV negative drug users have had Pneumocystis pneumonia. They must, by your own reckoning, considerably outnumber the cases in HIV positive drug users.
So lets have one paper, just one, showing that thousands of HIV negative drug users have had PCP.
Failure to post a paper will be recognised as acceptance by you that that your claims are bogus.
For some of you just now learning about HIV like coolerfrummybilly and Forty a good place to start is this NIAID sheet from 1995. http://www.aegis.com/factshts/niaid/1995/niaid95_fact_sheet_evidhiv.html
In it you find Forty's primate model,
Already by 1995 there were "three laboratory workers with no other risk factors who have developed AIDS or severe immunosuppression after accidental exposure to concentrated, cloned HIV in the laboratory. Two individuals were infected in 1985 and one in 1991. All three have shown marked CD4+ T cell depletion, and two have CD4+ T cell counts that have dropped below 200/mm3 of blood. One of these latter individuals developed PCP, an AIDS indicator disease, 68 months after showing evidence of infection, and did not receive an antiretroviral drug until 83 months after the infection. In all three cases, HIV was isolated from the infected individual, sequenced and shown to be the infecting strain of virus"
Some more, "through 1994 the CDC had received reports of 42 health care workers in the United States with documented, occupationally acquired HIV infection, of whom 17 have developed AIDS in the absence of other risk factors. The development of AIDS following known HIV seroconversion also has been repeatedly observed in pediatric and adult blood transfusion cases, in mother-to-child transmission, and in studies of hemophilia, injection-drug use and sexual transmission in which seroconversion can be documented using serial blood samples"
And of course about drug use causing AIDS,
"matched controls, individuals with similar lifestyles but without HIV infection, virtually never suffer these symptoms. For example, in one cohort in Vancouver, investigators followed 715 homosexual men for a median of 8.6 years. Every case of AIDS in this cohort occurred in individuals who were positive for HIV antibodies. No AIDS-defining illnesses occurred in men who remained negative for HIV antibodies, despite the fact that these men had appreciable patterns of illicit drug use and receptive anal intercourse."
and
"in the NIAID-supported Multicenter AIDS Cohort Study (MACS), 22,643 CD4+ T cell determinations in 2,713 HIV-seronegative homosexual men revealed only one individual with a CD4+ T cell count persistently lower than 300 cells/mm3, and this individual was receiving immunosuppressive therapy"
and
"Prior to the appearance of HIV, AIDS-related conditions such as Pneumocystis carinii pneumonia (PCP), Kaposi's sarcoma (KS) and disseminated infection with the Mycobacterium avium complex (MAC) were extraordinarily rare in the United States. In a 1967 survey, only 107 cases of PCP in this country had been described in the medical literature, virtually all among individuals with underlying immunosuppressive conditions. Before the AIDS epidemic, the annual incidence of Kaposi's sarcoma in the United States was 0.021 to 0.061 per 100,000, and only 32 individuals with disseminated MAC disease had been described in the medical literature.
"By December 31, 1994, physicians had reported to the CDC 127,626 patients with AIDS in the United States with definitive diagnoses of PCP, 36,693 with KS and 28,954 with disseminated MAC."
More lies from the washed up psuedoscientist.
Its funny how hiv "debunking" sites mentions 3 anecdotal cases, while ignoring the thousands of long term non progerssors, focus's on the very few animals that have gotten siv, while ignoring the thousands more that have not gotten hiv/aids.
BillyFrummyHunny,
I thought you didn't read my comments, but I see you got at least a few lines in. But you must've stopped reading by,
"through 1994 the CDC had received reports of 42 health care workers in the United States with documented, occupationally acquired HIV infection, of whom 17 have developed AIDS in the absence of other risk factors. The development of AIDS following known HIV seroconversion also has been repeatedly observed in pediatric and adult blood transfusion cases, in mother-to-child transmission, and in studies of hemophilia, injection-drug use and sexual transmission in which seroconversion can be documented using serial blood samples"
Three plus 42 = 45. Remember this is from 1995 twelve years ago. There's lots more now but I'll let you find that yourself. Maybe you'll get to do some reading after you figure out that Tower 7 architecture? And how they did that mycoplasma mind control on those innocent Saudi guys?
Ugly,
All anecdotal, no info on AZT/drug use/other microbes/catastrophic stress we know nothing about these people bc its all anecdotal given to us in a one second soundbyte.
Fails to mention the thousands of long term non progessors with hiv, etc etc.
Design a study that controls for confounding factors, not these random blurbs on someone's website.
Dear Adele,
I'm not scratching my head. Just shaking it in disgust and in concern for you. I didn't say there was RT in everything: Temin and Varmis did:
For instance, Reverse transcriptase "is a normal protein found in the uninfected cells of yeasts, insects and mammals" (Varmus H,. Reverse transcription Sci. Am. 257:48-54, 1987).
Once claimed by AIDS scientists to be a specific component required for "HIV" replication, and a surrogate marker for the presence of "HIV" in cultures, reverse transcriptase or RT is now published in market magazines concerning biotechnology stocks that have nothing to do with retroviruses (Pachez M. No need to be phased. Shares, 28-32, 2001).
I have a document from the U.S. Department of Health and Human Services Center for Biologics Evaluation and Research from November 19th, 1998 (Vaccines and relatated biological products advisory committee meeting-I could email you the PDF), and in it is a rather lengthy discussion beginning on page 13 by Dr. Arifa Khan entitled: "Update on reverse transcriptase activity in chicken cell derived vaccines:
"Initially Boni et al., in 1996 published that low level reverse transcriptase activity was detected in all chicken cell derived vaccines using a highly sensitive PCR-based revrese transcriptase assay called PERT, which can detect on to ten virions."
This initial finding was reported to WHO, and then additional studdies were done by several labs in Europe, as well as the US, including the NIBSC, the CDC, as well as labs in the FDA to confirm this initial finding, as well as to expand on this and to evaluate the use of the PERT assay and other PBRT-related assays for analysis of vaccines...
"And after confirmation that there was a RT activity present in all chicken cell derived vaccines, the important question, of course, was whether this RT activity was associated with a retroviral particle; and more importantly, whether this retrovirus particle could infect and replicate in human cells, and therefore be of public health concern."
"Studies done by other groups are summarized here. The RT activity was found to be associated with retroviral particles of two distinct avian endogenous retroviral families designated as EAV and ALV."
The document goes on and on, but essentially, it isn't out of the question that your children have had some of these chicken HERV's jabbed into them, and that on a sensitive assay, they might have developed antibodies to these exogenously introduced endogenous chicken HERV's.
As far as you EM statements are concerned, you might want to look at the EM's showing how "pure" the little particles you are describing were, that is, if you can find them in the cellular debris
http://www.virusmyth.net/aids/data/eppretoria.htm
BTW, regarding the ongoing discussion of animal models of "HIV" disease, you might want to try studying goats and sheep (baaahaaa) and dogs (arf!), because they test positive for the "unique" structural proteins of "HIV," and don't develop AIDS, so you can save a lot of money because your animals will not become sick. I have already mentioned that p24 can be found in the thymus glands of "uninfected" children (3), but alas, I'll reference it again. Please find the plagerized references below.
cheers,
Andy
1. Willman et al., Heterophile Antibodies to Bovine and Caprine Proteins Causing False-Positive Human Immunodeficiency Virus Type 1 and Other. Enzyme-Linked Immunosorbent Assay Results. Clinical and Diagnostic Laboratory Immunology, p. 615-616, Vol. 6, No. 4, July 1999.
2. Strandstrom et al., Studies with canine sera that contain antibodies which recognize human immunodeficiency virus structural proteins Cancer Res 1990 Sep 1;50 17 Suppl :5628S-5630S. (In this study, they claim that 50% of dogs tested positive.
3. Dura WT, Wozniewicz BM. Expression of antigens homologous to human retrovirus molecules in normal and severely atrophic thymus. Thymus 22 (4):245-54, 1994.
Adele,
My mistake: I said
"they might have developed antibodies to these exogenously introduced endogenous chicken HERV's."
Should be:
they might have developed antibodies to these exogenously introduced endogenous chicken CERV's.
So sorry,
Andy
Oh my Billy,
lookism sexism AND denialism? Why am I not shocked?
You really should read comments before responding to them.
Here's the second quote you missed and it's not a random blurb this one was published confounding factors and everything. Published in Lancet, 1993. Schechter MT et al "HIV and the aetiology of AIDS"
"matched controls, individuals with similar lifestyles but without HIV infection, virtually never suffer these symptoms. For example, in one cohort in Vancouver, investigators followed 715 homosexual men for a median of 8.6 years. Every case of AIDS in this cohort occurred in individuals who were positive for HIV antibodies. No AIDS-defining illnesses occurred in men who remained negative for HIV antibodies, despite the fact that these men had appreciable patterns of illicit drug use and receptive anal intercourse."
And NIAID isn't "someone's website." Maybe your confusing it with your mycowoo black helicopter my cat died of gulf war syndrome website. Which I'm sure is scrupulousely peer reviewed with thousands of thank you letters and all.
yes that study didnt control for azt, woo woo woo woo woo woo woo
Woo woo man you guys are weird to talk like that, you guys sound like aliens from another planet! Is that suppoosed to be funny? I could see you preforming stand up comedy going woo woo woo woo woo and the crowd looking at you like a complete lunatic!
I could imagine all of you mindless sycophant rejects in a room going woo woo woo woo woo woo woo woo woo for days! you guys are so weird and such social outcasts to talk like that! Woo woo woo woo!
WOoooooooooooooooooooooooooooooooooooo!
Forty,
Seriously, fact checking would really help you find your way to reality.
There has never been an animal model in which HIV injected into a primate, ANY PRIMATE, has produced an animal model of AIDS.
Rarely, chimps will develop OIs in HIV animal models, but as has been said before, demanding perfect animal models is not realistic.
There have been no IRB approved studies of HIV injection into human primates,...
Well, duh. But there have been accidental exposures.
and non-human primate injections which have been tried and tried, don't CAUSE AIDS in PRIMATES.
They do rarely. Animal models are not perfect.
There have been a few anectodatal cases of HIV self-injections by a human, NONE OF WHICH CAUSED AIDS. There have been numerous HIV positive needle sticks in health care workers over the last 20 years, and some serocnverted, HOWEVER, NONE OF THESE NEEDLE STICKS EVER CAUSED AIDS in the recipient of the needle stick. If you disagree, please post your reference which contradicts this statement.
This is the standard Duesbergian lie. Needle-sticks have led to both seroconversion and AIDS. In the 1994 CDC year end report, 17 of 42 documented US healthcare workplace exposured to and infected with HIV had progressed to AIDS. Other sources can be found here. From the table of contents, click to "Koch's Postulates Fulfilled," "Evidence From Blood Donor-Recipient Pairs," and "Single Source Outbreak of Pediatric AIDS."
Cohen (Cohen J. Fulfilling Koch's postulates. Science 1994c;266(5191):1647) mentions the accidental exposure of three laboratory workers to a lab strain of HIV, as reported by Blattner. Quoting Cohen,
Duesberg lied (and when confronted, resorted to hand waving), and his hangers on repeat these lies without ever investigating them. Partly because of the attention that accidental exposures to HIV and other pathogens, vastly improved control of any and all "sharps" and biohazard safety protocols came into use, along with the preventative use of anti-HIV drugs for exposed workers. Even with these, seroconversion does sometimes occur, and progression to AIDS does occur.
You beat me to it, Adele, but as usual, Forty doesn't look (google, pubmed, read) before he leaps (parrots denialist lies).
yes that study didnt control for azt
That's true. But it was peer-reviewed. And it showed illegal drug use or poppers doesn't cause AIDS. And it showed a "homosexual lifestyle" doesn't cause AIDS.
So will you concede on this peer-reviewed evidence that illegal drugs or poppers and homosexuality don't cause AIDS?
At the truly dreadful prospect of being accused by Jon Cohen of 'handwaving',
How many needlestick-AIDS cases are documented in peer-reviewed literature? How many thousand needlesticks per year and how many semi-anecdotal cases of needlestick-AIDS? 1 (one) in the first decade of the 'pandemic'. Then all of a sudden 42 'reported on that "somebody's website" that's even less fond of referencing its anecdotes than Adele is. So, ok, how many of those 42 cases have appeared in peer-reviewed literature?
Haemophiliacs: People constantly requiring blood transfusions, hardly the perfect animal model wouldn't you say...? although we're told by the resident expert that animal models can't expected to be perfect in the first place, which is why chimps don't get AIDS. Tell us, Adele, have chimps always been such an imperfect animal model for human infectious diseases?
Robster could perhaps fill us science illiterates in on how the almost proverbially unstable HIV survived the treatment it received as part of the clotting factor it was supposedly in?
yes that study didnt control for azt, woo woo woo woo woo woo woo
Woo to you too.
You obviously spend too much time reading Duesberg rather than reading the science.
Duesberg has made up a number of ad hoc excuses for ignoring the clear evidence in the Ascher and Schechter paper that recreational drugs do not cause AIDS.
One of them was that it was really the AZT that caused the CD4+ cell depletion, immune deficiency and opportunistic infections.
The data doesn't support this ad hoc excuse.
Of the 169 HIV+ patients that developed AIDS (none of the HIV- patients did) 90 had their AIDS diagnosis before starting AZT and a further 51 had CD4+ counts less than 300 cells/uL. So unless AZT has the magical property of travelling back in time then Duesberg is full of hot air.
Why does it say "high degree of tropism for T cells"?, and not, "HIV infects and KILLS T CELLS"? That's because HIV DOESNT kill T cells. This is well known and accepted by all, even by the honorable drug company representatives here in this discussion.
HIV does kill T-cells both directly and indirectly. However, direct killing is not the major way that HIV caused CD4+ depletion.
Duesberg cites this paper as evidence that HIV exists.
A molecular clone of HTLV-III with biological activity
He for some reason that is known only to himself ignores the data that shows that HIV has biological activity. (They also used controls in this experiment)
Don't you think it is a bit of an incredible coincidence that a virus with a tropism for CD4+ cells is found with an incredible degree of correlation in people with a disease characterised by severe CD4+ cell depletion?
"Maybe your confusing it with your mycowoo black helicopter my cat died of gulf war syndrome website"
Adele is on record mocking gulf war syndrome and the thousands of people who were sickened and ended up dying , and the thousands who claimed thier illness was contagious.
The next time a gulf war syndrome dies, ADele go to the funerals and do the "woo woo dance" I'd love to see it, do the two step back and forth, woo here and a woo there on the dead bodies of the gulf war vets, woo woo! You are one sick puppy! woo woo woo! woo!
gulf war syndrome vet
Adele is on record mocking gulf war syndrome and the thousands of people who were sickened and ended up dying , and the thousands who claimed thier illness was contagious.
No, she's making fun of people that make up half-baked conspiracy theories about Saddam Hussein weaponising mycoplamsas by adding the Env gene from HIV.
the mycoplasma was found in the blood by PCR,(useless to look for antibodies, scroll back) it wasnt found in healthy controls, mocking and making fun how it got there is not nice. I dont know how it did, but it's not something to joke about. Or do you enjoy doing the woo woo dance! do it give me a Wooooooooooooooooooooooooooooooooooooooooooooo!
And cant believe grown adults talk like complete loonies!
wooooooooooooooo
wooooooooooooooooooo
wooooooooooooooooooooooo!
News flash, thats not funny at all, its totally weird. You guys should go to a bar and hit on hot girl, and go woooooooooooooooowooooooooooooooowooooooooooooooooooooo and she what she does. LOL
And I
and see
Cooler,
"woo" is slang around here for pseudoscience. Has anybody verified that M. fermentans incognitus contains an HIV gene? That claim doesn't show up anywhere outside of conpsiracy pages and some fiction novel. You would think that a mycobacterium picking up a viral gene would be worthy of some investigation.
------------
Pope,
How many needlestick-AIDS cases are documented in peer-reviewed literature?
Look it up yourself. Needle-sticks are tracked as a requirement of medical worker safety laws.
How many thousand needlesticks per year and how many semi-anecdotal cases of needlestick-AIDS? 1 (one) in the first decade of the 'pandemic'. Then all of a sudden 42 'reported on that "somebody's website" that's even less fond of referencing its anecdotes than Adele is.
Those are CDC records. Why don't you ask for access to the records?
Lets go through this step by step. First, a needle-stick occurs. Is the patient HIV+? That cuts the chances right there. Based on the patient status, we move to the second step. The healthcare worker typically goes on a prophylactic course of ART. This has the effect of limiting the chance that the worker will seroconvert. Next, said worker, based on how their personal disease progresses, typically takes years to progress to AIDS.
The denialists say that there aren't any needle-stick AIDS cases, and then there aren't enough.
So, ok, how many of those 42 cases have appeared in peer-reviewed literature?
Pubmed is that way ^^
Haemophiliacs: People constantly requiring blood transfusions, hardly the perfect animal model wouldn't you say...?
Well, they are humans, and they received the equivalent of multiple exposures, not through transfusions, but via Factor VIII treatments, which were pooled from multiple blood donations. Now that Factor VIII is made either through recombinant DNA technology or through the traditional method plus improved purification, these exposures don't happen, and hemophiliacs aren't becoming HIV+ at a rate higher than the general population. So the denialist claim that Factor VIII causes AIDS is obviously false.
although we're told by the resident expert that animal models can't expected to be perfect in the first place, which is why chimps don't get AIDS. Tell us, Adele, have chimps always been such an imperfect animal model for human infectious diseases?
The answer to that depends on the disease.
Robster could perhaps fill us science illiterates in on how the almost proverbially unstable HIV survived the treatment it received as part of the clotting factor it was supposedly in?
Not knowing the specifics of Factor VIII production, all I can say is that enough virions survived processing to be capable of causing infection. The current protocol includes previously absent donor screening and testing systems along with techniques to prevent the survival of viruses in the purified plasma product.
the mycoplasma was found in the blood by PCR,(useless to look for antibodies, scroll back) it wasnt found in healthy controls, mocking and making fun how it got there is not nice. I dont know how it did, but it's not something to joke about. Or do you enjoy doing the woo woo dance! do it give me a
Where are the peer reviewed papers demonstrating that he found a weaponised mycoplasma containing an HIV Env gene?
Where are the gene sequences?
In 1999 (War and Health) they write: Although this preliminary result will require conformation by sequencing the mycoplasma genome in the area of the putative inserted gene...
Well it's 2007 now. Where is his evidence?
Has anyone verified that Gallo said HIV is caused by a cytopathic retrovirus like he claimed in 1984, oh yeah I'm sorry HIV is now an autoimmune disease because it became known after gallo's press conference that HIv was was only present in 1 out 500 t cells or so! Hiv is an autoimmune disease now, classic case of a futile attempt to "save the hypothesis"
I asked that fool Joel gallant the hiv specialist from Johns Hopkins and he admitted its a "diffuse" immune response that causes depletion, Pure speculation to save the hypothesis.
I'd have to review the evidence to see why he made that claim. You are not a scientist and are not that intelligent so you wouldnt understand that if you make one preliminary error it doesnt nullify all your work, I dont even know if its an error.
A good scientist can make mistakes and admit to them, he doesnt claim that now, but he must have had good reason to say that, considering all the awards he won, and how you are just a washed up loser with no life who's totally miserable. All you do is sneer at scientists that are not bought off by drug companies.
What about your Idol Gallo when he said people will die in a year or ten, how about how he bypassed peer review and went public with no published papers? What about how he stole the virus from montagnier? When he admitted the virus he detected was barely detectable, in only a small fraction of t cells? HOw about that he admitted years later in the Parenzee trial that a partial correlation isnt enough to prove casuation? Why did the loser go public than?
I really don't enjoy talking to you at all. Hopefully Dr. Mantious will come back and further humiliate you.
I'd have to review the evidence to see why he made that claim. You are not a scientist and are not that intelligent so you wouldnt understand that if you make one preliminary error it doesnt nullify all your work, I dont even know if its an error.
It does shed some light on his ability to find mycoplasma sequences.
Nicolson still seems to be spreading his story about mycoplasmas with an inserted HIV env gene through his non-scientific and fictional works. That is a mark of pseudoscience.
What about your Idol Gallo when he said people will die in a year or ten, how about how he bypassed peer review and went public with no published papers? What about how he stole the virus from montagnier?
Gallo is hardly my idol. It is informative that you spend most of your time attacking Gallo rather than dealing with the science that has accumulated in the last two decades. It reminds me of Creationists going on about Darwin and anti-vaccination kooks going on about Pasteur and Maniotis going on about Gajdusek.
Gallo didn't bypass peer-review. Look at the dates on the Science papers. He had submitted his paper, it had been peer-reviewed and accepted for publication before the press conference was held. Gallo wasn't the person who called the press conference anyway.
Despite what people suffering from DTWS (Denialist Time Warp Syndrome) might think the world didn't stop in 1984. Gallo's initial work has been replicated time and time again and the connection between HIV and AIDS has gotten stronger and stronger.
This is more than I can say for Nicoloson's work which have never moved past a weak correlation.
Is anyone else here struck by the quite bizarre paradox of Cooler and his mycoplasma theories? He bends over backwards to excuse ropey and unrepeatable pseudoscience and uses every logical fallacy in the book to talk up his claims there is viable evidence. Even when his "experts" are caught with their trousers down, he lamely says they allowed to make mistakes if they correct them later (which they don't). Evidence for his pet myco theory is almost nonexistent, and countered by a large volume of good science to the contrary.
Yet as soon as HIV is discussed, he demands 100% certainty in all things - 99.9% is not good enough. No margin for error, no scope for scientists modifying hypotheses in the light of new data, no acknowledgement that there is a vast bulk of peer reviewed science providing evidence HIV causes AIDS and refuting alternative hypotheses, nada.
Cooler, I'd be surprised if mycoplasma could accrue just 0.1% of the evidence for its causation of AIDS/GWS/CFS/whatever that that HIV has for its link with AIDS. Science has a habit of sorting out fact from fiction. Get over it.
Hi DT, good to hear from you. Why should we only accept the 40% HIV that Gallo found and not the 100% required by Koch's Postulates? Aren't there HIV-Negative cases of AIDS, which disproves HIV being the vector? When does correlation equal causation? Beyond all of that, what I have found to have major problems is with the HIV Antibody Test. When was the Antibody Test validated? Why did the CDC make the decision in 1987 that having antibodies must equal active infection? Why aren't the proteins in the HIV Anitibody Test unique and specific for HIV? Why can 70 things cause a false positive to the test? Not to mention other odd things such as HIV-Negative persons have been found to have high viral loads, Britain will not use the Western Blot Test and an Ameican can walk across the border to Canada and no longer have AIDS. These are the disclaimers in the ELISA Antibody Test and the viral load test, respectfully, "there is no recognized standard of establishing the presence or absence of HIV-1 or HIV-2 in human blood" and "not intended to be used as a screening test for HIV or to confirm HIV infection." Nevertheless, these tests are used daily.
DT, you must realize that most rethinkers were on the same side as you originally but when things do not add up, what are we do do, pretend that they don't exist? I for one want proven facts, which seem to be lacking. Where is just one epidemiology study proving once and for all that HIV causes AIDS? The scientists must be too busy spending our tax dollars on other things than to do what should have been done years ago. Another question for you, why wasn't Robert Gallo nominated for a Nobel Prize? Surely the discoverer of the plaque of our century deserves this honor.
Cooler is looking forward to the return of "Dr. Mantious"
So am I!
When "Dr. Mantious" writes he humiliates himself by lying about better scientists and what they do. Like when he lied about J. Klausner saying two percent of flu vaccine people testing HIV positive. Another honest mistake I'm sure. Klausner said nothing like that and neither does anyone else whose respectable. We went throw those early 90s papers last week and the flu vaccine probably doesn't cause false + and no way 2%. "Dr. Mantious" told us he would talk about the Klausner thing but he didn't. He changed the subject but then yesterday he brought up flu vaccine AGAIN. Gotta hand it to him, good liars should be shameless. And he is.
Yes I hope Dr. Mantious returns because when he does he also humiliates people who
1) try to exploit the real sufferings of many African Americans and other minority groups for their own pseudoscience ends by lying about "pharma" or "big gubmint" conspiracies to kill black mothers with nevirapine or something so crazy ridiculous it hurts your brain.
2) ridicule the suffering of some Gulf War veterans by making up crap about how their CAT died of it.
3) cover up their own disgusting ideas about sexuality or race by accusing other people of them.
Noreen,
I'm glad to see you are still doing well. I hope your health holds.
Why should we only accept the 40% HIV that Gallo found and not the 100% required by Koch's Postulates?
You are going by statements regarding science from 20+ years ago using techniques of the day. HIV is in 100% in AIDS cases now.
Aren't there HIV-Negative cases of AIDS, which disproves HIV being the vector?
No. There are cases of idiopathic CD4+ lymphadenopathy. Its progression and duration differ from AIDS, is exceptionally rare and the cause is unknown, although there are some interesting hypotheses as to what might cause it.
When does correlation equal causation?
Perhaps you should ask that of the denialists pushing long disproved concepts of drug abuse, behavior, Factor VIII, treatment, etc as causing AIDS. After spurious correlations were corrected for, they had nothing, but couldn't admit it.
Where is just one epidemiology study proving once and for all that HIV causes AIDS?
No level of proof will convince the denialists. Many epi studies have been done that reasonable people accept.
I don't know if Billy is really a high school kid but it's funny to see him attack Gallo.
Also first let me say I respect Gallo and he definitely does alot for people who suffer with HIV and AIDS. But cooler really. Gallo wasn't the only person to ID HIV. There was Montagnier who is NOT a denialist. And also Jay Levy. Did you ever hear of Jay Levy? He isolated HIV and wasn't involved in that French-USA flap at all. And there were others.
I really like what Chris said. Attacking Gallo is like attacking Darwin. So if Darwin didn't get EVERY SINGLE THING right and ID EVERY SINGLE FOSSIL in the world, that means evolution doesn't happen?
But the "Nicolosons" are right. Sure.
Actually, my health is fine thanks to LDN, which I believe would be a better choice of drugs because of basically non-existant side effects and it does seem to prevent O.I. indirectly. I enjoy reading what all of you highly-educated people have to say. I still go to the doctors not for my sake but theirs. You see they do not understand how I am doing so well but it is not magic just good, old-fashiioned health habits. I am in contact with many people, like myself, who have given up the antiretroviral drugs and they too are leading normal lives without incident.
Dear Adele,
Your comments are completely wrong and out of line.
First, go ask Joyce Ann Haford about nevirapine. Unfortunately, she is not talking now, since was killed by Nevirapine. She was a pregnant Black lady who was hideously executed by her doctors with a deadly toxic drug called nevirapine as described in this Harpers Magazine article.
Adele, perhaps you are unaware that Harpers Magazine is not a conspiracy rag sheet. It is a mainstream American publication.
Go and ask the Health Minister of South Africa for her opinion on nevirapine, or any other toxic drug for HIV, for pregnant black women of South Africa. She and the Prime Minister have rejected these deadly toxic drugs as you should, too. The government of South Africa and others repected people believe that administration of these drugs to pregnant black women is a form of Institutional Racism, and Iatrogenic Genocide.
You know as well as I do that toxic drugs can NEVER eradicate a nucleotide sequence in the human genome, and that is what HIV is.
There has never been a placebo controlled study showing any benefit AT ALL from nevirapine.
The NIH study conducted in Africa to get nevirapine approved was flawed by missing data, severe corruption, and academic misconduct all documented by Dr. Jonathon Fishbein who was hired to make sure the research was conducted properly, and instead was fired when he pointed out the flaws, corruption and academic misconduct in the nevirapine trial. His story is public information. You know all this and yet you still defend the drug. You are a hypocrite, Adele. This is not a "gobmint conspiracy", these are real people dying from toxic drugs, and others like Fishbein standing up for what is right. This is a lesson you can learn from, Adele. Stop pandering to drug company interests. Big Pharma corporations are the most profitable corporations in the history of western civilization. They don't need you to defend their profit margin.
For more info, www.reviewingaids DOT com
new link to fix broken link to Harper's article on nevirapine, Jonathon Fishbein, Joyce Hafford etc.
my apologies.
http://www.harpers.org/archive/2006/03/0080961
I'm glad you're still doing well too Noreen. I'm interested in learning more about naltrexone and HIV because I don't know literature on it. Is there some information you recomend? And does anyone else here know about this?
Also Noreen have you thought about helping in any studies? There are alot of scientists looking for people like you who have HIV and are doing ok without antivirals. I know you might be skeptical about HIV science but that would be a major way to help other people who aren't doing as well as you if you want to.
The death of one woman is a despicable screw up by some medical people at least if it really happened the way Farber describes. Tens of thousands of black kids with AIDS because you took away the drugs, that's genocide. And THAT'S out of line, plowboy.
The Health Minister of South Africa is responsible for tens of thousands of deaths in babies who never would've had HIV and then AIDS if their mothers got the drugs. And if people like your collaborator friends didn't put the fake "White Western Science" stamp of approval on it.
And Forty Harpers gave the finger to good journalism when it decided to publish that denialist shrew's lies without doing any fact checking. And then defended Farber and its own crap editing. Are you a journalist Forty? You can respect Harper's but alot of people don't anymore including me.
You know your "placebo control" argument is bunk but you keep using it anyway. Go ahead. Nevirapine is better than other drugs it was tested against at reducing mother to child transmission. And because of people like you and your friends tens of thousands of black South African babies got HIV needlessly. Maybe you aren't racist I don't know you but you have to admit some denialists are. There's a whole crew of you who are ultra right-wing nuts homophobes too. And anyway the results' the same as if you were.
I'm sorry one woman died supposedly of nevirapine. Again we just have one person's word on this. If it's true the woman's doctors weren't doing what they were supposed to do. Farber knows that and you should know it. These drugs have to be monitored they're not candy. If used right and monitored, they aren't going to kill anyone though.
Thousands of kids in the United States are Alive and Well today because Nevirapine and other drugs and safe practices took a 20-40% transmission rate down to like 1%. Alot of those kids would be dead today if you had your way. And guess what? Many of them are African-American.
So again, you exploit the bad care ONE African-American woman got for your own ends. And the goal of your propaganda is to get rid of drugs that let tens or finally hundreds of thousands of African-American kids actually have a chance in this world.
Robster said:
This is a basic blatant lie based on the phoney definition of AIDS as REQUIRING a positive HIV test. TB is AIDS if the HIV test is positive. TB is not AIDS, and is merely TB, if the HIV test is negative. This is called a tautology which is making something "true" by its definition. There are plenty of immune suppressed patients who are HIV negative, and have low T cell counts and opportunistic infections. In reality these should be called HIV negative AIDS cases. Anyone who gets high dose corticosteroids and dies of disseminated fungal infection has HIV negative AIDS. This happens all the time.
ICL is another phoney definition which was concocted to save keep the NIH money flowing for a medical mistake made obvious by the heretical announcement of HIV negative AIDS cases at one of the AIDS meetings. These ICL cases are in reality HIV negative AIDS, and they are not rare, they are quite common.
These are not spurious correlations unless you happen to be a drug company reprentative. Much of what is called AIDS is chronic IV drug, and hard drug abuse in gays and minorities with repeated STD's, chronic antibiotic abuse, etc. Virtually all of Pediatric AIDS is maternal drug addiction, and fetal addiction/withdrawal. The exception being kids like Ariel Glaser who were obviously tragically sacrificed to AZT toxicity. Even though Ariel's death was a tragedy, future deaths from toxic drugs are preventable, and it is no excuse to impose this form of iatrogenic death on other children and mothers in the name of the Eizabeth Glaser Foundation which recives huge amounts of money from the drug companies who make the toxic drugs. This is public information available to anyone.
Again a complete lie from a drug company representative. This article, The Discovery of HIV as the Cause of AIDS by Robert C. Gallo, M.D., and Luc Montagnier, M.D. NEJM. Volume 349:2283-2285 December 11, 2003 Number 24, was supposed to be the one that proves HIV causes AIDS. Ask Adele or Raven if this article is REALLY THE ONE that proves that HIV causes AIDS. It proves nothing. There aren't any articles that prove HIV causes AIDS. There are only evasive lies from the honorable drug company representatives.
This is a disgrace.
For more info; www.reviewingaids DOT com
Same 4 morons who repeat that use this site over and over again. Don't you guys have lives?
Yeah Nicolson and Lo were never debunked, every animal LO injected his mycoplasma sickened and died. You cant debunk someone with an animal model, losers. They have a correlation and an animal model with a microbe thats detectable with electron microscopy in the sick people/ animals.
What do you losers have? A correlation with no reliable animal model ( virtually every animal injected is unaffected), with a microbe that according to your high priest Gallo is present in 1 out of every 10,000 t cells and nuetralized by antibodies.
Im not saying that HIV has nothing to do with AIDS but because of all these paradoxes youd better have some rock solid epidiemology to prove your "species specific" "barely detectable" microbe and there are none that controlled for confounding factors. None of those cohort studies were designed to test the hiv hypothesis, they were designed with the premise that hiv did cause AIDS and were designed totally differently because of that. So don't whine when scientists far more qualified than you are demand some answers.
This is freshman year undergraduate microbiology, and you guys are too dumb to realize it.
Forty neurones,
Leaving aside the amusing contradiction of the following sentence for the moment ("The government of South Africa and other repected people"), I must pick you up on your claim that: "There has never been a placebo controlled study showing any benefit AT ALL from nevirapine.
Well what about:
ISS 047?
ACTG 193a?
ACTG 241?
INCAS?
All of them double blind, placebo-controlled studies showing the benefits of Nevirapine. No doubt I could dig out a few more given more time.
Do we get to hear a grovelling apology, or more hand waving and spluttered excuses?
Just for everyone's reference. I don't work for a drug company. No part of my pay comes from a drug company. I'm actually critical of how drug companies sometimes hype their stuff and pay off doctors. Also how sometimes things get dumped on Africa. I don't defend drug companies I really don't know much about them. I defend good medicine and saving peoples lives with drugs that work and have benefits much higher than side effects.
Billy,
Freshman microbio?
Will you be taking that next year?
Dear Adele,
RE:
"When "Dr. Mantious" writes he humiliates himself by lying about better scientists and what they do. Like when he lied about J. Klausner saying two percent of flu vaccine people testing HIV positive. Another honest mistake I'm sure.
No mistake, see below.....
"Klausner said nothing like that and neither does anyone else whose respectable. We went throw those early 90s papers last week and the flu vaccine probably doesn't cause false + and no way 2%. "Dr. Mantious" told us he would talk about the Klausner thing but he didn't. He changed the subject but then yesterday he brought up flu vaccine AGAIN. Gotta hand it to him, good liars should be shameless. And he is."
PROBABLY DOESN'T you say? Good reason then to launch Salem-style witch hunts against folks like Christine who test 6 different ways, none of which are consecutively positive. I wonder if Christine or any other "HIV-convicted persons" were was tested with:
FDA recalls Abbott Laboratories HIV p24 Antigen Test Kit lot 71843M101.
" The failure to deliver the Antibody to HIV-1 (Rabbit) component of the test kit to the reaction well could result in a false negative test. The recall notification instructs establishments that currently have in inventory the recalled product to discontinue use and discard the product."
2002 (August 7) FDA recalls Bio-Rad Laboratories Genetic Systems HIV1/HIV-2 Peptide EIA lot 105VP1. " The recalled test kits are qualitative enzyme immunoassays for the detection of antibodies to HIV-1 and/or HIV-2 in human serum and plasma, and also in cadaveric serum specimens. Microwell plates in this lot that are performing outside of expected performance ranges as indicated by invalid (low) HIV-1 and HIV-2 Positive Controls and elevated Negative Control values."
2003 (January 6) FDA recalls Abbott Laboratories HCV EIA 2.0 Test Kit lot 92527M101 (4/15/2003). "The manufacturer found an increase in frequency of Negative Control Out of Range High values, which results in an increased likelihood of invalid assay runs... Establishments that have the recalled product in inventory are instructed to discontinue use and destroy any remaining product."
2004 (May 13) FDA recalls DiaSorin's HIV-1 / HIV-2 Plus O EIA Testing Software.
" An error was contained on the ETI-LAB Applications disk for programming the BioRad HIV-1/HIV-2 Plus O assay. The error induced specimen and conjugate incubation temperatures for the assay to remain at ambient temperature rather than the required 37°C temperature."
2004 (May 17) FDA recalls bioMerieux (Durham, NC) NucliSens HIV QT.
" Some irregularities have been observed with one lot's guanidine isothiocyanate (GuSCN) component, which may affect the sensitivity and accuracy of assays."
2004 (June 24) FDA recalls Roche's Amplicor HIV-1 Monitor Test, v 1.5.
" Roche has confirmed increased frequency of occurrence of "blue foci" with the Avidin-Horseradish Peroxidase (AV-HRP) Conjugate Lot E09659. Increased frequency of the occurrence of "blue foci" may lead to elevated and/or observed out of sequence optical density readings in the microwell plate assays that have used this particular lot of reagent."
2005 (January 18) FDA recalls GEN-Probe Inc Procleix HIV-1/HCV Assay.
" Procleix HIV-1 / HCV Assay, Master Lot 401254, was found to contain an elevated level of copper. The source of the elevated copper was the raw material, Trehalose, which is also a component of the Enzyme Reagent. The increase in copper may affect kit performance."
2005 (February 4) FDA recalls Globus Media Inc. Rapid HIV Test Kits.
"Rapid HIV Test Kits, marketed nationwide via the Internet, by Globus Media, were not reviewed for safety and effectiveness as required under U.S. law. Consequently, there is no assurance that the results from these kits are reliable.DO NOT RELY ON ANY TEST RESULT FROM THESE RECALLED KITS. Consumers who have these products should not use them.Consumers who have used the RAPID HIV Test Kit, should consult a health care professional immediately to confirm any results."
2006 (October 6) FDA recalls Home Access Health Corporation (Hoffman Illinois) Home Access and Home Access Express HIV-1 Test System lots 042108, 042109, 042110, 042111, 042113, 052101, 042010, 042011, 042012, 042013, 042014, 042015, 042016, 042017, 052001. "The lancets may not be sterile as of the printed "Use By" date. These lots should have been labeled with a "Use By" date of October 2006. HAHC recommends that these lots be removed from distribution and they will not be able to provide results for any blood specimen collected after October 31, 2006. It isn't clear how aseptically-sealed blood-letting lancets lose their sterility over time."
2006 FDA recalls Vironostika HIV-1 test kit lots:
259606, 121566, 1008926, 259606, 121567, 1008926, 259606,121568, 1008926, 259605,
259717, 160342, 1011220, 259605, 259717,160339, 1011021."These HIV-1 finished kit lots in the field have been reported to contain EnzAbody reagent that appears noticeably cloudy and/or flocculent, instead of clear and non-turbid as expected 30 minutes after reconstitution. Use of cloudy EnzAbody could possibly increase your risk of inaccurate HIV test results in patients and therefore should be avoided."
"Yes I hope Dr. Mantious returns because when he does he also humiliates people who
1) try to exploit the real sufferings of many African Americans and other minority groups for their own pseudoscience ends by lying about "pharma" or "big gubmint" conspiracies to kill black mothers with nevirapine or something so crazy ridiculous it hurts your brain.
You mean like Lockman et al.s trials on 875,000 black mother-infant pairs who now have a 41% resistance rate due to their little nevirapine experiment?
2) ridicule the suffering of some Gulf War veterans by making up crap about how their CAT died of it.
That's papa Bush's and Tremont's doing when he pushed the anthrax vaccine on the Gulf War vets as I referenced before, not mine.
3) cover up their own disgusting ideas about sexuality or race by accusing other people of them.
Really? What is you phone number baby?
Wow! So you found those "HIV" pictures I linked and could actually find an "HIV" particle amongst all the garbage? Care to comment? I ate some RT for breakfast this morning in my fried eggs (didn't you just love that Department of Biological Standards reference to RT I sent being in ALL chicken-derived vaccines?
Still believe chronic drug addition is a good thing for a person and doesn't lead to any immunological problems? Take it one day at a time, Adele, and just don't drink!
I DON'T LIKE CATS and I never said anything about them! They are useful, I suppose for neurobiological experimentation, if you believe the results from Hubel and Weisel that is.
BTW, the name is spelled "Maniotis!" There's no ous in it.
About Simonsen, Klausner-and flu vaccines and phony test kits:
JAMA. 1992 Aug 26;268(8):1015-7.
Multiple false-positive serologic tests for HIV, HTLV-1, and hepatitis C following influenza vaccination, 1991.
Mac Kenzie WR, Davis JP, Peterson DE, Hibbard AJ, Becker G, Zarvan BS. Bureau of Public Health, Wisconsin Division of Health, Madison 53703.
"We estimate between 0.6% and 1.7% of blood donors who received influenza vaccine this season had multiple false-positive viral ELISAs."
Is this plagerism? Distortion? A reason to "roll out drugs" on continents of persons who either are diagnosed without any test kit, or who have one ELISA or repeatedly reactive ELISA's, WB's or PCRs?
Of course its always the 100% accurate test kits fault (the fault of Abbott Labs and their ilk as opposed to the flu vaccine industry! So we should sue the test kit makers, not the vaccinologists?
Am J Epidemiol. 1995 Jun 1;141(11):1089-96.
Multiple false reactions in viral antibody screening assays after influenza vaccination. Simonsen L, Buffington J, Shapiro CN, Holman RC, Strine TW, Grossman BJ, Williams AE, Schonberger LB. Division of Viral and Rickettsial Diseases, Centers for Disease Control and Prevention, Atlanta, GA 30333, USA.
"A case-control study of 101 affected donors and 191 matched controls found that recent receipt of any brand of influenza vaccine was significantly associated with testing multiple false positive (p < 0.05), as was a history of recent acute illness (p < 0.05) and of allergies (p < 0.05). Surveillance for monthly rates of multiple reactive donations from May 1990 through December 1992 linked the seasonal cluster of multiple false-positive donations to the use of viral screening test kits thought to react nonspecifically to donor immunoglobulin M. There was no similar increase in multiple false-positive donations during the 1992-1993 influenza vaccination season after the HIV-1 and hepatitis C virus tests were replaced; however, the number of donations that were falsely reactive for only HTLV-I almost doubled, indicating that false reactivity was not specifically associated with the 1991-1992 influenza vaccine. Retesting of affected donors found that the duration of HTLV-I and hepatitis C virus false reactivity was 3-6 months. The cluster of multiple false-positive donations in 1991 was MOST LIKELY caused by the test kits used, rather than by the influenza vaccine."
What part of the sentence, "recent receipt of any brand of influenza vaccine was significantly associated with testing multiple false positive (p < 0.05), as was a history of recent acute illness (p < 0.05) and of allergies (p < 0.05)" are you having problems with?
It's too bad Andrew didn't read the comments I made on this subject above which completely refute him. I guess he was busy getting a long list of papers about how scientists actually try to improve their tests and fix problems with them.
The conclusion of the vaccine/false positive story by the researchers themselves was that false positives happened in one season was it 90-91? And were from that years batch of HIV tests. They said it was the tests, not the vaccine. Plus no evidence of causation.
All Klausner does is cites Simonsen et al. Since Andrew hasn't read Simonsen et al only looked at a sentence from it he doesn't realize what their conclusion is. See previous paragraph.
I hope Andrew will apologize to Klausner for lying about what he said in his letter to the editor.
There is no good evidence influenza vaccine or rabies has caused any false positives on HIV tests.
BTW It was Andy's 911 conspiracy friend Billy who introduced "Dr. Mantious" to us. Sorry but I thought it's funny.
For those desiring more information about LDN, check out lowdosenaltrexone.org and the moderator for the site is Dr. Gluck, who is very helpful. I have tried to be involved in studies but the NIH is only interested in long-term non-progressors. If anyone knows of any studies being done on those who had AIDS and no longer take the meds, please let me know. It is amazing that no one seems to be interested in such persons, even my own doctors do not do a very good job of questioning me about anything. All they say is to take the meds and I refuse. Nevertheless, they still want me come in every three months because I think that they are curious as hell or they are waiting for me to crash. I am 17 months off of the drugs and finally have some normal reports (blood and liver) for a change. My CD4's have dipped to 86 and at last count were 131 and of course my viral load is greater than 100,000 but what is the most important thing is that I haven't any symptoms since the LDN. From my point of view, it is a no-brainer to stay on LDN and continue to be healthy.
ICL is another phoney definition which was concocted to save keep the NIH money flowing for a medical mistake made obvious by the heretical announcement of HIV negative AIDS cases at one of the AIDS meetings. These ICL cases are in reality HIV negative AIDS, and they are not rare, they are quite common.
I'm going to call your bluff again. Where's your evidence that ICL is quite common?
Go and ask the Health Minister of South Africa for her opinion on nevirapine, or any other toxic drug for HIV, for pregnant black women of South Africa. She and the Prime Minister have rejected these deadly toxic drugs as you should, too. The government of South Africa and others repected people believe that administration of these drugs to pregnant black women is a form of Institutional Racism, and Iatrogenic Genocide.
Go and ask other members of the South Africa government that have had family members die from AIDS what they think of the Unhealth Minister.
YAY!
YAAAAYYY!!!
Spongy Noble answered MY Question! I'm sooo excited.
He said that Aids is TOO FEW blood cells!
That's so good to know.
I'm so happy, that answers a lot, back to you Doctor M.
BUT Spongy and the rest of the fun-time bubble-bunch didn't answer MY question - I mean, they answered my second question, but not my ACTUAL Firstest question.
Which was, What's the pure, particulate standard for any and all H-EYE-VEE tests?
Nobody answers. I'm left all alone to wonder.
No standards, no answers, I'm feeling blue.
I did find this though, which helps me understand a little better. It says that the tests don't matter at all - only the people I use'em on!
"Special Note for Washington State
To minimize the risk of false positive results,
False Positives? What's That!
False positive means that the test result is positive but the client is not infected.
Get the fudge outta here, you crazee kat! What's going on! Positive but not Postive? HAHAHAHAA!
I know they're just kidding...whew! Fun-knee.
The low prevalence of HIV in Washington State means that most testing sites service client populations with less than 1 percent prevalence."
Did you go to sleep? Not yet, here's the part that is tickly:
"In such cases, there is increased likelihood that reactive HIV tests will be false positives."
I can understand that - because blacks and gays and the like, well, they get Aids, right, so it makes sense, uh-huh, that their tests - you followin' me - that their tests ACTUALLY work, but for other people, not so much.
Right? Is that it? It depends on WHO your testing - because the test doesn't really test for anything, does it. I mean, do they?
I think I get it now, thanks for helping me understand our big blue rats-nest.
I love all of you, I hope none of you suffer anything close to what you do to others. I really, really mean that.
Hugs and blouses,
Dear Raven,
of the 57 health care workers who became Hiv positive from occupational exposure, how many came down with AIDS? ZERO. If there had been any AIDS cases in the 57 HIV positives, this would have been reported. 69% of the source patients had AIDS. However no mention of the per centage of the health care workers who had AIDS. Why omit this data? Because the number was ZERO. I saw this article a few days ago when doing the literature search. And try to resist the ad homs, it doesnt become you. Unless of coure you are on the payroll, and are paid per ad hom, like the othe drug company reps here. If you are trying to post a reference that show AIDS from occupatinal exposure, this isn't it. Try again.
SS 047
ACTG 193a
ACTG 241
INCAS
a drug rep said referring to the above nevirapine studies, All of them double blind, placebo-controlled studies showing the benefits of Nevirapine. No doubt I could dig out a few more given more time. Do we get to hear a grovelling apology, or more hand waving and spluttered excuses?
Anyone with the faintest knowldge of these studies knows that NONE of them were placebo controlled. All these studies compared the deadly effects of one drug combo against another. The benefit was that one arm killed fewer people than the other arm. Look it up.
I dont know much about hiv testing, but is there verification that everyone that test's positive has actual virus in them via pcr/culture and that healthy controls dont?
I'm going to call your bluff again. Where's your evidence that ICL is quite common?
Sure, first you provide your evidence, the reference article from one of the 100 links of AIDS TRUTH that proves that HIV causes AIDS.
You provide your evidence, the peer reviewed literature report of thousands (or even hundreds) of health care workers getting occupationally acquired AIDS from exposure to patients with AIDS, and the placebo controlled study showing nevirapine has ANY benefit what-so-ever. You can't because ther aren't any, my pompous arrogant drug company employee. Note: A government CDC report of a few lab workers is not peer reviewed medical literature. Of course we know the government would NEVER lie to us, so that why we need a real report in the peer reviewd medical literature. I looked and its not there.
The primate experiment injecting HIV into human primates (ie health care workers) was a collossal failure, just like the chimps who don't get AIDS, health care workers don't get AID from needle sticks from AIDS patients. They do get hepatitis B in large numbers, NO AIDS though. I've gone through this over and over again, and you still launch ad hominems and fail to provide ANY evidence of peer reviewed medical literature reports. Why not? Because there aren't any.
A drug rep asked me the following question,
do I believe that HIV exists?
Adele says she has seen electron micrographs of HIV, and even used gold particles attached to antibodies to tag the HIV and she is sure she was looking at HIV, and I believe Adele, dont you?
I dont know much about hiv testing, but is there verification that everyone that test's positive has actual virus in them via pcr/culture and that healthy controls dont?
I've already cited this paper in this thread.
Human immunodeficiency virus type 1 detected in all seropositive symptomatic and asymptomatic individuals.
The various "rethinkers" have strategically avoided reading the paper.
Sure, first you provide your evidence, the reference article from one of the 100 links of AIDS TRUTH that proves that HIV causes AIDS.
You've already been provided with a number of papers that all provide strong evidence that HIV causes AIDS.
That you choose to ignore them is not my fault.
You say ICL is quite common where are the papers that provide evidence for this?
The primate experiment injecting HIV into human primates (ie health care workers) was a collossal failure, just like the chimps who don't get AIDS, health care workers don't get AID from needle sticks from AIDS patients. They do get hepatitis B in large numbers, NO AIDS though. I've gone through this over and over again, and you still launch ad hominems and fail to provide ANY evidence of peer reviewed medical literature reports. Why not? Because there aren't any.
I've provided you with peer reviewed articles that have detailed 3 lab works that were occupationally infected with HIV and all suffered CD4+ depletion and full-blown AIDS in on case. So far you don't appear to have read them although two of the articles are free.
I for one am glad that more health and laboratory workers have not been infected with HIV. You seem to support the deliberate infection of humans with HIV.
These incidents were not part of an experiment. They were isolated accidents that were reported. Your rejection of CDC reports is just another ad hoc excuse for ignoring inconvenient data.
Adele says she has seen electron micrographs of HIV, and even used gold particles attached to antibodies to tag the HIV and she is sure she was looking at HIV, and I believe Adele, dont you?
That's hardly a direct answer. If you are trying to appear evasive and dishonest you are doing a good job.
The immunoelectron microscopy technique provides incontrovertible evidence that the virus particles are indeed HIV.
Virology. 1987 Jan;156(1):171-6. Fine structure of human immunodeficiency virus (HIV) and immunolocalization of structural proteins.
I'm yet to hear a halfway plausible excuse from a HIV nonexistentialist about this.
I'm yet to hear a halfway plausible excuse from a HIV nonexistentialist about this.
Gee, Dr. Noble, are you not the one who said one has to understand what one references and demonstrate it by constructing an argument?
But as you wish. For an in depth "excuse about this", how about "that": http://www.theperthgroup.com/
But as you wish. For an in depth "excuse about this", how about "that": http://www.theperthgroup.com/
At no stage do the Perth Group provide a plausible explanation for the immunoelectron microscopy studies. If you can refer me to a specific article then go ahead. otherwise you are just bluffing again.
Dr. Noble, once you've specified exactly what it is that isn't answered "plausibly", preferably with some quotes and commentary - kinda like a real argument. You know what a real argument is don't you?
LDN was something that a doctor in New York City called Bernard Bihari used to promote, back when there were few other options. Naltrexone is used to treat alcohol and opioid dependence. I think the idea is that it promotes a Th1-type immune response. Bihari's data were not great, to say the least, he divided people into "compliant" and "non compliant" groups in order to try and show the compliant group did better. I remember talking to one person back then who swore by it, but I also recall Bihari having a hard time accepting that it wasn't working for people when it didn't. Bihari was generally seen as a little out there, but he in no way denies HIV causes AIDS, and I don't think he had any problem using ARVs, either.
I just looked up his page on the website Noreen mentioned:
http://www.lowdosenaltrexone.org/ldn_hiv_1996.htm
"When naltrexone is used in conjunction with the newer and more potent antiviral combinations, it accelerates immune system healing."
As a side note, the load time on this page is now prohibitive, might be an idea for those with wanting to continue the free-for-all to shift it somewhere else. The HIV vaccines thread, perhaps - not very relevant, but then this thread was supposed to be about smallpox.
Andrew,
I am appalled. You distort the work of other scientists by inventing a "quote" so that you can attribute to them an absurd conclusion, and when it is brought to your attention you assert that the fictitious "quote" is more accurate than authors' own words.
You "quoted" Laurent-Crawford et al. (1991) as saying:
And based on this false "quote" you claimed that Laurent-Crawford (1991) suggested that mycoplasmas may be the cause of the immune collapse of AIDS and that they reported that maximal viral production occurred in the absence of viable cells.
All of these claims are simply false. Laurent-Crawford (1991) makes no mention of a potential role for mycoplasma in the immune collapse of AIDS. None whatsoever. And the paper never claims that virus is produced in the absence of viable cells. Never. You are simply putting words in the authors' mouths so that you can blame them for the distorted conclusions you draw from their data.
When confronted with your dishonesty, you have persistently defended your fictitious "quote," most recently:
The essence of your excuse seems to be that you've repeated this lie so many times that to your ear it has acquired a certain "truthiness," so much so that you claim your made-up "quote" is better than the original:
Andrew, this was not an honest mistake. You have not fused 2 sentences from the paper to construct your "quote". For you to make this claim just emphasizes your lack of integrity because Chris Noble has already pointed out that the source of your "quote" is really Papadoupulous-Eleopulos et al. (1995) Genetica 95: 5-24:
except that you have rearranged the quotation marks in order to attribute the "quote" to Laurent-Crawford (1991).
It is also a transparent falsehood when you imply that this mistake was made in haste as you were responding to a blog from memory. You cut-and-pasted this passage from a manuscript that you wrote and published on the web ("The ABCs of AIDS Denialism," by Andrew Maniotis PhD, dated August 17, 2006). The misattribution of the quote from Papadoupulous-Eleopulos (1995) to Laurent-Crawford (1991) is already present in this manuscript.
Unfortunately, this type of intellectual dishonesty is simply business as usual for you, as anyone who reads through this blog can see. Professor Maniotis, just because you've become accustomed to misattributing quotes and distorting the scientific work of others "many times before" on the pseudoscientific AIDS denialist websites for which you usually write, doesn't make it acceptable behavior.
Your apologies should be directed not to me, but to Laurent-Crawford, Montagnier, and their co-authors, whose work you have belittled. Laurent-Crawford (1991) never claims that viral production occurs in the absence of living cells. That is just Maniotis's terribly flawed interpretation of Laurent-Crawford's data.
Professor Maniotis, you have a PhD from Berkeley, you did a post-doc at Harvard, and hold an academic position at a major American University--yet you don't seem to understand the difference between "accumulation of nucleosomes" and "cell death". Laurent-Crawford (1991) very clearly explain that the earliest cytopathic effects of HIV infection (vacuolization of cells and syncytia formation) occur at least a day to several days before cell lysis, depending on the experimental conditions. They also demonstrate that the accumulation of nucleosomes or, in some experiments, of histones, coincides with these early cytopathic effects. In their description of Figure 1 they report that:
They further demonstrate that the nucleosomal accumulation represents fragmentation of the genome of the host cell and that, as the host DNA becomes fragmented, unintegrated viral DNA accumulates in the cell, as do viral proteins. The picture is characteristic of a lytic viral infection, in which, as the viral genome hijacks the synthetic machinery of the cell to produce new virions, the host cell DNA is fragmented as the cell is forced into the process of programmed cell death.
Because the viral genome has now taken over the cell's biosynthetic machinery, fragmentation of the host cell DNA does not render the cell incapable of producing viral proteins. The cell continues to express the viral genes even after the host DNA has become fragmented. That is exactly why Laurent-Crawford (1991) are so careful to specify "accumulation of nucleosomes" as opposed to "cell death" (the term you mistakenly use).
When they repeated the experiment in the presence of mycoplasma removal agent (MRA), they showed that although the time course of infection was delayed, the early signs of the cytopathic effect still coincided with fragmentation of host cell DNA and the expression of viral proteins still coincided with the accumulation of unintegrated viral DNA.
There is nothing about this experiment that conflicts with well-described cell biological mechanisms, and the results certainly do not violate the logical principle that an effect cannot precede its cause. Descriptions of these types of viral infections can be found in any standard textbook of cell biology used in introductory undergraduate or graduate level courses. For example, you might visit Pub Med to read Chapter 13 of Cooper, GM (2000) The Cell: A Molecular Approach. Second Edition, Sinauer Associates, Inc..
Nothing evasive about it. I believe Adele, dont you?
You and your honorable drug representaatives are the evasive ones. You claim that HIV causes AIDs, yet refuse to point to the articles that prove that HIV causes AIDS. your evasive answer is to go to pubmed. Your evasive answer is to list the NEJM article by Gallo which (as I have extensively discussed) does not prove HIV causes AIDS. Neither Adele, nor Raven , nor kevin nor cooller nor the Pope have agreed that any of the links provided so far proves HIV causes AIDs. Are you trying to hide your secret article? Or are you simply being evasive?
I would really like to be convinced and become one of the "believers" in the HIV causes aIDS hypothesis, just like all all of you honorable drug company representatives.
Just present the links to the referenes that will convince any ordinary person, and I will be convinced. But you can't because there aren't any.
Medical science has never proven that HIV causes AIDS. On the basis of this non-proof, people are being killed by deadly drugs like nevirapine that have never been tested in a placebo controlled drug trial.
People are not being killed by HIV, they are being killed by the HIV drugs, like Ariel and Elizabeth Glaser who were sacrificed to AZT toxicity.
for more info; see reviewing aids DOT com
Forty:
"There has never been a placebo controlled study showing any benefit AT ALL from nevirapine."
DT (In anticipation of frenetic handwaving and goalpost moving):
"Well what about: ISS 047, ACTG 193a , ACTG 241, INCAS?"
Forty (waving hands frantically, hurridley shifting goal posts):
"Anyone with the faintest knowldge of these studies knows that NONE of them were placebo controlled.
You evidently do not understand what placebo-controlled means. It means that a placebo tablet of Nevirapine is given to some patients, and genuine Nevirapine given to others. In these trials, either placebo or genuine Nevirapine was added to a background regimen of 2 NRTIs. The groups receiving genuine Nevirapine all did better.
Question 1: If Nevirapine is a deadly toxin (as you assert) then why should it have improved the outcome of patients taking it? By received denialist wisdom, the groups getting nevirapine should have fared worse.
Question 2: When can we see the single paper to support the denialist claim that thousands of HIV negative drug users have had PCP?
Question 3: Are you capable of answering the above, genuine and specific questions, or will they be ignored as I expect?
Hey folks,
Here is a NEJM article hot off the press RE: needlesticks...Not plagerism, just posting of some relevant article...
Volume 356:2693-2699 June 28, 2007 Number 26
Needlestick Injuries among Surgeons in Training
Martin A. Makary, M.D., M.P.H., Ali Al-Attar, M.D., Ph.D., Christine G. Holzmueller, B.A., J. Bryan Sexton, Ph.D., Dora Syin, B.S., Marta M. Gilson, Ph.D., Mark S. Sulkowski, M.D., and Peter J. Pronovost, M.D., Ph.D.
ABSTRACT
Background Surgeons in training are at high risk for needlestick injuries. The reporting of such injuries is a critical step in initiating early prophylaxis or treatment.
Methods We surveyed surgeons in training at 17 medical centers about previous needlestick injuries. Survey items inquired about whether the most recent injury was reported to an employee health service or involved a "high-risk" patient (i.e., one with a history of infection with human immunodeficiency virus, hepatitis B or hepatitis C, or injection-drug use); we also asked about the perceived cause of the injury and the surrounding circumstances.
Results The overall response rate was 95%. Of 699 respondents, 582 (83%) had had a needlestick injury during training; the mean number of needlestick injuries during residency increased according to the postgraduate year (PGY): PGY-1, 1.5 injuries; PGY-2, 3.7; PGY-3, 4.1; PGY-4, 5.3; and PGY-5, 7.7. By their final year of training, 99% of residents had had a needlestick injury; for 53%, the injury had involved a high-risk patient. Of the most recent injuries, 297 of 578 (51%) were not reported to an employee health service, and 15 of 91 of those involving high-risk patients (16%) were not reported. Lack of time was the most common reason given for not reporting such injuries among 126 of 297 respondents (42%). If someone other than the respondent knew about an unreported injury, that person was most frequently the attending physician (51%) and least frequently a "significant other" (13%).
Conclusions Needlestick injuries are common among surgeons in training and are often not reported. Improved prevention and reporting strategies are needed to increase occupational safety for surgical providers.
Source Information
From the Center for Outcomes Research, Department of Surgery (M.A.M., C.G.H., J.B.S., D.S., M.M.G., P.J.P.), the Quality and Safety Research Group, Department of Anesthesiology and Critical Care Medicine (M.A.M., C.G.H., J.B.S., D.S., P.J.P.), and the Division of Infectious Diseases, Department of Medicine (M.S.S.), Johns Hopkins University School of Medicine; and the Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health (M.A.M., J.B.S., P.J.P.) -- all in Baltimore; and the Department of Plastic Surgery, Georgetown University School of Medicine, Washington, DC (A.A.).
Where are all these dying or dead 55% of 99% of doctors who stuck themselves? Haven't seen too many physicians bodies on my way to work lately.
I know for a fact that universal "HIV" screening within mandatory medical resident training programs has ever prompted a letter of apology to the family of Dr. David Acer, for his committing suicide on the basis of mistaken charges that he spread "HIV" to his patients [1], which the CDC later exonerated him of doing (after his suicide), because the CDC could "find no evidence the dentist's HIV-positive patients contracted their infections from him because their virus' DNA did not match his, and also concluded the dentist's patients did not contract the virus from one another -- in effect, that unclean dental implements did not act as conduits." Other studies that have followed exposure of health care workers have also found no transmission of AIDS [2].
Today's NEMJ article says:
"By their final year of training, 99% of residents had had a needlestick injury;
for 53%, the injury had involved a high-risk patient.
Of the most recent injuries, 297 of 578 (51%) were not reported to an employee health service, and 15 of 91 of those involving high-risk patients (16%) were not reported. Lack of time was the most common reason given for not reporting such injuries among 126 of 297 respondents (42%)."
If this is true, then half of the 99% of last year trainees in medical schools have been at risk of acquiring "HIV," "Hep B," "or "Hep C." As suggested, this figure is probably under-reported for the reasons given. Where are all these AIDS cases? Do they all get "cured" with prophylactic AZT?
I worked with a liver transplant surgeon who this happened to a decade or more ago. Within hours of her exposure, she told me they put her on short-course AZT prophylaxis. She then told me she took AZT for 3 days, became so violently ill, that she threw the pills down the toilet and flushed them away! She never became "HIV," Hep B or C positive.
Perhaps this is because it is known that even huge amounts of "HIV" "virus" (READ SURROGATE MARKERS HERE FOLKS) can be inactivated (NOT DETECTED) within seconds upon IgG binding of "infectious, purified, and highly concentrated "virus":
J Infect Dis. 1996 Apr;173(4):863-9.Links
CD4-IgG binding threshold for inactivation of human immunodeficiency virus type 1.
Berkower I, Mostowski H, Bull TE, Murphy D.
Laboratories of Immunoregulation, Food and Drug Administration, National Institutes of Health, Bethesda, Maryland, USA.
The stoichiometry of human immunodeficiency virus type 1 (HIV-1) inactivation by soluble receptor CD4-IgG hybrid dimers (CD4-IgG) was examined. The extent of HIV-1 inactivation was measured in a sensitive plaque-forming assay, and the corresponding level of CD4-IgG binding was determined by immunofluorescence of infected cells. Ninety percent virus inactivation occurred at relatively low levels of CD4-IgG binding (10% of the saturating level). At even lower binding levels (1.4% of maximum binding), virus survival was 44%. Over a broad range of binding conditions, the survival curve followed a model in which viruses binding more than a threshold level of CD4-IgG were completely inactivated, while viruses binding less remained infectious. The data indicate that CD4-IgG binding to 1.4% of gp120 binding sites equals the threshold for inactivation. Thus, virus inactivation can begin when 3 CD4-IgG (of approximately 216 gp120 sites) bind per virion.
And it is simply appalling that the factor VIII and IX concentrates were said to have killed off the hemophiliac population (who are actually living longer now with "HIV" since the introduction of the concentrates), when it has been know for at least 15 or more years that simple human blood proteins such as serum albumin eliminates "HIV" infectivity upon contact (read-can't get cultures to produce a signal despite PHA stimulation).
Transfusion. 1989 Sep;29(7):629-34.Links
Inactivation of the human immunodeficiency viruses (HIV-1 and HIV-2) during the manufacturing of placental albumin and gammaglobulins.
Grandgeorge M, Pelloquin F.
Department of Research, Institut Mérieux, Lyon, France.
A laboratory study was undertaken to verify the elimination and/or inactivation of the human immunodeficiency viruses HIV-1 and HIV-2 during the manufacture of placental albumin and the gammaglobulins Gamma 16 and Veinoglobuline. Nine steps of the process were selected for study. Samples of current production batches were taken at these different stages and a known quantity of virus was added. Each sample was then processed according to the production schedule for the corresponding step, and the residual viral activity was measured. In eight of nine steps, a complete viral clearance was achieved. Estimation of the cumulative infectivity reduction due to these nine steps is in the following range: greater than 12 to 16 log10 HIV-1 and greater than 17 to 19 log10 HIV-2 for Gamma 16, greater than 9 to 13 log10 HIV-1 and greater than 13 to 15 log10 HIV-2 for Veinoglobuline, and greater than 19.7 log10 HIV-1 and greater than 24 log10 HIV-2 for albumin. As many other purification steps were not included in this study, the real infectivity reduction capacity for the whole process probably exceeds these values. Nevertheless, the levels of inactivation measured clearly document a rigorous fractionation process that has a high assurance of killing or eliminating all contaminating virus.
Also, no embalmers have ever gotten "THE AIDS VIRUS"...
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1350194
Am J Public Health. 1989 October; 79(10): 1425-1426.
Occupational exposure to human immunodeficiency virus (HIV) and hepatitis B virus (HBV) among embalmers: a pilot seroprevalence study.
S B Turner, L M Kunches, K F Gordon, P H Travers, and N E Mueller
Division of Community Health Services, Boston Department of Health and Hospitals, MA.
Abstract
We performed a serosurvey of 133 embalmers in an urban area where human immunodeficiency virus (HIV) infection is prevalent. Although we found histories of needlesticks to be common, and the seropositivity rate of hepatitis B virus (HBV) (13%) was approximately twice that of a blood donor comparison group, HIV antibody WAS UNIFORMLY ABSENT in 129 embalmers who denied HIV risk factors, and present in one of four with self-described risk behaviors. The risk of HBV infection was higher among embalmers who have worked more than 10 years, relative risk (RR) 16.2 (95% confidence interval 2.1, 126.5), did not routinely wear gloves, RR 9.8 (CI 3.4, 28.5), or are employed in the city of Boston, RR 4.7 (CI 1.8, 12.0).
1. Ted Anthony. STUDY: HIV not contracted from dentist. Associated Press, Thursday, December 1, 1994. ww2.aegis.org/news/ap/1994/AP941233.html
2. Hirsch MS, Wormser GP, Schooley RT, Ho DD, Felsenstein D, Hopkins CC, Joline C, Duncanson F, Sarngadharan MG, Saxinger C et al. Risk of nosocomial infection with human T-cell lymphotropic virus III (HTLV-III).N Engl J Med. Jan 3;312(1):1-4, 1985.
Franklin,
the only explanation I have is, Andrew is a pathological liar. He wrote J. Klausner "emphasized" 2 percent of flu vaccine recipients test HIV false positive. After we confronted him with the evidence he was wrong he repeated it.
J. Klausner never wrote that. Klausner's references didn't write that. Andrew is lying.
The first studies in 1991 said 0.6 to 1.7 percent of flu vaccine recipients were testing false for several ELISAs. The conclusion to all these studies was test kits were to blame and flu vaccine wasn't itself causing false positive. The problem was in one season, anyway.
Andrew is the kind of "agenda-scientist" who takes a sick kid, maybe with asthma or depression or something, and tells her parents, oh, it was definitely that flu vaccine you gave her last fall or maybe the MMR she had when she was a baby. Who cares about cause and effect or proof.
In fact Andrew thinks HIV science or vaccine science switches effect and cause. But for great Galileos like him there is no such pesky restriction,
The physicists gave up on causality in the 1930's and replaced that kind of primitive thought process with dynamical systems and quantum mechanics. I suggest you read some history of science.
Andrew's words, not mine. He's above "causality". For Dr. Maniotis, a vaccine is the cause of every childhood illness, no proof required. Drugs are the cause of all AIDS, no proof required. And that's good for him because there isn't any proof for his feeble-minded woo.
Just commented past another lie-avalanche from Maniotis.
In the little Maniotis book of logic, some doctors get stuck with needles, therefore if HIV causes AIDS and can be transmitted, 55% of doctors should die on the road on Andrew's way to work. Where are all these dying or dead 55% of 99% of doctors who stuck themselves. Haven't seen too many physicians bodies on my way to work lately.
He cites a paper where a grand total of 15 recent respondents did not report a needle stick from a "high-risk" patient.
It's called hyperbole. Andrew starts with "55% of 99% of doctors" have a needle stick from a "high risk" patient. Then he assumes, lets look at this,
1) All high risk patients have HIV, NOT!
2) They all have viral loads high enough to transmit via needle stick, NOT!
3) All needle sticks are equally likely to transmit a virus NOT!
4) All doctors stuck with a needle get infected NOT!
5) No one gets prophylaxis NOT!
6) 55% doctors get infected and immediately seroconvert and die of AIDS. NOT!
In the real world, medical workers get drugs to help prevent transmission of HIV. Andrew knows one woman who threw up and threw away her pills. Well I know one who didn't and took her whole course of pills and was fine. Anecdotes are crap, Andrew. The studies show prophylaxis prevents transmission and HAART prevents AIDS. That's why there were more needle-stick transmissions and AIDS cases in the first decade of AIDS than since HAART came out.
Some info for the Maniotises of the world:
1 in appx 350 needlesticks from a known HIV positive source will result in HIV infection.
1 in appx 3000 mucosal exposures from a known HIV positive source will result in infection.
In a population with 1% HIV seropositivity, the chance that a random needle stick injury will result in HIV infection is appx 1 in 35 thousand.
In the same population, the chance that a random blood-to-mucous membrane exposure will result in HIV infection is appx 1 in 3 million.
A single drug (AZT) cuts the risk of infection by 80% in those who are exposed to HIV.
Regarding your referenced study of embalmers:
Embalmers usually get skin or mucosal exposures, with percutaneous injuries being less frequent. The 14 of 133 embalmers who had Hepatitis B markers stated they had experienced a needle stick, but we don't know how many of the remainder ever had a needle stick - the study mysteriously does not tell us. We also don't know how many "AIDS" cases were actually embalmed - the embalmers' recall is obviously imprecise (a selection of embalmers from Boston recalling they had embalmed more AIDS cases than there had been AIDS deaths reported up to that date in the entire state of Massachusetts), and no comment is made on whether any needle sticks actually occured with any of these "AIDS" cases. My guess is that if they knew which were the "AIDS" corpses (and they say they did), they'd be more than a little careful when waving around their infusion cannulas.
The fact that none of the 129 embalmers without other risk factors have not acquired HIV from their occupation is merely a statistical irrelevancy. What are you trying to prove by citing this study? Your inability to find pertinent references to support your claims?
Adele my love,
RE: Distorting Klausner:
Something important you missed in math, and the Klausner article. 1.7 rounded off is about 2. When I was young, they taught us to always round "up" in the higher math classes of elementary school. Maybe you suffered from "the new math?"
RE: ad hominem:
I'm not a pathological liar-I'm a homeopathologist as Robster (that nameless professor who is afraid his students might see what he does when he isn't at his day job) dubbed me.
RE: Needlesticks and todays NEJM article and my post on it:
There is no doubt that doctors die of AIDS related issues. Look at David Acer. He couldn't beat his "high risk" stigmatization, so he committed SUICIDE. So it is clear that "HIV" causes physicians to sometimes die, as it does the countless unfortunates whom they brow beat into believing they are "HIV" infected.
Robster, Franklin,
Much more later about the mycoplasm removal agent issue when I have time-I'll spell it out for you and explain why it is an artifact of culturing because the cultures were all stimulated with IL2 and PHA-causing nucleosomal fragmentation IN both "infected" and in CONTROL CULTURES. I suppose Montagnier felt he should report it anyway, although both his controls and experimentals acted the same way, which might explain why effect preceded cause in this experiment. I'd like to get away with that sometime in the peer reviewed literature: show that both the experimentally infected and control cultures exhibited the same result!!
Suffice it to say for now, my reference to this paper and the way I described it was and is appropriate in the context of any discussion re: mycoplasm association to AIDS, cell culturing, cause and effect, and viral assays, especially since Montagnier's patient 1, and all of the work based on Patient 1's and others during this period of "LAV" or lymphodenopathy ASSOCIATED "virus" beginnings, must be proudly accepted with the knowledge that the "isolates" (especially from patient 1) were obtained from a man with lymphadenopathy, who had been treated the year before for syphilis, twice for gonnorhea, he had herpes 1 and 11, plus cytomegalovirus.
RE: Finding "THE" article that proves "HIV" causes "AIDS:"
I posted it above, but here goes again:
Barre-Sinoussi, F,m J.C. Chermann J.C., Rey F., Nugeyre MT., Chamaret, S., Gruest J., Dauguet C., , Axler-Blin C., Vezinet-Brn F., Rouzioux, C., Rozenbaum R., & Montagnier L. 1983 Isolation of a T-lymphotropic retrovirus from a patient at risk for Acquired Immune Deficiency Syndrome. Science 230: 868-871).
All of you are wrong about "HIV/AIDS" being a disease of too few or too many lymphocytes, or ICL without "HIV." It has become clear that "HIV" really attacks the liver (and wastes the muscles by infecting mitochondrial DNA).
Bica et al., "End-stage liver disease is now the leading cause of death in our hospitalized HIV-seropositive population."
Clinical Infectious Diseases 2001;32:492-497
© 2001 by the Infectious Diseases Society of America.
CHEERS,
ANDY
DT,
Wow! 1 in appx 350 needlesticks from a known HIV positive source will result in HIV infection
Wonder how that figure was arrived at. Do you know? I advise you to think before you answer, you just might shoot yourself in the foot.
Please excuse my error, and thank you for correcting my mistaken impression that a placebo pill was intended to contained inert ingredients with no pharmacologic activity. As you say, a perfectly good placebo is one that contains two deadly, highly toxic NRTI's (DNA poisons).
On the other hand, perhaps there is a slight flaw in this thinking about toxic placebos. Sorry to have to be so rude, as to contradict your flawed thnking, but we must insist on the old fashioned placebos with inert ingredients, you know, the ones that don't kill the patient.
Adele,
Youve repeatedly come off as a health care professional, a tech that works pcr's from time to time. I came Across an Adele and Dale on a website at Utah state university. THis ADele is not a scientist at all, just the husband of a scientist named Dale, is this you?
If not do you have any proof of your credentials?
http://www.usu.edu/fchd/cdlab_youngs.cfm
Im pretty sure this is you..................................this is hilarious if its true! LOL
cooler,
As part of the Zionist 911 conspiracy to wipe out Ruby Ridge black helicopter enthusiasts with mycoplasma, I think you're asking a valid question that deserves a fair answer.
Here is a copy of my full c.v. for you to check out although I took my address out since I don't want you harassing my kids.
PS I don't live in Utah.
hahahahahahahahaha
LOL
Where's your credentials that youre a scientist?
Cooler,
I think you're on to something. Dale 's gotta look something like that, and you've definitely got Adele's age right.
Spongy Noble,
Thank you for posting that paper, it's interesting, I'll read it with attention.
http://jcm.asm.org/cgi/reprint/28/1/16?view=long&pmid=2298875
I have a question though.
If there was no standard for testing before the paper was published, and there is no standard after the paper was published, then, and I really am a little confused here,
then what the fun does this mean:
"Our results indicate that HIV-1 can be isolated from 100% (56 of 56) of AIDS patients, 99% (87 of 88) of ARC patients, and 98% (259 of 265) of HIV-1 antibody-positive asymptomatic individuals. "
I mean, it's nice that they can find.. .well, that's the question - what is it they're finding, if they don't have a standard to know what it is they're finding?
And they can find the bits, from - and what is it that they mean by isolation, because I looked up the piece, and there are no pictures, but when I went to disneyland, I DID take pictures of Mickey and Donald -
Do you know why Mickey Mouse divorced Minney Mouse, by the way?
Anyway, I took pictures, and there was Mickey, so I guess I sort of isolated him, I mean, there's a standard - well - is there a standard Mickey Mouse? That's a good question, but they sure own the copyright, I found that out the hard way.
Anyway.
They say that they can find some thing in 98 percent of people who test no-standard hiv test 'positive' - now, is that positive in a high risk group, or a low-risk group?
Or, what was the risk activity of the people in the group?
So, you can't quite find it in everybody, which is good, because if you did, then you'd probably have to be able to isolate it, with pictures -
and by the way, they go on to say, that this really settles the game:
In summary, we were able to definitively demonstrate that HIV-1 infection is present in all HIV-1 antibody-positive adults, regardless of clinical status, by using a sensitive
culture or PCR assay for detection of the virus."
"Certainly the argument that HIV-1 is not the cause of AIDS because it is not present in all HIV-1-seropositive AIDS patients is no longer tenable."
"This large study confirms earlier reports that all HIV-1 antibody-positive adults are at risk for the development of AIDS. In addition, recently licensed serum antigen tests for HIV-1 appear to have limited utility in the direct detection of HIV-1 in antibody-positive patients."
So, they say that all no-standard test 'hiv' reactive high risk group negros and gays, drug users and the like, are 'at risk for the development of AIDS."
And then the the tests suck - I mean, you know, 'appear' to have limited utility of HIV.
So, what the f--- does all of this mean?
The good news for me is that the tests still have no standard - but how can you isolate somthing that you have no standard for, and that doesn't match the tests you use to test for it?
Help! I'm running a clinic in Australianus, and my Aboriginal populations Need To Know how long before I kill them with the life-saving drugs.
Please help!
No standard, so what's isolation?
I'm still waiting....
Question 1: If Nevirapine is a deadly toxin (as forty moos says) then why should it have improved the outcome of patients taking it? By received denialist wisdom, the groups getting nevirapine should have fared worse.
Question 2: When can we see the single paper to support the denialist claim that thousands of HIV negative drug users have had PCP?
DT,
I fear you will wait until the Moon spirals into the Earth if you truly expect an answer. The denialists have no answers, only criticism, hatred, and illogic. I recently told my wife about this website and the denialists who frequent it. Her response was, and I quote verbatim, "Do all mental institutions give their patients access to the Internet?"
Of all the multiply-fallacious points raised by our entertaining friends, the insistence on a "single paper" is by far the most instructive to me. I once read somewhere--unfortunately I have forgotten just where--a comparison of science to a trial by jury. A jury foreman who asked for the "single piece of evidence" that established a defendant's guilt would be laughed out of the courtroom, and justifiably so. Of course, the denialists you debate on Aetiology would never make it onto such a jury in the first place. At the acceptable risk of offending the few denialists who are upstanding members of our society, denialists have proven themselves again and again to be sociopaths: religious extremists, the political fringe (left and right), racists, homophobes, the conspiracy-obsessed, quack profiteers off the misery of their fellow humans, plagiarists, pedophiles, the list goes on. We could no doubt find such individuals in any section of society, but it seems to me that the denialists have achieved a remarkable concentration of the despicable dregs of humanity within their ranks.
But back to the trial analogy: the guilt of a defendant is not settled by a single piece of evidence, not even an admission of guilt. What surveillance video could not be faked? What confession not coerced? What DNA test not tainted or swapped? Unless every member of the jury was physically present at the crime scene, what jury could possibly pronounce a verdict with 100% certainty? This is why many people oppose the death penalty, a punishment that, if unjustly applied, can never be reversed.
Yet the law allows conviction when guilt is established "beyond a reasonable doubt." As the evidence piles up and the jury deliberates, conclusions are reached and the law acts upon them.
When the first descriptions of AIDS cases were published, theories abounded. As Tara Smith mentioned earlier, almost every theory that denialists have cultivated for two decades was rigorously proposed and examined in the first years of the epidemic. These studies proved beyond any reasonable doubt that the causative agent was transmissible by blood and by sexual contact. They proved further, and again beyond any reasonable doubt, that drugs, the various herpesviruses, and other proposed agents did not in fact cause AIDS. They indicated that the agent was a virus, not a fungus or a bacterium. This was the context in which Montagnier's and Gallo's groups published their evidence on what we now call HIV.
Did these early papers prove that HIV causes AIDS? I suppose the answer would depend on where one places the bar of "reasonable doubt." Many "jury members" were convinced, but others waited for more evidence. As the next few years passed, the number of papers supporting the hypothesis rose into the thousands.
The very scientists who had championed other theories of AIDS pathogenesis, that is, those who had the most to lose, in terms of funding, prestige, and even self-respect, were they to agree with the HIV hypothesis--within a short period of time, these very scientists almost unanimously agreed that HIV caused AIDS beyond any reasonable doubt. The consensus that emerged between 1980 and 1985 or so cannot be explained by conspiracy theory, at least not if one knows a scientist or two. Forcing an entire generation of scientists, against their will and against their better judgment, to agree on anything, much less a fallacy, would be impossible. The only explanation for the consensus is that thousands of scientists evaluated the evidence independently and came to the same conclusion: HIV causes AIDS.
Remarkably, those very few scientists who later dissented were and are, without exception, outsiders. They did not and do not study lentiviruses. As such, their qualifications to evaluate the evidence are substandard. The recent Australian trial of Parenzee brought this issue to the forefront when the Judge pronounced the defense "experts" of the so-called Perth Group to be unqualified to offer expert testimony.
Never in the history of the legal system has such a volume of high-quality evidence been presented by a prosecution team as HIV/AIDS scientists have accumulated against HIV. Rarely (although I'm confident many lawyers have horror stories to tell) has a defense team concocted such a cockamamie, logic-twisting, obviously false explanation as have the misfits of denialism.
There will always be those who deny the validity of a verdict. When I travel abroad, usually in continental Europe, unfortunately, I am always sure of one constant: seeing "Free Mumia" posters in Rome, Vienna, Berlin, Paris, Bern. The obsession with this one case has puzzled me. Why Mumia and not some other death-row inmate? I happen to think Mumia is guilty, although I don't think he should die. But I admit, the evidence against him, in fact, the evidence against any defendant, is nothing compared with the scientific evidence against HIV.
HIV is guilty as charged, beyond any reasonable doubt.
Nothing evasive about it. I believe Adele, dont you?
Yes, it is evasive.
I do believe Adele but that is not the reason why I accept that HIV exists. I base my view on a number of papers that have been written including the early paper by Hans Gelderblom that I cited.
You and your honorable drug representaatives are the evasive ones. You claim that HIV causes AIDs, yet refuse to point to the articles that prove that HIV causes AIDS
Your language displays your pathological thinking. What I and several others have given you are a number of papers that all a) provide strong evidence that HIV causes AIDS and b) provide strong evidence that various "alternative" theories about AIDS are incorrect.
Your insistence on an "ultimate" proof is just part of a long pattern of moving goalposts. With any single paper that you are provided with you will invent some silly excuse for ignoring the whole paper and move the goalposts again.
It's a typical "Denialist" game. You sit back and insist that other people prove something to you. Meanwhile you provide no evidence for any alternative explanation or even demonstrate that you have the vaguest understanding of the evidence. You won't even make an honest statement about your viewpoint.
Nobody can "prove" anything to you. This is more a reflection of your igornace and delusional thinking than any weakness in the evidence.
Dear ElkMountainMan,
Science isn't law and doesn't work on reasonable doubt. It works by hypotheses, drawing up experiments, testing the hypotheses directly by more experiments, revising the hypotheses, etc. During the 1940's you will find all textbooks regarding human chromosome numbers to have been wrong, and only later, was the diploid number found to be the 46 it is thought to be today. Didn't matter that every scientist in the world believed there was 48: one observation, after improved karyological preparation procedures, changed everything. Just because 1,000,000 papers are published based on the premise that cancer is "a genetic disease" doesn't change the fact that when you put the most malignant cancer cells (melanomas for instance) into an embryo, the highly aneuploid, genetically screwed up cells form normal dorsal root ganglia and other neural crest-derived tissue. The genes and genetic defects don't drive the cancer-the environment the cells find themselves in, in this case the embryo, does.
Similarly, one cannot ignore any data...as do the AIDS apologists. When scientists publish things like:
The Veterans Affairs Cooperative Study Group reported that "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians," [1] one can't ignore it.
Or when it is published that children born to ZDV-treated mothers "are more likely to have a rapid course of HIV-1 infection compared with children born to untreated mothers, as disease progression and immunological deterioration are significantly more rapid and the risk of death is actually increased during the first 3 years of life" [2] one can't ignore it.
Or when the announcement of the Concorde study reported:
"The results of Concorde do not encourage the early use of zidovudine in symptom-free HIV-infected adults. They also call into question the uncritical use of CD4 cell counts as a surrogate endpoint for assessment of benefit from long-term antiretroviral therapy," one cannot ignore it.
It gets dicey, however, when legal mandates are directed by pseudoscientific beliefs or junk science. This is the case with "HIV" and AIDS. Even Gallo realized that one of the two first AIDS defining diseases wasn't caused by "HIV" nor could it be explained by "HIV:" Kaposi's sarcoma.
In the case of parents, like Christine Maggiore, who test 6 different ways for "HIV" (inconclusive, positive, inconclusive, positive, negative, and positive), and her daughter dies 36 hours after a reaction to a drug that causes up to 10% adverse reactions in some studies and constitutes the reason that physicians usually ask you if you are allergic to penicillins as their first question, and then the state tries to take your other child away and threatens to file criminal charges against you and your "HIV" negative partner of 12 years because it considers you "HIV" positive based on the 6 inconsistent tests, and then calls in a person like Ribe (see below) to resolve the case in favor of "the establishment view of a disease syndrome, then you got a society, directed by junk science and dangerous Nazi-like human experimenters, calling the shots, rather than science or even common sense.
AUGUST 15 - 21, 2003
Web of Deceit
Murder conviction overturned because D.A. withheld evidence
by Jim Crogan
A state appellate court has overturned the murder conviction of Jose Salazar for killing an infant girl in 1996, ruling that the L.A. County District Attorney's Office deliberately concealed information from the defense about a deputy coroner's mistakes, his altered findings and changed testimony in other homicide cases.
The case against Salazar had focused on the timing of the child's injuries. Since that timeline was in dispute, and no forensic evidence or eyewitness tied him to the crime, the appeals court determined that the introduction of Deputy Coroner James Ribe's credibility problems would likely have produced a different verdict.
The unanimous decision was handed down last week. The three-judge panel also ordered the case returned to the trial court. But the District Attorney's Office has not yet said if it will retry the case. The 2nd Appellate District underscored its anger at the D.A.'s Office by publishing the opinion, meaning it can be cited as a precedent by defense attorneys, and naming names of the offending parties.
Gail Harper, Salazar's appellate attorney, said the oral arguments in June signaled victory. "The judges patiently listened to me. Then they challenged the deputy attorney general, representing the D.A., to explain why sanctions shouldn't be issued for this deliberate Brady violation."
Under the U.S. Supreme Court's 1963 Brady v. Maryland decision, prosecutors must turn over potentially exculpatory evidence to defense attorneys. Withholding such favorable evidence violates a person's right to a fair trial. "The D.A.'s Office has this 'win at any cost' attitude. Publishing it and naming names is the only way you get these folks' attention," Harper says. "They don't give a damn about their legal obligations. I hope attorneys in other Ribe cases are lining up to file appeals."
Salazar was sentenced to 15 years to life for killing Adriana Krygoski. He volunteered to watch her while the babysitter went shopping. He was the boyfriend of the sitter's daughter and lived with them. Witnesses testified that the child had two visible head bruises when her mother dropped her off, but otherwise appeared to be healthy. The toddler then hit her head on a coffee table while Salazar's girlfriend was with her.
When the infant awoke from her nap, she started vomiting. Salazar said he tried to help, but eventually called 911. At the hospital, doctors discovered two skull fractures. Ribe testified that the injuries were consistent with violent shaking or hitting a flat surface. The injuries, he said, would have rendered Adriana "instantaneously" unconscious. Without treatment, death would have followed within a few minutes or a few hours. The defense's medical expert strongly disagreed, arguing that the injuries could have occurred hours earlier. But Ribe's timeline focused suspicion on Salazar.
Prosecutors intentionally withheld information about Ribe's inconsistent testimony in other child-death cases, particularly the 1995 beating death of 2 1/2-year-old Lance Helms. The issues in that case closely match those in Salazar's.
In the Helms case, Ribe testified that death occurred within "30 to 60 minutes" of his injuries. The boy's mother, Eve Wingfield, was with him when he died. Wingfield's public defender then persuaded her to plead guilty to a lesser charge of child abuse. Ribe later changed his mind and told detectives the boy died immediately after the beating. The LAPD reopened the case in 1996 and charged Helms' father. David Helms was convicted of murder, and Wingfield was released. An appeal is pending, and Harper says the appellate court requested she investigate potential Brady violations in that case.
The appellate court also highlighted other Ribe cases. At the 1996 trial of Roberto Cauchi, for the torture-murder of a child, Ribe changed his earlier preliminary-hearing testimony, introducing unexpected evidence of sexual abuse and "shaken baby" syndrome. In the 1996 gunshot-murder trial of Sean Hand, Ribe changed his preliminary testimony about the wounds and time of death. In the 1996 trial of Charles Rathbun, Ribe changed his conclusion on the cause of Linda Sobek's death from inconclusive to strangulation. In the 1996 "shaken baby" death trial of Destiny Jacobo, Ribe admitted missing two bruises and changed his conclusions about the time of death. In the 1997 stabbing-death trial of Lorrie Tuccinardi, Ribe changed his testimony about the wounds. At a 1997 preliminary hearing for Edith Arce and Rene Urbano, in a child-murder case, Ribe testified that he changed his mind about a bruise, saying it came from a blow, not a bedsore.
Appellate Judge J. Gary Hastings wrote, "The duty of disclosure [exculpatory material by prosecutors] does not end when the trial is over." Hastings also detailed the efforts taken by Deputy D.A. Jennifer Turkat, who prosecuted Salazar; her supervisor, Alan Yochelson; his supervisor, Roger Gunson; and the D.A.'s Office to stonewall Salazar's defense, Harper, and even Deputy D.A. Dinko Bozanich, the prosecutor of the Arce/Urbano case.
Ultimately, it was Bozanich, a veteran prosecutor, who exposed this web of deceit. In 1999, he gave Harper an affidavit on his investigation into Ribe and the D.A.'s repeated failure to disclose exculpatory evidence. In his opinion, this revealed "intolerable and unethical practices at the highest levels of our office."
Harper says it was Bozanich's stand that helped her discover the truth. And Gigi Gordon, a veteran defense attorney and acknowledged Brady expert, says, "Dinko is the real hero here. He broke the code of silence inside the D.A.'s Office."
Bozanich says he only did what prosecutors must do ethically. "What happened here sends an awful message to young prosecutors and the public," he explains. "When prosecutors do something wrong, sanctions should follow." Bozanich says it's evidence of a "just win, baby" philosophy that developed during Gil Garcetti's tenure. "I'm sorry to say, nothing has changed under Steve Cooley."
But Lael Rubin, a special counsel to D.A. Cooley who helped establish his office's Brady Policy and Alert System for prosecutors to check out witnesses, insists things are better. "If the office had our Brady policy in place prior to December 2000, this case would have been handled very differently."
But the Cooley administration has been in office for two years, and it could have told the court that Garcetti's position was a mistake. Yet it didn't. "We just got the Salazar decision this week," responds Rubin.
And what of the Brady Alert System? Is Ribe's name included? "No, I don't think so," she answers. "Our system is not totally complete."
1. JD Hamilton et. al. and the Veterans Affairs Cooperative Study Group. A controlled trial of early versus late treatment with zidovudine in symptomatic human immunodifficiency virus infection." New England Journal of Medicine, 326: 437-434, 1992.
2. de Martino et al., Rapid disease progression in HIV-1 perinatally infected children born to mothers receiving zidovudine monotherapy during pregnancy. AIDS. 13 (8):927-933, May 28, 1999.The Italian Register for HIV Infection in Children. AIDS, 13:927-933, 1999].
3. Seligmann et al., Concorde: MRC/ANRS randomised double-blind controlled trial of immediate and deferred zidovudine in symptom-free HIV infection. Concorde Coordinating Committee. Lancet, Apr 9;343(8902):871-81, 1994.
Or when it is published that children born to ZDV-treated mothers "are more likely to have a rapid course of HIV-1 infection compared with children born to untreated mothers, as disease progression and immunological deterioration are significantly more rapid and the risk of death is actually increased during the first 3 years of life" [2] one can't ignore it.
Nobody is ignoring this study. It's been cited 38 times.
On the other hand Denialists are continuously misrepresenting these studies. Maniotis fails to mention that treatment with zidovudine during pregnancy reduces the number of children born with HIV. Among the babies that are infected with HIV despite zidovudine treatment during pregnancy there was a higher proportion of rapid progression.
The evidence suggests that this is due the zidovudine treatment reducing the number of intrapartum infections compared to in utero infections. In utero infections are known to have a higher rate of disease progression.
The only question left is why does Maniotis keep on citing references that don't actually support his claims?
The Veterans Affairs Cooperative Study Group reported that "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians," [1] one can't ignore it.
You'll have to forgive my doubt but is this an actual quote from the paper or a Maniotis construction?
Should I go to the library and check?
By a weird coincidence I found the "quote" without the quotation marks on an indymedia comment by a "Robert Gallo".
"Its been about 10 years since the announcement of the Concord study reported in The Lancet that AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians:..."
Re: Chicagoland Premieres "The Other Side of AIDS," continuing censorship, pharmacogenecide, not "HIV" stupid!
In another comment "Robert Gallo" writes:"Forgive me for using the pseudonym (Robert Gallo), but my family and I have been targetted here in Chicago by folks who have gone to long lenths to ruin me, and for all intents and purposes, have not yet succeeded, although my tenure was denied at my University on the basis for my views and lectures against the "HIV-AIDS" insanity (yes, I really am a sort of famous scientist that can't spell). But they have not shut me up, or put my science out of business, although I am barred at the University from teaching medical students (they still allow me to have graduate students and post-docs). So please forgive my caution."
However, the use of antiretroviral therapy is now associated with a series of serious side effects and long-term complications that may have a negative impact on mortality rates. More deaths occurring from liver failure, kidney disease, and cardiovascular complications are being observed in this patient population.
www.nih.gov/about/researchresultsforthepublic/HIV-AIDS.pdf
Dr Noble, notice that little three letter word fourth from the end of the first line, what does that mean?
Does it mean that previously there were no problems with serious side effects, that "might have a negative impact on mortality rates" (you gotta love the way these guys word it), but now (Oct. 2006) there are?
Or does it mean, previously we didn't really want to admit it, but now we can't afford to ignore the problem any longer?
Or is there another explanation, perhaps one involving a "working definition of intrauterine and intrapartum transmission" and lots of "mights" and "ifs", like in de Martino et al's obligatory attempt to explain away failure?
Dear Dr. Noble,
You research steel building beams (I saw that, as an assistant professor in Australia, you have first authored 4-5 papers on the subject during your career)?
Because you have shown such deep insight in this (as well as countless other blogs) on the subject of AIDS, and I am assuming this is you I found, and you are not by chance the Chris Noble of Hamilton Heights High School Fine Arts Department Head, who commented on Ryan White's funeral, could you please speculate using your first-hand knowledge of human diseases and pathology as to the causes of:
Hemangiomas,Kaposi's sarcoma, or Kassabach-Merit phenomenon, and how the pathogenesis of these various cancer-like syndromes differ due to their different aeteologies?
Would you care to comment on the cause of Alzheimers?
Multiple sclerosis? This should be an easy one.
Diabetes type I or II? Do you know the cause?
Rheumatoid arthritis? What is the cause?
Herpes in the eye or brain when there can be found no herpesvirus particles present in the inflammations, according to all of the neurologists who write on the subject?
The causes of any symptoms in secondary or tertiary syphilis in either untreated or inadequately treated primary patients?
Cause of asthma?
Cystic fibrosis.
Neurofibromatosis?
Parkinsons? Just the cause.
Hematology's long-standing problem of why immune reactions are evoked after transfusions in the absence of the predicted necessary immune responses.
I can think of many many more issues that you can kindly provide us the cause(s) of.
Hepatitis B? (How does the cellular damage occur in livers of humans or chimps perfused directly with hepatitis b patient sera, or mice (or humans for that matter), and how does hepatitis b lead to cancer 40 years later when no cellular changes in the livers consistent with transformation or even damage can be detected?
Why did Pasteur need to give cranial injections to his dogs to insure 100% infectivity in his animal model, when only half of his dogs would acquire it through IV infusions? Could it have been the Joseph Meister, like the 50% of rabies-resistant dogs, would not have developed full blown rabies also?
If your research into steel building reinforcements has provided you with such insights into AIDS, AIDS-related cancers, the immune system (you don't have to be a retrovirologist to have relevance to the subject of Acquired Immune Deficiencies-and those who claim this "expertise to be necessary are only being intellectual snobs), then surely, then I do implore you to perhaps apply to my department (I have some influence here), and
Thank you, and in anticipation,
Cheers,
Andy
Notice how the honorable Dr. Chris Noble (doctor of what? steel beams?), the self proclaimed HIV expert, uses typical political activist tactics. He evades the bulk of Dr. Maniotis comments and uses tricks and gimmicks. Why can't you answer all of Dr. Maniotis comments, Dr. Noble? Stop playing games like a paid drug company hack, and get to your point if you have one.
The facts remain Dr Noble, you have not explained to us the mechanism by which HIV causes AIDS, because there is none, just as there is no animal model of disease, no placebo controlled study of the current toxic drugs for HIV, nor a gold standard for the HIV test kits. A simple selenium pill for a nickle has been shown more effective than the toxic drugs you peddle.
You have not yet admitted your mistake, and you haven't apologized for the 300,000 gay drug users whose lives were terminated by the toxic drug, AZT, while they were betrayed by the medical system they trusted.
You have not apologized for the mistake of Dr. Ho "Hit em Early, Hit em Hard" excessive use of HAART toxic drugs for HIV, based on flawed research. Even John Moore himself, the self proclaimed AIDS political advocate (funded by big Pharma) admits this was a mistake.
You haven't apologized for the scientific misconduct and outright fraud at the NIH involving the nevirapine trials in Africa brought to light by whistle blower Dr. Jonathon Fishbein who was rewarded for his honarable deeds by being fired from his job and ostracized.
You havent explained that long term non-progressors have HIV and don't get sick, and giving toxic drugs to these people will only harm them for no reason. You haven't explained why the NIH or the CDC hasn't a clue as to why some people are long term non-progressors or how many of these people are in the population. What if a pregnant mother has HIV and is a non-pregressor? If she correctly refuses toxic drugs, her baby is taken away by a social agency. This is a disgrace.
After all these "mistakes", you are now asking people to trust you and your toxic drugs again? Why should they. Why don't you take your toxic drugs and self administer them as a rectal suppository, Dr Noble, you repulsive, arrogant, pompous drug peddler.
Why should anyone take you or your toxic nevirapine drug trials seriously after it was banned by the CDC, and after revelations of scientific misconduct and fraud involving the NIH nevirapine trials by whistle blower Jonathon Fishbein? You are asking for our trust after betraying our trust.
I have never claimed that thousands of HIV negative drug users have PCP pmeumonia as you have falsely ascribed to me. However, according to the source linked below, drug addiction is a well known predisposing factor for PCP pneumonia and immune suppression ; here is the entire list,
High-risk groups for PCP pneumonia include
Premature infants
Patients with immunodeficiency diseases, including severe combined immunodeficiency disease (SCID) and acquired immunodeficiency syndrome (AIDS).
Patients receiving immunosuppressive drugs, especially cortisone-like drugs (corticosteroids)
Patients suffering from protein malnutrition. PCP is found in countries with widespread hunger and poor hygiene.
Drug Addiction at: microrao dot com/micronotes/mycology.pdf
Funny, my wife said the same thing about you when she just read your comment.
Argument from authority. The "consensus " believes it, therefore it must be true.
These are Ad Hominem attacks. The qualifications were perfectly fine. Any Emergency Room MD is qualified as an expert witness to testify in a court of law, and give their opinon about HIV /AIDS. What do you think they do all day? I will spell it out for you. They order blood tests for HIV, and discuss the results and treatment recommendations with the patients. Why would a hospital employ them, and why would any patient trust them or listen to them if they weren't qualified?
And what made this Elk Horn Head a legal expert. I bet he couldn't get out of a parking ticket without hiring a lawyer. The legal system and the Parenzee trial has nothing to do with the reality that AIDS science is in a shambles. Numerous mistakes have been made resulting in deaths of hundreds of thousands from AZT, and now the newer hiv drugs are killing people with liver failure and stevens johnson syndrome. There is still no mechanism of disease, no animal model, no gold standard for the HIV test kits, no occupationally acquireed AIDS ( No report in the Brazilian medial literature of occupatinally acquired AIDS until a single one after 200,00 AIDS cases were treated.)
If Elk Horn's appeal to authority without any rational basis is expected to convince anyone to trust the medical system after a series of betrayals with death by AZT and the Dr Ho mistakes, Mr. Elk Horn Mountain Man will be sadly disappointed, as a matter of fact, he can take his toxic Hiv drugs and self administer them as a rectal suppository. Heck, a non-toxic selenium pill for a nickle does better than any of the toxic HIV drugs, and it wont kill you like they do (1).
Instead of going on a rant which essentially appeals to some authority you imagine you have and dont, why don't you rationally take a few minutes to explain in very simple teminology the mechanism of disease, how HIV causes Aids, using a few references in the medical or science literature along the way. We are waiting Mr. Elk Horn Head .
(1)Suppression of Human Immunodeficiency Virus Type 1 Viral Load With Selenium Supplementation, A Randomized Controlled Trial, Barry E. Hurwitz, PhD Arch Intern Med. Jan 27, 2007;167:148-154.)
denialists have proven themselves again and again to be sociopaths: religious extremists, the political fringe (left and right), racists, homophobes, the conspiracy-obsessed, quack profiteers off the misery of their fellow humans, plagiarists, pedophiles (Elkmountainman)
Elkie,
Word is they're looking for somebody over at AIDStruth to author their next science feature. Its working title is,
Duesberg and Paedophilia: Why HIV Causes AIDS
Maybe it would be something for you and your charming wife?
You can go here to learn more about what kind of scientific and literary standards are expected: http://aidstruth.org/duesberg-homophobia.php
You research steel building beams (I saw that, as an assistant professor in Australia, you have first authored 4-5 papers on the subject during your career)?
Unlike you I have never made an appeal to my own authority. What I can do is go to the library and read the papers that you cite and check whether they support your claims.
This is what I have done. Your "quotation" :The Veterans Affairs Cooperative Study Group reported that "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians," [1] one can't ignore it. is not found in the article that you cited. the only place that it can be found is in an online comment by somebody using "Robert Gallo" as a pseudonym.
Quotation marks are meant to indicate a direct quote from the authors not your own misinterpretations. This isn't just some quaint tradition. It's about basic honesty and integrity.
You have consistently misrepresented the studies that you claim support your position. In at least two cases you have fabricated quotes.
Because you have shown such deep insight in this (as well as countless other blogs) on the subject of AIDS, and I am assuming this is you I found, and you are not by chance the Chris Noble of Hamilton Heights High School Fine Arts Department Head, who commented on Ryan White's funeral, could you please speculate using your first-hand knowledge of human diseases and pathology as to the causes of:
Are there any scientists that claim to know the exact causes of all of these diseases (apart from Hulda Clark)?
The statement," AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians" happens to be a true statement, Dr Chris Noble, so get off your hobbyhorse and get down to business. It doesn't have to originate from a quote from another author or paper anywhere, because it happens to be true. Get out there and sell your toxic HIV drugs, so that abortions can be induced in pregnant women, and impoverished malnourished black and hispanic drug addicts, homosexuals and other undesirables can be eliminated from society by a silent iatrogenic genocide of toxic drugs while the watchdogs slumber.
The statement," AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians" happens to be a true statement, Dr Chris Noble, so get off your hobbyhorse and get down to business. It doesn't have to originate from a quote from another author or paper anywhere, because it happens to be true. Get out there and sell your toxic HIV drugs, so that abortions can be induced in pregnant women, and impoverished malnourished black and hispanic drug addicts, homosexuals and other undesirables can be eliminated from society by a silent iatrogenic genocide of toxic drugs while the watchdogs slumber.
When somebody cites a paper and gives a quote in quotation marks it is supposed to be an actual quote from the authors of the paper.
It is imperative that when you make scientific claims you present evidence to support them. In the case of HIV Denialists they do no research of their own and hence they are reduced to sifting through the literature to find evidence from "orthodox" studies. If they do this it is imperative that you accurately report the findings of that research. What is seen in HIV Denialism is that the results of "orthodox" studies are frequently misrepresented or distorted in an attempt to find evidence for their claims. In the worst cases quotes are fabricated.
Your assertion that it's OK to fabricate quotes and falsely attribute them to "orthodox" scientists because the have "truthiness" is delusional.
No, your right. The Gallo quote pertaining to the paper he described, actually said, and I defend Gallo's statement:
1. "In symptomatic patients with HIV infection, early treatment with zidouvdine delys progression to AIDS, but in THIS controlled study, it did NOT improve survival, and it was associated with MORE side effects."
WHAT THIS MEANS TO ME IS THAT THIS IS A DANGEROUS WORTHLESS DRUG, UNLESS YOU KNOW SOME OTHER MEANING FOR "DOESN'T IMPROVE SURVIVAL AND IT WAS ASSOCIATED WITH MORE SIDE EFFECTS?"
2. "There were 43 deaths, 23 in the early-therapy group, and 20 in the late-therapy group." "EARLY THERAPY" MEANS THAT THE PATIENTS ARE NOT DEEMED AS SICK AS THE "LATE THERAPY" PATIENTS (EARLY IN DISEASE-LATE IN DISEASE-GET IT)? HEALTHIER PATIENTS DIED QUICKER.
3. "Thus all 10 of the deaths that were not preceded by or associated with an AIDS-defining event occurred in the early-therapy group" (WHO WERE SUPPOSEDLY HEALTHIER SINCE THAT IS WHAT EARLY THERAPY GROUP MEANS).
4. "The medium time from the diagnosis of AIDS to death was 16 months in the early therapy group, and 19 months in the late-therapy group." AZT KILLS HEATHIER PEOPLE FASTER THAN SICKER PEOPLE?
5. "The racial and ethnic groups appeared to respond differently to the timing of zidpovudine therapy. Fewer minority (African American and Hispanic) patients died in the late therapy group (two deaths) than in the early-therapy group (nine deaths), but the difference was not significant." (2 versus 9 deaths not significant?). MORE OF THE HEALTIER AFRICAN AMERICANS DIED AS A RESULT OF AZT THAN THE SICKER ONES. TI'S A MIRACLE DRUG.
6. "Among non-Hispanic (they mean Non-African American or Native American) white patients, early therapy significantly delayed the onset of AIDS BUT HAD NO EFFECT ON SURVIVAL" (TABLE 3-CAPITALS MINE). WHAT THIS MEANS TO ME IS THAT IT'S OK TO GIVE THEM DIARRHEA, VOMITING, ANEMIA, CANCER (READ THE PACKAGE INSERT), ETC., AND THEY DIE AT THE SAME TIME.
7. "Minority patients were much more likely than white patients to be intravenous drug users (40% vs. 10%)." MORE SIGNIFICANT THAN 2 LATE-TREATMENT AFRICAN AND HISPANIC AMERICAN DEATHS VERSUS 9 AFRICAN OR HISPANIC AMERICAN DEATHS I SUPPOSE?
8, " Changes in CD4+ counts from base-line values showed clear differences between treatment groups over time." WHICH MEANS THAT THIS MARKER HAS NOTHING TO DO WITH DEATH FROM AIDS SINCE:
"it did NOT improve survival, and it was associated with MORE side effects."
9. " After two years of follow-up, we found no difference in survival between the two treatment groups (BECAUSE THE GODDAMN CANCER DRUG DOESN'T WORK)!
10. "In patients who received early treatment we found a significant reduction in progression to AIDS, a finding that complements those of the placebo-controlled studies conducted by the AIDS Clinical Trials Group in symptomatic and asymptomatic patients (2,3)" (these are the Fischl and Volderding 1990 Studies Dr. Hamilton is referring to).
A REDUCTION IN PROGRESSION TO AIDS, YES, UNLESS YOU ARE BLACK OR HISPANIC AND TREATED EARLY:
"Fewer minority (African American and Hispanic) patients died in the late therapy group (two deaths) than in the early-therapy group (nine deaths), but the difference was not significant." BECAUSE IT ISN'T SIGNIFICANT IF YOU ARE BLACK OR HISPANIC?
I Guess this is why Gallo posted the quote on that website as I copied it:
"The Veterans Affairs Cooperative Study Group reported that "AZT disproportionately harmed Blacks and Hispanics, and provided no benefit to the quelling of advancing immune suppression in Caucasians," [1]
Noble said:
"the only place that it can be found is in an online comment by somebody using "Robert Gallo" as a pseudonym."
How do you know it is a pseudonym? Have you asked him how he feels about AZT these days? I know he doesn't think much of the vaccine...
Gallo himself, in the pages of Science, after the so-called failure of the 120 million dollar AIDSVAX program was announced, suggesting that:
"A sound Rationale (is) needed for Phase III HIV vaccine trials."
Also, in this Science article, the AIDSVAX trials were criticized by Gallo and his co-authors because they were from the beginning, a colossal waste of time, money, but most of all, as Gallo warns in the last sentence of the letter to Science, the trials are potentially damaging for the credibility (and future funding) of the HIV=AIDS paradigm:
"The decision about whether or not to proceed with mounting a phase III HIV-1 vaccine trial needs to take into account the likelihood of success and the consequences of failure, the value of what can realistically be learned, the human and financial costs involved. As a whole, the scientific community must do a better job of bringing truly promising vaccine candidates to this stage of development and beyond. More highly immunogenic HIV-1 vaccines that offer a greater hope of success than the ALVAC-gp120 combination are, in fact, now in early-phase clinical trials." (Gallo and others, Science, Vol 303 16 January, 2004).
Dr Maniotis, I agree with previous posters on this thread - you are a disgrace to the name of science. No matter how you try and lie about it, the VA study group did not report what you say it did.
Every "justification" you have pointed to in the VA study for your quote invention is based on a distortion or misinterpretation of the study results.
You have been found out several times manufacturing "quotes" out of thin air, and seem totally unrepentant. You seem quite comfortable with using your own words as quotes from another source, because you feel that's what they "should have" said.
If you feel this is acceptable, then I guess you will have no problem with this innacurate statement:
Dr Andrew Maniotis has freely admitted inventing quotations from scientific papers. On the Aetiology blog, he said "I have frequently lied about what authors have found in their studies. I do this in order to prop up my own ridiculous and disproven theories about AIDS".
Presumably we can now attribute this quote to you and spread it across the internet with impunity, safe in the knowledge that this is what I feel you "should" have said, even if you didn't.
Andrew,
I think I might detect some minor progress on your part with respect to your "integrity-challenged" quotes of the scientific work of others. Twice in this thread you've referred to the "last sentence" of a paper you cite as: Gallo and others, Science, Vol 303 16 January, 2004. (The correct citation is: Burton et al. (2004). A Sound Rationale Needed for Phase III HIV-1 Vaccine Trials. Science 303:316)
The first time you referred to "the last sentence" of this article you managed to omit the last sentence:
You made the same omission in your "The ABC's of AIDS Denialism," from which you pasted this passage. I wonder how many other inaccurate quotes you published in that essay? Have you ever counted them?
On July 2, you again pasted this passage into the thread, but this time you actually added back the last sentence!! And you did so before anyone pointed out your omission. That's big progress for you. On the other hand, you didn't alert the readers to your previous inaccurate quote, but no one's perfect.
Keep up the mantra. I think it may be helping:
franklin was they guy who DENIED that Ariel Glaser ever took AZT.
.
Now, that's real AIDS denial.
You guys gang up on Dr. Maniotis because you cant attack the larger arguments, and like corrupt defense lawyers are trying to get off on a technicality.
Montagnier meant what he said, he conducted expirements that showed that hiv didnt kill cells, and thats why he said in 1990 that HIV might be benign. He blamed cofactors, mycoplasma incognitus, and still does as of 2000 in his book Virus.
Andrew Maniotis is a university professor at the U of Illinois Chicago who knows very well that he is telling lies about HIV, AIDS and vaccination. He get's "ganged up on" because he tells lies sometimes and other times just distorts or misrepresents the truth.
Some people, such as HIV-infected individuals who have no science training, have very good reasons for being deluded into believing that HIV does not exist or is harmless. Andrew Maniotis has no such excuse, he knows very well that he is lying.
Unless PS Duke can back up his statements with facts, Duke himself is obviously lying.
Doctor of What? Lyology of course.
Andrew,
Why does it seem like every time someone tries to track down one of your "quotes" from the scientific work of others--the "quote" turns out to be inaccurate? Here's the latest one:
Previously in this thread you also referred to Barre-Sinoussi's presentation:
In "The ABC's of AIDS Denialism" (from which you pasted the "quote") you provide the following reference for the "quote":
http://www.aids2006.org/PAG/PSession.aspx?s=653
This link takes us to the program of the XVI International AIDS Conference, and although the quoted sentence appears on the web page, it was not written or spoken by Barre-Sinoussi. Instead, it was written by Cheryl Baxter, a "Rapporteur" who summarized the day's talks for the web site. Her blurb on Barre-Sinoussi's talk included some more information that you chose to omit:
Again, you misattribute a quote. Barre-Sinoussi never spoke the words that you "quote" her as saying. A link to a video file of her talk is provided on the web page. You might consider watching it some time.
You not only misattribute the quote, but (again) you draw false conclusions from your false "quote". Nowhere does Barre-Sinoussi (or even Baxter) state the conclusion you attribute to Barre-Sinoussi: namely that the vaccine trials "have not evoked humoral, cellular, or mucosal immunity, or demonstrated T-cell activation to date." In fact, they say the opposite. Barre-Sinoussi discusses (and Baxter alludes to) a randomized trial of a therapeutic HIV vaccination strategy in which the vaccination elicited specific CD4 and CD8 T-cell responses and decreased viremia, and the T-cell responses were strongly correlated with prolonging the time that patients could remain off HAART therapy.
Once again you falsely attribute a conclusion to another scientist, and once again your conclusion is the opposite of what the scientist actually said.
The people Like Dr mantious do not prevent others from hearing other sides of arguments and do not prevent others from hearing another side of issues. They are quite willing for people to be exposed to both sides of an issue and have the public decide on their own.
The orthodoxy operates with complete censorship and lies by omission, and are too scared to defend their views publicly, and rely on the "peer review" process, which are usually manned by gatekeepers who mindlessly parrot the CDC's and drug companies propaganda, and refuse to publish anything that opposes the establishments propaganda.
These tactics were used in many oppresive societies in the past. For example in Russia during communism or Germany during Facsism the propaganda of the state corrupted the scientific process.
For example if you were an economist in Russia and you wanted to publish in an academic journal that Stalins economic policies were whack, you would never be able to do so, and if you managed to make a challenge to the orthodoxy you would be attacked as a "charlatan"
Why does mainstream medicine today rely on uninformed consent?
Why do they never reveal that Vaccines in the early 90's had 100 times the daily EPA's safe limit of mercury, and the flu shots today still exceed the limit by many times?
Why dont they mention the many people who recently took Gardisil and immediately after had serious advserse effects as uncovered by judicial watch in complaints to the FDA?
That microbes like HPV have totally failed Kochs postulates and some scientists believe that cervical cancer is more complicated than HPV?
That AZT is a chemotheraputic drug that damages the mitochondria? Dont people have a right to know they are being put under long term chemotherapy?
That some scientists think that the lack of a reliable animal model and the fact that HIV is only in small fraction of tcells means that the case on HIV warrants further study?
The whole system relies on only telling patients one side of the story to control them and destroy their lives. It denies Americans informed consent to make important decisions that effect their own bodies and thier own health. It's a complete disgrace.
Cooler, there are many more than "two sides" to EVERY story. There are at least 700 "sides" to the HIV/AIDS story.
Do some homework.
I agree, let the public hear all sides and decide accordingly
Cooler, you say that the scientific orthodoxy is censoring debate. But what about denialist sites like You Bet Your Life and AIDSmythExposed that have a virulent dislike for any orthodox views being expressed on their sites and block posters?
The existence of blogs like Tara's, where dissidents have even showered vitriol on her by calling her things like a suppurating pustule, and where regular comparisons with Nazis are used as terms of abuse, and where other ad homs are regularly employed rather than any attempt to engage in civil debate, prove there is no "censorship" that you speak of.
If you refer to the fact that dissidents don't get theri theories into the published literature, then the answer is pretty obvious and there is no need to talk of censorship or conspiracies.